
Abstract
Background:
Trauma center and multidisciplinary management protocols have been proven to improve the outcomes of severely injured patients. Hemorrhage from pelvic injury is associated with high mortality and is a common cause of preventable trauma death. This study aimed to evaluate the effects of the establishment of a trauma center and management protocols on the outcomes of hemodynamically unstable patients with pelvic fractures.
Methods:
Hemodynamically unstable patients with pelvic fractures were reviewed retrospectively over a 10-year period. They were grouped into the pre-phase and post-phase, which were defined as before and after the establishment of a trauma center and protocols, respectively. Basic characteristics and outcomes were compared between periods.
Results:
This study enrolled a total of 106 patients. Basic and physiological characteristics were not significantly different in both phases. Pre-peritoneal packing and resuscitative endovascular balloon occlusion of aorta were only performed in the post-phase (pre-peritoneal packing, N = 27; resuscitative endovascular balloon occlusion of aorta, N = 10). In the post-phase, the time from emergency department arrival to hemostatic intervention was significantly shorter (269 ± 132.4 min vs 147.2 ± 95.5 min, p < 0.0001), and mortality due to acute hemorrhage was significantly lower (p = 0.003; absolute risk reduction: 0.22; relative risk reduction: 0.72). Multivariate logistic regression analysis identified age, injury severity score, and the pre-phase as independent risk factors for mortality.
Conclusion:
The establishment of a trauma center and multidisciplinary management protocols, such as pre-peritoneal packing and resuscitative endovascular balloon occlusion of aorta, improved the outcomes of hemodynamically unstable patients with pelvic fractures.
Introduction
Trauma is a leading cause of death for young people in Korea. According to Statistics Korea, the rate of trauma deaths was 65.4 per 100,000 in 2010. 1 This rate gradually decreased to 51.5 in 2020 but is still high. Globally, the unintentional injury death rate was highest in the Southeast Asian region (80 per 100,000) and lowest in the American region (39 per 100,000) in 2010. 2
The rate of preventable deaths in Korea is reportedly decreasing but still higher compared with those in developed countries.3,4 Therefore, the Ministry of Health and Welfare and medical professionals decided to establish regional trauma centers in 2012. The first regional trauma center opened in 2014, with plans to establish a total of 17 regional trauma centers in Korea by 2021. Several changes may be observed after the establishment of a trauma center, such as an increase in the volume of trauma cases in the center, trauma-dedicated resources, performance improvement programs (PIPs), or the development of a regional trauma system.
The mortality rate of hemodynamically unstable patients with pelvic fractures remains greater than 30% despite advancements in the management of severely injured patients.5–8 Furthermore, it is also one of the most frequent contributors to traumatic preventable death. 9 Therefore, management strategies for these patients, including initial resuscitation, diagnosis, and therapeutic interventions, are essential in reducing mortality. The majority of trauma centers emphasize angioembolization (AE) as an effective intervention to stop pelvic bleeding, although AE cannot address venous or bony hemorrhage within the pelvis.10,11 Approximately 85% of bleeding due to pelvic fractures is known to be of venous or bony origin. Therefore, the initial approach should achieve hemostasis in the retroperitoneal space through a pelvic binder or pre-peritoneal pelvic packing (PPP).11,12 The utilization of AE needs a proper facility, equipment, and human resources. It is well known that time to hemorrhage control is related to mortality, but it typically takes around 2–5 h before AE is performed at many centers.7,8,13,14
PPP with external pelvic compression reportedly stops hemorrhage and facilitates other emergent operative procedures.11,15 We included pelvic binders, PPP, external pelvic fixation (EPF), and AE in the pelvic fracture management algorithm after the establishment of a trauma center in 2014 and added resuscitative endovascular balloon occlusion of aorta (REBOA) to the management algorithm in 2016. 16 The aim of this study was to evaluate the time to intervention and the outcomes of hemodynamically unstable patients with pelvic fractures before and after the establishment of a trauma center and management protocol. We hypothesized that the establishment of a trauma center and protocols, including interventions such as PPP and REBOA, would shorten the time to intervention and reduce mortality at our institution.
Materials and methods
Setting
The Gachon University Gil Medical Center is a 1500-bed teaching hospital in Incheon, South Korea, that serves a population of 3 million people. The regional trauma center was established in 2014 in accordance with the trauma system development plan of the Ministry of Health and Welfare. Before 2014, the emergency center managed trauma patients without a dedicated trauma surgeon, trauma team, dedicated facilities, or protocols for the evaluation and management of pelvic injuries. There were more than 3000 trauma-related admissions, of which 500–550 patients presented with major trauma (injury severity score (ISS) > 15). The regional trauma center is equipped with a trauma bay, 2 operating rooms dedicated to trauma, a 20-bed trauma intensive care unit, and a trauma angiography suite. These facilities are reserved for trauma patients only. A hybrid operating room was also prepared for simultaneous endovascular intervention and open surgery. Fourteen full-time trauma surgeons currently work at the center and a team of emergency physicians, anesthesiologists, and radiologist consultants are available 24/7. Improvements after the establishment of the center are summarized in Table 1.
Structural elements of Korean Regional Trauma Center.
