
Abstract
Background:
Polypharmacy and inappropriate prescribing are risk factors for adverse drug reactions, which commonly cause complications in older people. The STOPP (Screening Tool of Older Persons’ Prescriptions)/START (Screening Tool to Alert Doctors to Right Treatment) criteria are screening tools, which aim to improve prescribing in the elderly.
Objectives:
The aim was to improve prescribing, using the STOPP/START criteria, for patients aged 65 and above, who were admitted to the Clinical Decisions Unit at University Hospital Lewisham. We focused on the most common prescribing errors in clinical decision unit, an emergency medicine department.
Methods:
We reviewed all patients aged 65 and above admitted to the Clinical Decisions Unit in September. Data was collected from clinical documentation and archived drug charts. This pilot study of 114 patients revealed the most common prescribing errors, of which 8 were STOPP and 11 were START criteria. A plan–do–study–act methodology was implemented over 1 month, involving presentations, emails and posters. Prescribing patterns were then reviewed over 4 weeks in December in 111 patients.
Results:
Focusing on the 8 STOPP and 11 START criteria, there was a significant reduction in the proportion of patients with at least one STOPP error (17.5% to 9%, p = 0.04). However, the decrease in the percentage of patients with at least one START error was insignificant (24.6% to 20.7%, p = 0.24).
Conclusion:
By identifying problematic areas of prescribing and using targeted interventions, the proportion of STOPP errors made in clinical decision unit reduced significantly. This study highlights the prevalence of prescription errors in the clinical decision unit and the impact of using screening tools to reduce incorrect prescribing.
Introduction
Polypharmacy and inappropriate prescribing (including potential prescribing omissions) are risk factors for adverse drug reactions, which commonly cause adverse clinical outcomes in older people.1,2 The elderly (aged 65 and above) are particularly vulnerable to adverse drug reactions due to changes in physiology with age and multiple comorbidities.3,4 Adverse drug reactions account for 30% of all hospital admissions in the elderly. 5 They have been shown to contribute significantly to emergency department attendances, in-hospital morbidity/mortality 6 and new hospital admissions.
These types of errors are prevalent in all healthcare settings. Studies in Ireland have shown that inappropriate prescribing of one or more drugs was prevalent in 21% of patients in the primary care setting, 7 35% in the acute hospital setting, 8 and 60% in nursing home care. 9 These studies have also revealed that serious prescribing omissions were even more prevalent, with 58% of patients in hospitals and 23% of patients in primary care not being prescribed appropriate medication for their comorbidities.
The Beers criteria were developed in 1991 to help tackle inappropriate prescribing in the elderly nursing home population. 10 It was widely used but found to have limitations, as several of the drugs were no longer in use in Europe and others were no longer contraindicated in elderly people. Furthermore, the Beers criteria did not account for prescribing omissions. 11 In 2010, a new criterion for inappropriate prescribing in the elderly was created, which was explicitly designed to be used in the clinical setting and found to be more sensitive than the Beers criteria. 12 It is known as the Screening Tool of Older Persons’ Prescriptions (STOPP) and Screening Tool to Alert to Right Treatment (START) criteria and was revised in 2014. 13
The STOPP/START criteria are composed of a total of 114 criteria, 80 STOPP and 34 START, which were formed, using a Delphi consensus methodology, by a panel of doctors, pharmacists, pharmacologists and primary care physicians with expertise in geriatric medicine and pharmacotherapy in the elderly population from 13 countries in Europe. 11 The 80 STOPP and 34 START criteria are grouped by a physiological system (e.g. the cardiovascular system, central nervous system) and accompanied by a short explanation of the interaction. The STOPP/START criteria have since been successfully applied in a number of settings. A randomised controlled trial showed that using the STOPP/START criteria as an intervention significantly improved medication appropriateness and reduced prescribing omissions in older people hospitalised for acute illness. 14
The aim of this project was to determine the prevalence of inappropriate prescribing in the elderly population in the clinical decision unit (CDU) of a busy London district general hospital and by identifying common prescribing errors, to create an intervention which would be specific to the department and thus would have the most significant effect in improving prescribing in the elderly.
Methods
Initial data collection was carried out to determine the prevalence of inappropriate prescribing in the elderly population (aged 65 and over) admitted to the CDU, an emergency medicine department. Data was collected from clinical documentation using iCare and WinDIP software systems as well as hard copies stored in the archives (September–October 2017). Data collection was performed by medical students and a physician. Written informed consent was not required as patient data has not been used in this article.
Lewisham and Greenwich Trusts and the University Hospital Lewisham approved this audit.