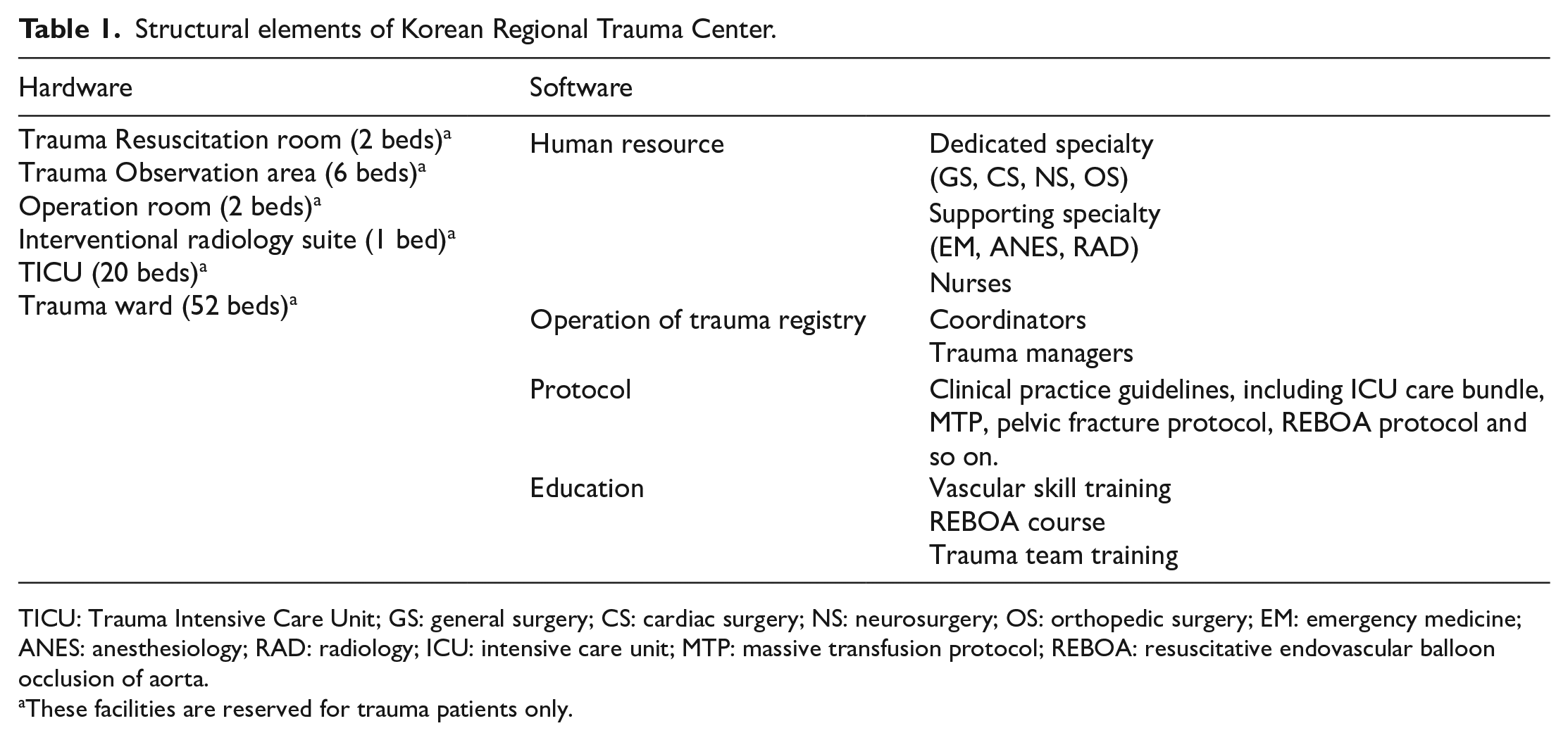
TICU: Trauma Intensive Care Unit; GS: general surgery; CS: cardiac surgery; NS: neurosurgery; OS: orthopedic surgery; EM: emergency medicine; ANES: anesthesiology; RAD: radiology; ICU: intensive care unit; MTP: massive transfusion protocol; REBOA: resuscitative endovascular balloon occlusion of aorta.
These facilities are reserved for trauma patients only.
Since the establishment of the trauma center, efforts have been made to establish various protocols at the institution. The pelvic bone fracture algorithm and massive transfusion protocol (MTP) were established through a multidisciplinary conference including trauma department staff, emergency department (ED) staff, a laboratory medicine physician, and a medical laboratory scientist. The MTP includes emergency transfusion within 15 min, a specified blood product ratio (a 1:1:1 ratio of packed red blood cells (pRBCs) to fresh frozen plasma (FFP) to platelets), and the use of tranexamic acid.
Study population
The study included hemodynamically unstable patients with pelvic fractures from January 2009 to December 2018. Non-responders were defined as having a systolic blood pressure (SBP) < 90 mmHg during the initial resuscitation despite the transfusion of 2 units of pRBCs. We excluded patients who died in the ED or from out-of-hospital cardiac arrest, patients < 16 years old, patients without interventions to control pelvic bleeding (PPP, REBOA, AE, and EPF), and those who received delayed interventions after the treatment of other injuries. The outcomes of the enrolled patients were analyzed by time period; the pre-phase and post-phase were defined as before and after, respectively, the establishment of the trauma center and protocols.
Protocol
During the pre-phase, patients with pelvic injuries were initially evaluated and managed at the ED by emergency physicians. After evaluation and initial resuscitation, the general and orthopedic surgeons on call decided on further management plans. AE was mainly performed if extravasation of contrast was seen on computed tomography. Pelvic circumferential compression devices or external fixations were not utilized in this phase. There was no protocol for the management of bleeding pelvic fracture patients.
During post-phase, severely injured patients were managed at the trauma bay by a trauma team utilizing dedicated facilities. Patients with bleeding pelvic fractures were managed according to a previously published algorithm (Figure 1). If pelvic bone fracture was diagnosed in portable X-ray, application of pelvic binder was considered. Patients who tested positive for abdominal fluids on focused assessment with sonography for trauma (FAST) were brought to the operating room for both laparotomy and PPP. EPF was performed following the operation if the corresponding personnel were available. If patients remained hemodynamically unstable despite PPP, AE was then performed. For patients with negative FAST results, AE was attempted first. However, if AE was not immediately available, or the patient was hemodynamically unstable while waiting for AE, PPP was performed as a first choice. Since 2016, we have implemented REBOA in the algorithm for extremely unstable patients.
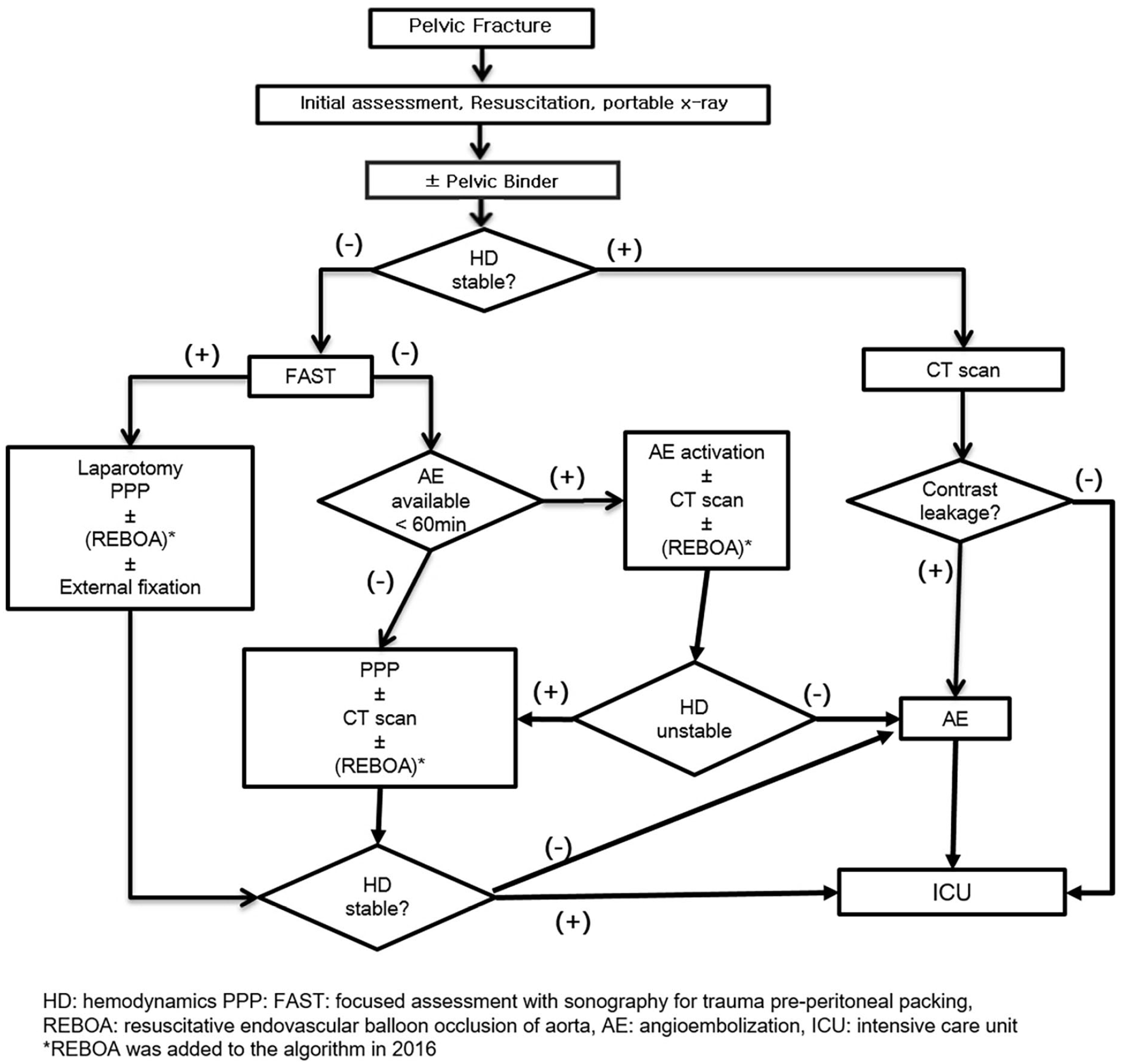
An algorithm for the management of pelvic fracture.
Statistical analysis
Numerical data were presented as the means and standard deviations, whereas categorical data were presented as percentages. The normality test showed a normal distribution of the data. The univariate analysis was performed using the Student’s t test and chi-square test. Covariables with significance in the univariate analysis were analyzed in a multivariate regression model. Multivariable logistic regression was utilized to evaluate independent risk factors for mortality. Statistical significance was defined as p < 0.05. All statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA).
Results
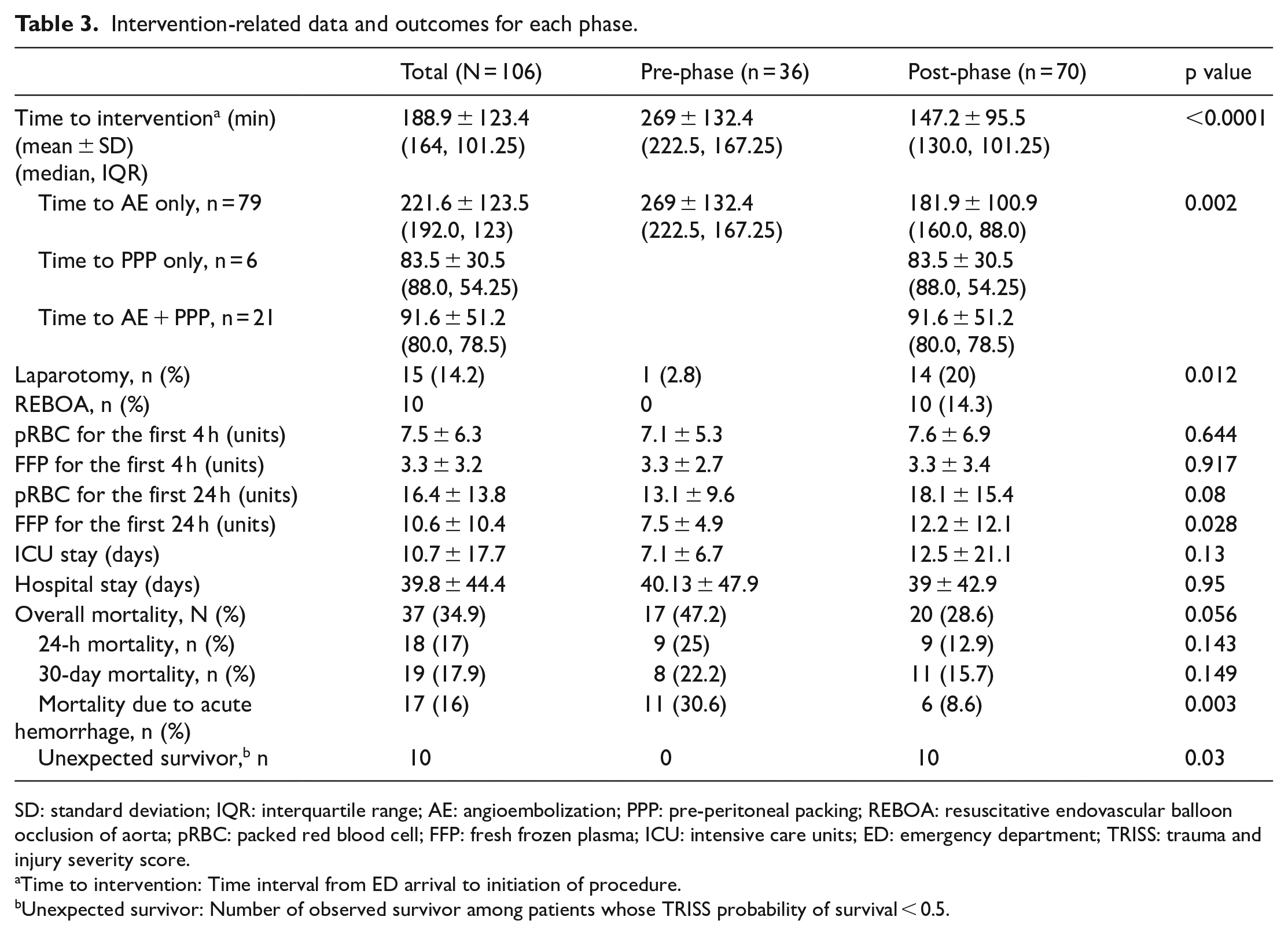
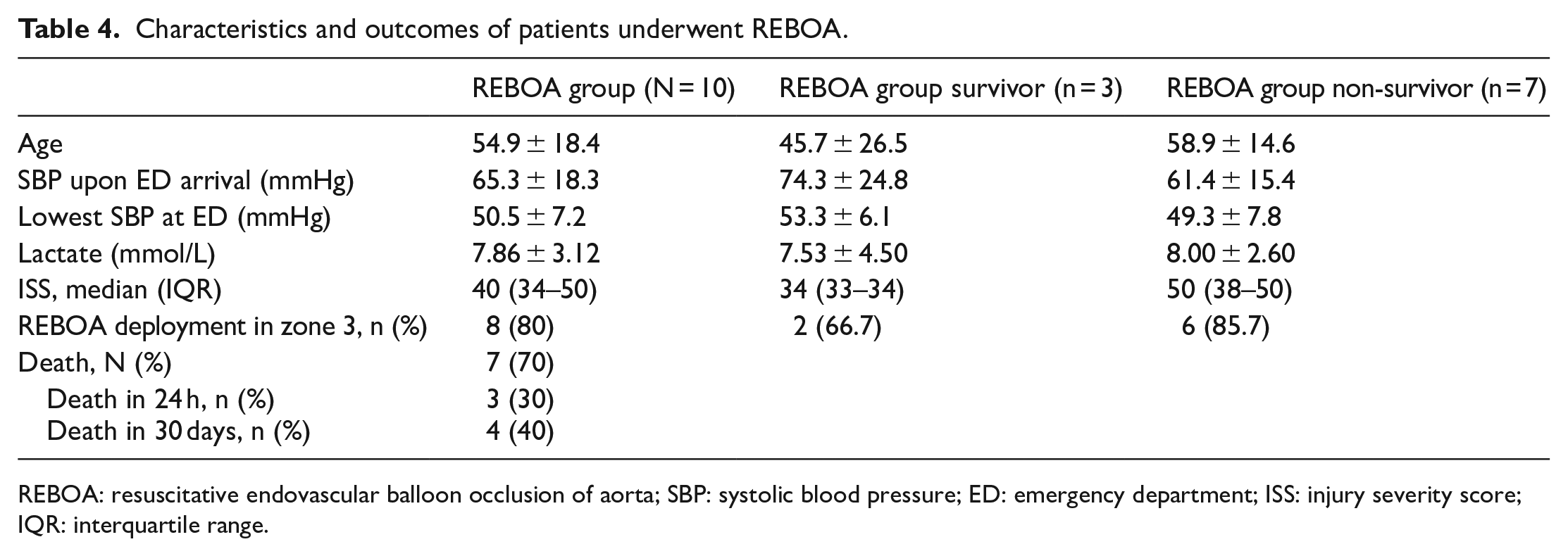
We extracted data from 1469 patients with an Abbreviated Injury Scale (AIS) pelvis score over 1 point from the trauma center database. A total of 106 (7.2%) patients met the inclusion criteria of the current study (Figure 2). The mean age of patients was 52.3 ± 19.8 years and 53 (50%) of the patients were male. Demographic data indicated a mean SBP at ED admission of 83.5 ± 29.2 and the lowest SBP at ED of 60.4 ± 25.7 mmHg. Median values of the Glasgow Coma Scale (GCS) and ISS were 15 (interquartile range (IQR) = 9–15) and 38 (IQR = 32–50). The basic demographics of both groups were statistically similar (Table 2). The mean amounts of pRBC and FFP transfusion for the first 24 h were 16.4 ± 13.8 units and 10.6 ± 10.4 units, respectively. The mean amount of FFP transfusion for 24 h significantly increased from 7.5 ± 4.9 units to 12.2 ± 12.1 units in the post-phase (p = 0.028). The mean time to intervention (for PPP, AE, or both) was 269 ± 132.4 min in the pre-phase and 147.2 ± 95.5 min in the post-phase (p < 0.001). The mean time to AE only was also significantly shorter in the post-phase (p = 0.002). The time to intervention decreased over the study period (Figure 3) and REBOA was performed only in the post-phase for 10 patients. The overall mortality rate of the study population was 34.9%, with a decrease from 47.2% in the pre-phase to 28.6% in the post-phase (p = 0.056). The mortality rate associated with acute hemorrhagic shock also decreased from 30.6% in the pre-phase to 8.6% in the post-phase and it was statistically significant (p = 0.003; absolute risk reduction: 0.22; relative risk reduction: 0.72). Acute hemorrhagic shock is a type of hypovolemic shock caused by a pelvic fracture. There were no trauma and injury severity score (TRISS) unexpected survivors (TRISS probability of survival < 0.5, TRISS coefficients 2009 revision) in the pre-phase, but there were 10 (24%) unexpected survivors in the post-phase (Table 3). Patients who underwent REBOA had lower SBP and higher lactate levels and ISS than those who did not. In eight patients, REBOA balloon was deployed in zone 3. Seven patients survived for more than 24 h and three patients survived until discharge (Table 4).
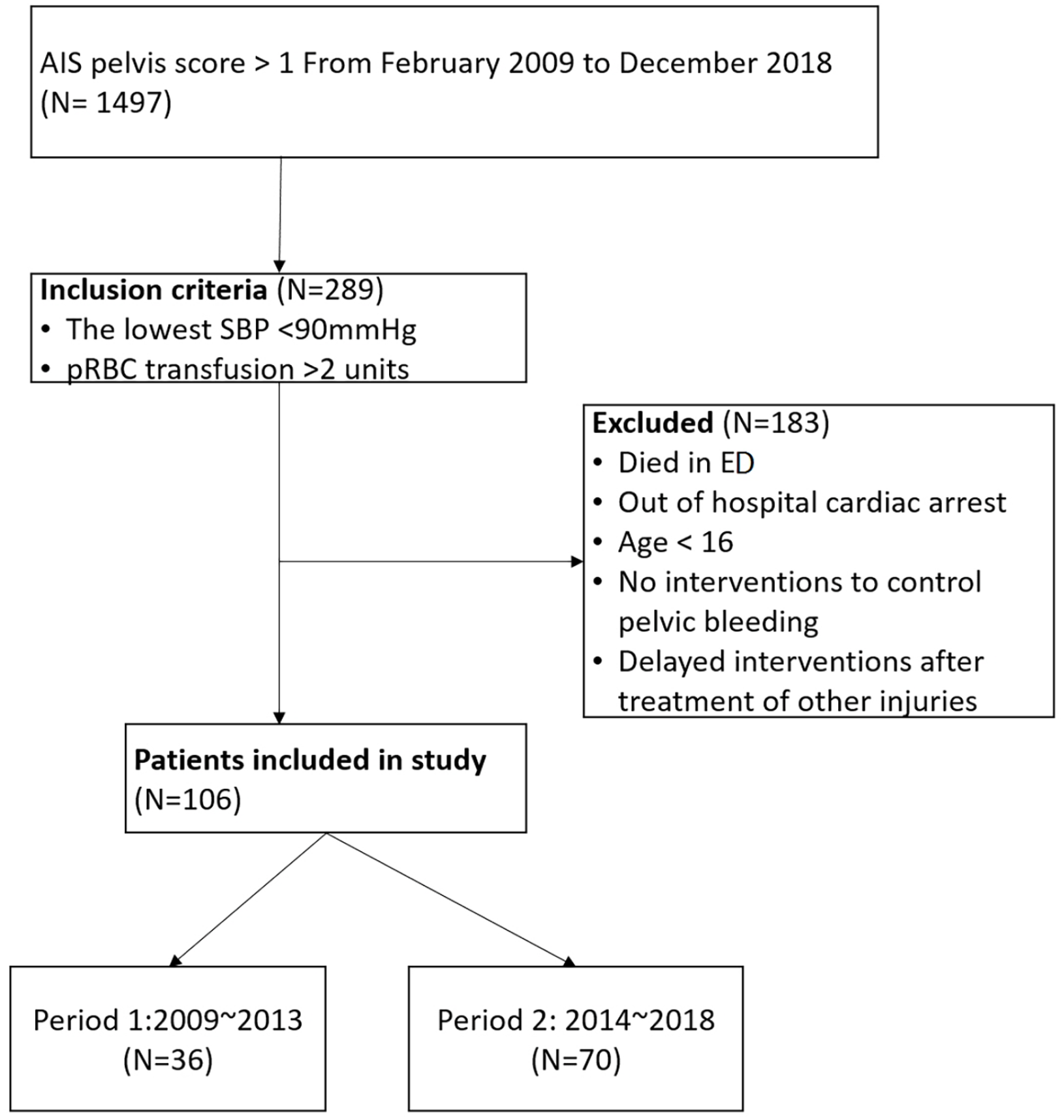
Flowchart of patient inclusion.
General characteristics of all patients managed in the pre-phase and post-phase.
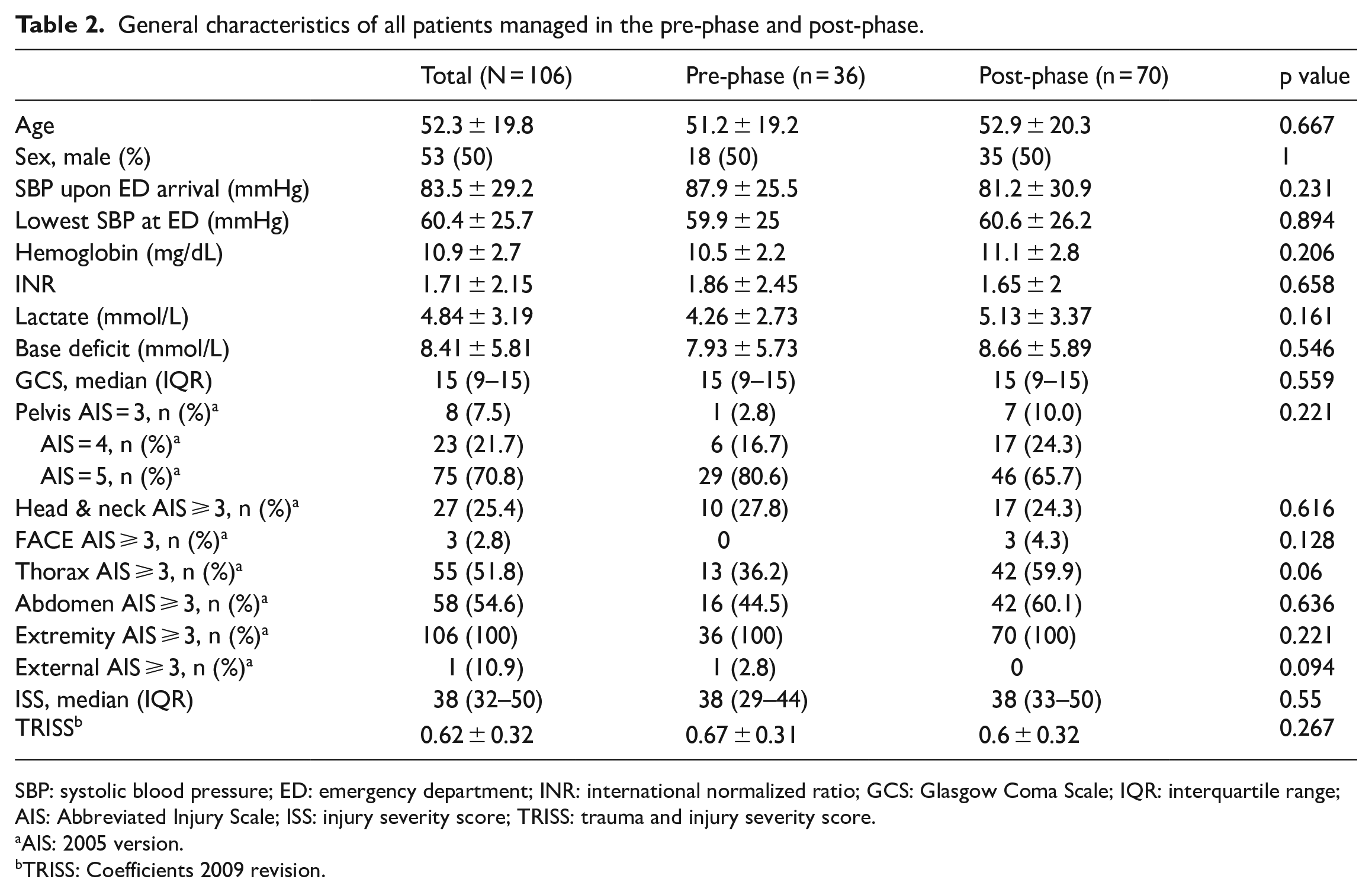
SBP: systolic blood pressure; ED: emergency department; INR: international normalized ratio; GCS: Glasgow Coma Scale; IQR: interquartile range; AIS: Abbreviated Injury Scale; ISS: injury severity score; TRISS: trauma and injury severity score.
AIS: 2005 version.
TRISS: Coefficients 2009 revision.
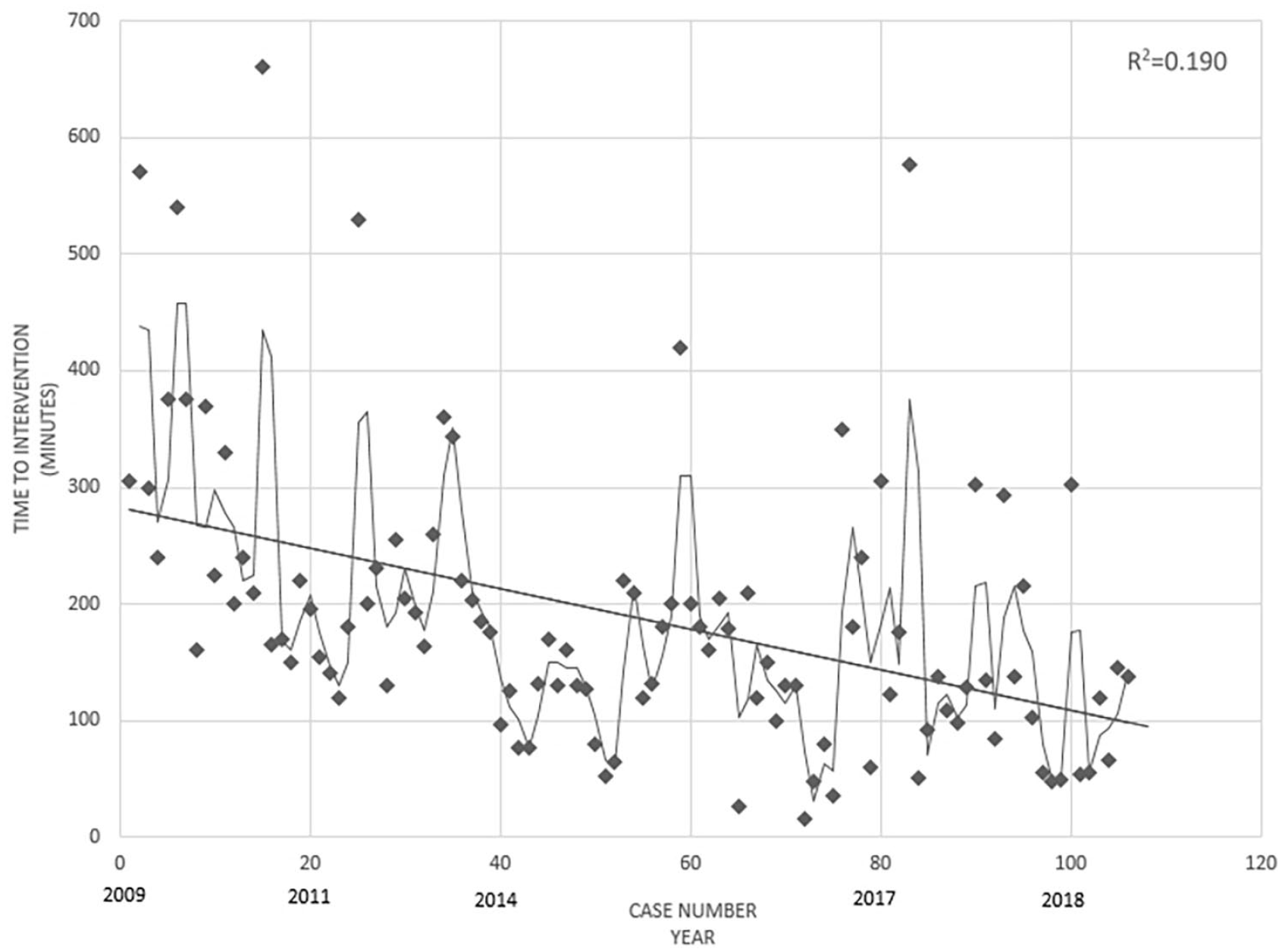
Time from the emergency department to intervention throughout the study period.
Intervention-related data and outcomes for each phase.
SD: standard deviation; IQR: interquartile range; AE: angioembolization; PPP: pre-peritoneal packing; REBOA: resuscitative endovascular balloon occlusion of aorta; pRBC: packed red blood cell; FFP: fresh frozen plasma; ICU: intensive care units; ED: emergency department; TRISS: trauma and injury severity score.
Time to intervention: Time interval from ED arrival to initiation of procedure.
Unexpected survivor: Number of observed survivor among patients whose TRISS probability of survival < 0.5.
Characteristics and outcomes of patients underwent REBOA.
REBOA: resuscitative endovascular balloon occlusion of aorta; SBP: systolic blood pressure; ED: emergency department; ISS: injury severity score; IQR: interquartile range.
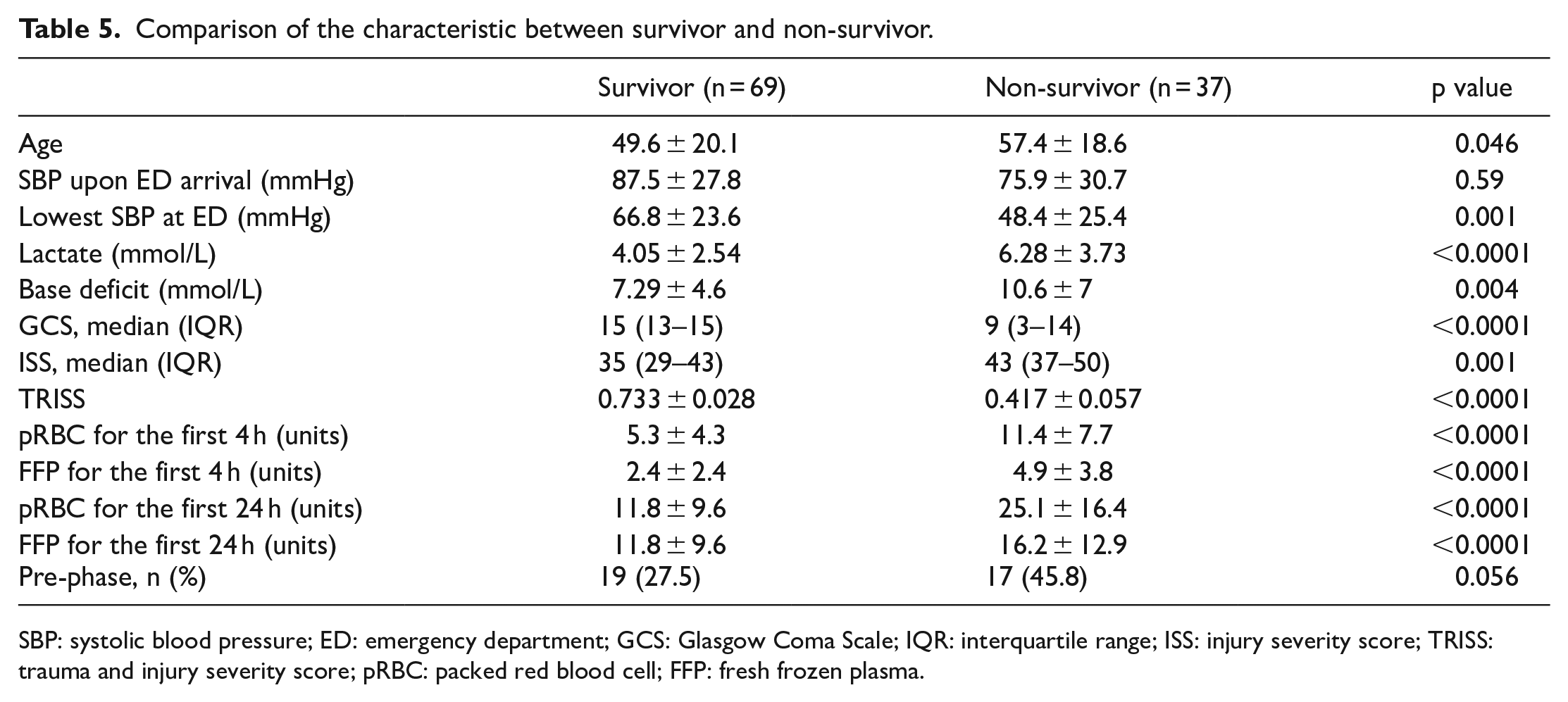
Patients who survived were found to be significantly younger (49.6 ± 20.1 vs 57.4 ± 18.6 years, p = 0.046) and have higher SBP (66.8 ± 23.6 vs 48.4 ± 25.4 mmHg, p = 0.001), GCS, and TRISS, with lower ISS, lactate levels, base deficit, and transfusion amounts (p < 0.001) (Table 5).
Comparison of the characteristic between survivor and non-survivor.
SBP: systolic blood pressure; ED: emergency department; GCS: Glasgow Coma Scale; IQR: interquartile range; ISS: injury severity score; TRISS: trauma and injury severity score; pRBC: packed red blood cell; FFP: fresh frozen plasma.
A multivariate logistic regression analysis evaluated the independent risk factors for mortality as listed in Table 6. After adjusting for age, sex, base deficit, lactate, ISS, TRISS, and transfusion amounts, the following variables were found to be significantly associated with overall mortality: age (odds ratio = 1.19; 95% confidence interval (CI) = 1.04–1.35), ISS (odds ratio = 1.16; 95% CI = 1.02–1.32), and the pre-phase (odds ratio = 13.4; 95% CI = 3.02–59.89).
Logistic regression analysis of the independent risk factors of mortality.
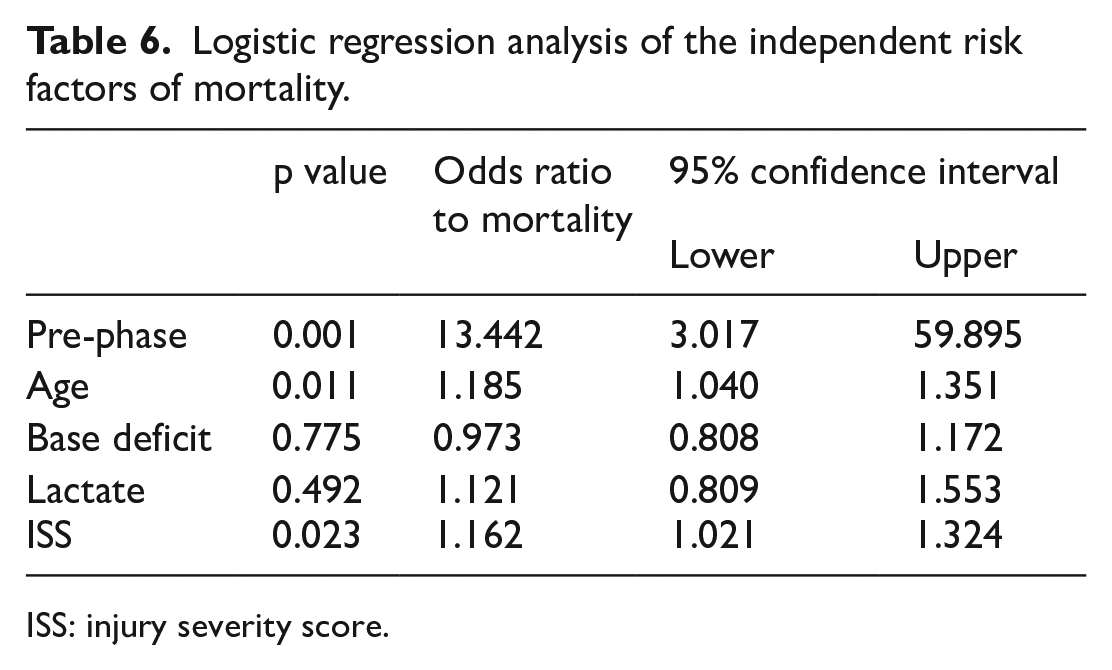
ISS: injury severity score.
Discussion
Trauma center establishment has been associated with reduced mortality in several studies and it is mainly due to increased annual trauma volume, trauma-dedicated resources, and PIPs.17–19 Before the establishment of a regional trauma center, approximately 250 severely injured patients (ISS > 15) were admitted to our hospital annually. However, after the trauma center opened in 2014, more than 500 severely injured patients have been managed annually. Previous research has shown that establishing a trauma center and centralizing the care of severely injured patients may lead to better outcomes. 20 With the establishment of the center, we shared and educated paramedics on guidelines for severely injured patients. Therefore, the volume of trauma patients and the rate of direct transportation have increased from year to year. 21 Furthermore, the presence of human resources (trauma-dedicated surgeons, nurses, and a trauma program manager) and a PIP could influence resuscitation practice, time to intervention, and hemorrhage control modalities. 10
Bleeding pelvic fractures are uncommon but are associated with significant mortality due to hemorrhagic shock. Before the establishment of a trauma center, hemodynamically unstable patients with pelvic fractures were managed mainly by an emergency physician in the initial resuscitation phase. After the diagnosis of a bleeding pelvic fracture was confirmed using imaging studies, general and orthopedic surgical services were contacted. In many cases, however, there were conflicts between departments when deciding on further treatment interventions. In one study, the application of a multidisciplinary clinical pathway with joint decision-making between trauma and orthopedic surgeons resulted in improved outcomes in patients with pelvic fractures. 17 Therefore, rapid hemostasis with appropriate treatment following a multidisciplinary algorithm involving hemostatic interventions is crucial. We implemented this pelvic fracture management protocol in 2014 shortly after establishment of the trauma center.
The Advanced Trauma Life Support (ATLS) guidelines recommend using a pelvic binder for external compression of pelvic cavity when there are signs of a pelvic ring fracture from pre-hospital to the ED before imaging. 22 Studies have also demonstrated that commercial pelvic binders are more effective in controlling pelvic bleeding than a conventional “bed-sheet” compression. 23 In Korea, pre-hospital pelvic binder application is very rare and our hospital used the conventional “bed-sheet” compression in a few cases until 2014. After the official approval of commercial pelvic binders by the Ministry of Food and Drug Safety in 2013, we used these in the management algorithm for suspected pelvic fracture patients in 2014. EPF was rarely used in this study because the orthopedic surgeons in our hospital prefer pelvic binder application over EPF. Furthermore, since there is only one orthopedic surgeon in charge of trauma at our institution, emergency EPF is rarely implemented. In a study comparing pelvic binder and EPF in patients with pelvic fractures, those who underwent EPF needed higher amounts of transfusion. 24 Thus, until now, we have mainly utilized pelvic binders for external compression purposes in the algorithm for pelvic injury management in the initial phase.
AE has been used since the 1970s for hemorrhage control in patients with pelvic bone fractures. It has been proven to be effective and remains the most widely used hemostatic intervention. However, AE may not be an effective intervention to stop bleeding due to pelvic fracture because approximately 80% of the bleeding is associated with bone or venous bleeding. 11 Venous bleeding cannot be managed by AE, so AE in hemodynamically unstable pelvic injuries results in poor patient outcomes with mortality rates greater than 40%. 11 In addition, the availability of AE varies by institution. AE requires specific facilities, equipment, and human resources, so some centers are unable to perform this technique. Even at centers that can perform AE, it might not be available immediately, especially at night or during the weekend, which can further increase the mortality rate.14,25 Several studies have reported that the time from ED arrival to AE was at least 2 h, extending up to more than 5 h.26,27 In our study, the time to AE only decreased from 269 min in the pre-phase to 181 min in the post-phase, but this waiting time is still too long for hemodynamically unstable patients.
PPP has been proposed as an alternative intervention to AE. PPP is a simple procedure, so it can be performed in the resuscitation room or operating room by a trauma surgeon within an hour of patient arrival. The time to PPP was 44–55 min in recent studies and this is significantly shorter compared with that for AE.7,28 PPP also significantly decreased the time to intervention in our study. Studies have demonstrated that implementation of clinical guidelines that include PPP for hemodynamically unstable patients led to significant decreases in transfused blood products and mortality.7,28 More recent studies have revealed that PPP is a safe and rapid intervention associated with significantly reduced mortality in hemodynamically unstable patients with pelvic fractures compared with patients managed by a conventional intervention without PPP.29,30 Cheng et al. demonstrated that a three-in-one operation (i.e. EPF, PPP, and on table AE) was associated with lower overall mortality. 31 Moreover, unstable pelvic fractures are often associated with intra-abdominal injuries. One study reported that a total of 34.3% of severe pelvic fracture patients had associated intra-abdominal injuries, including bladder and bowel injuries. 32 In such cases, AE might delay abdominal exploration, or a laparotomy might delay hemostasis using AE. However, a midline laparotomy and PPP can be performed simultaneously with separate incisions, thereby achieving hemorrhage and contamination control rapidly without concerns for cross-contamination in the retroperitoneal space from bowel injuries. 15 Kam et al. illustrated the interventional approach of multiple devices (Figure 4). 33 In this study, concomitant laparotomy increased in the post-phase after the inclusion of PPP in the management algorithm. In addition, laparotomy for the decompression of abdominal pressure in patients with suspected abdominal compartment syndrome was only performed in the post-phase. The World Society of Emergency Surgery (WSES) guidelines for pelvic fracture recommend that PPP should always be considered in hospitals with no AE services and that PPP is an effective surgical measure for early hemorrhage control in hypotensive patients with bleeding pelvic disruptions. 22 Therefore, PPP is recommended as the first intervention for hemodynamically unstable patients (WSES grade IV) in the pelvic trauma management algorithm. 22
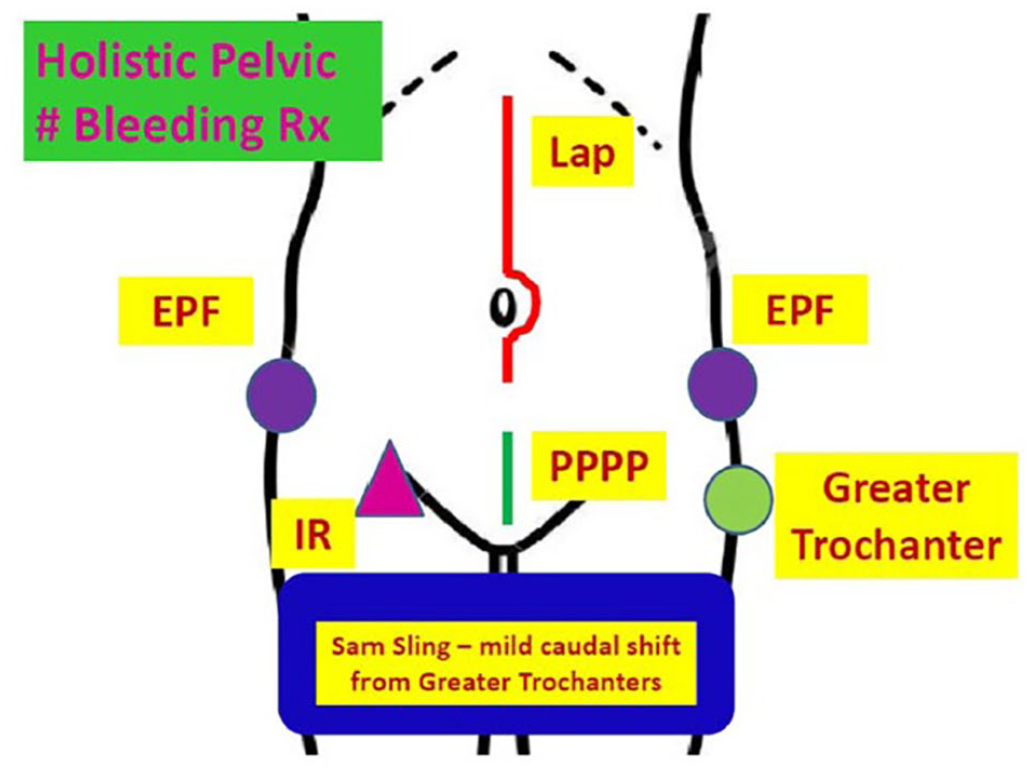
Schematic diagram of abdominopelvic hemostasis interventions.
REBOA has recently been reported as a viable alternative to performing an aortic cross-clamp (ACC) through emergent thoracotomy.34,35 REBOA can be a “bridge” procedure in cases of torso hemorrhage followed by an operation or AE. REBOA can be placed in zone 1 (supra-celiac) or zone 3 (infra-renal). Zone 3 REBOA can be optimal, especially for pelvic bleeding, because it can raise blood pressure and reduce arterial bleeding associated with pelvic injury while preventing ischemic insult to visceral organs, as well as having a long occlusion time. 36 Although there is little evidence of mortality benefit in previous articles, the WSES guidelines suggest REBOA as an alternative to ACC and propose that zone 3 REBOA should be considered to be a bridge to definitive treatment in hemodynamically unstable patients. 22 Our center has implemented REBOA in the pelvic injury management algorithm since 2016 and REBOA was performed in 10 patients; 80% of these were deployed in zone 3, with three patients surviving until discharge.
The purpose of this study was to evaluate changes in outcomes after trauma center establishment and the implementation of a pelvic injury management protocol including PPP and REBOA. This study demonstrated significant reductions in the time to interventions and mortality due to acute hemorrhage. We believe that these changes are due to (1) an attending trauma surgeon being the leader of a multidisciplinary team; (2) reinforcing the competence of surgeons and the trauma team through training such as an REBOA course and vascular skills training; (3) management protocols including pelvic binders, PPP, and REBOA; (4) an increase in concomitant laparotomy; and (5) changes in blood product usage according to the MTP. We think these changes might only be possible to achieve through the establishment of a trauma center with financial support in developing countries such as Korea.
This study has several limitations. The main limitations are its retrospective study design and small sample size due to the study being only from a single institution. These might have introduced selection bias. In addition, we investigated in-hospital mortality only and this might have influenced our results. Finally, we could not evaluate the adherence of individual surgeons to the management algorithm. In the future, a well-designed multi-center prospective study with a larger sample size should be designed to analyze the relationship between trauma center establishment and patient outcomes.
This study builds upon a previous study titled “Effects of the Establishment of a Trauma Center and a New Protocol on Patients With Hemodynamically Unstable Pelvic Fractures at a Single Institution in Korea,” to demonstrate the impact of a trauma system on major pelvic fracture patients.
Conclusion
Improved outcomes in hemodynamically unstable patients with pelvic fracture were achieved because of the establishment of a trauma center and multidisciplinary management protocols as an important bundle of changes. Trauma center designation can advance the management of severe trauma cases such as pelvic fracture, especially in developing countries.
Footnotes
Author contributions
M.L. and B.Y. had full access to all the data and drafted the manuscript. J.L., G.L., Y.P., J.G., M.J., and K.C. participated in the study design, data collection, and the education.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Gachon University research fund of 2019 (GCU-2019-5282).
Availability of data and materials
Data and materials can be made available to the public through direct requests to the corresponding author.
Informed consent
Written informed consent was obtained from each patient included in the study.
Ethical approval
This study was reviewed and approved by Gachon University Ethics Committee (GAIRB2022-010).
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.