The initial data collection included a total of 114 patients over the age of 65. We reviewed all clinical documentation for these patients to ascertain whether inappropriate prescribing (as outlined by the STOPP/START criteria) was present. Results showed that 37% of these patients had at least one prescribing error. Of these, 8 STOPP and 11 START criteria were consistently not met (i.e. the error occurred more than once; Tables 1 and 2).
The eight STOPP criteria consistently not met in the elderly population of the clinical decision unit.
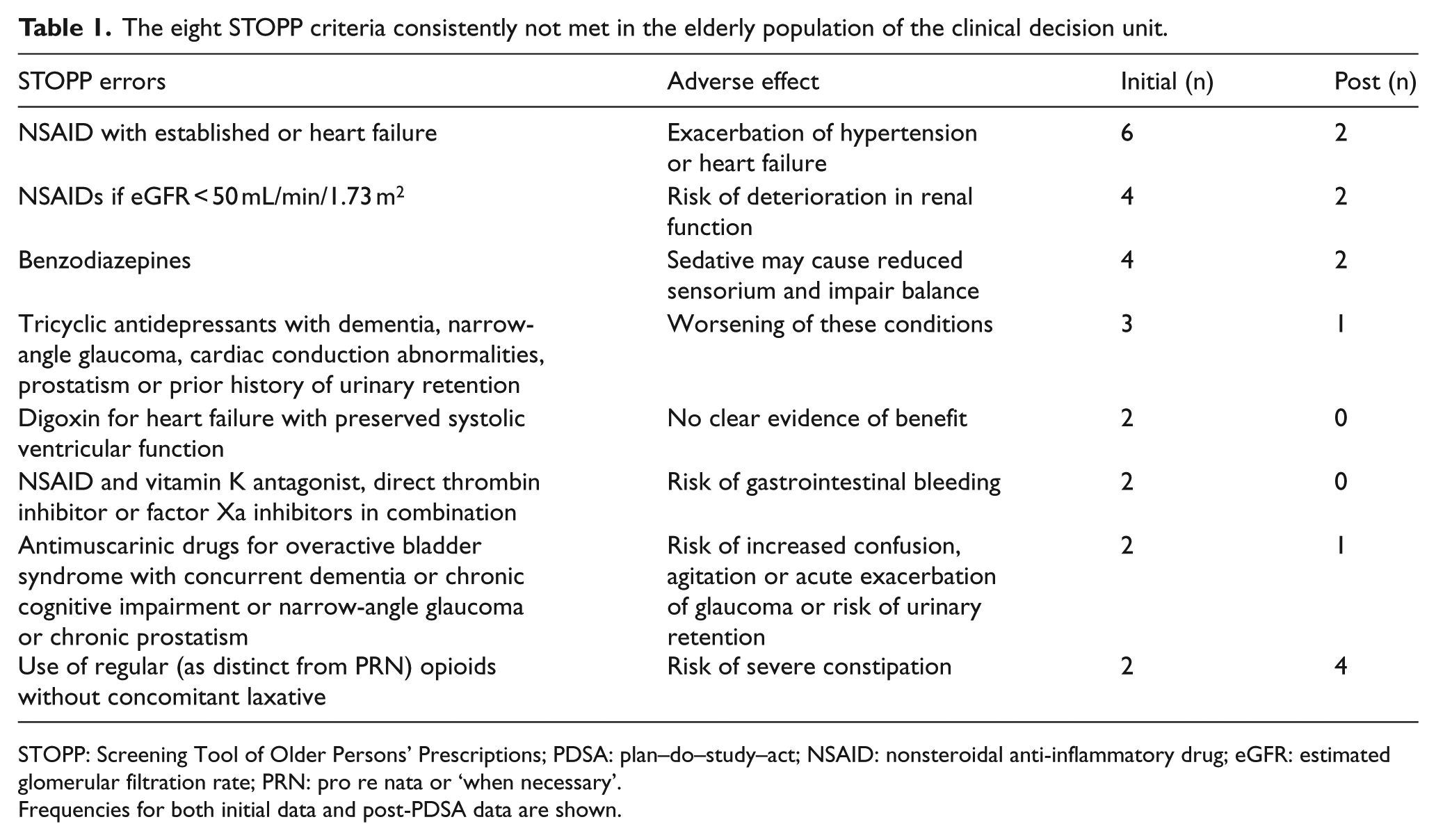
STOPP: Screening Tool of Older Persons’ Prescriptions; PDSA: plan–do–study–act; NSAID: nonsteroidal anti-inflammatory drug; eGFR: estimated glomerular filtration rate; PRN: pro re nata or ‘when necessary’.
Frequencies for both initial data and post-PDSA data are shown.
The 11 START criteria consistently not met in the elderly population of clinical decision unit.
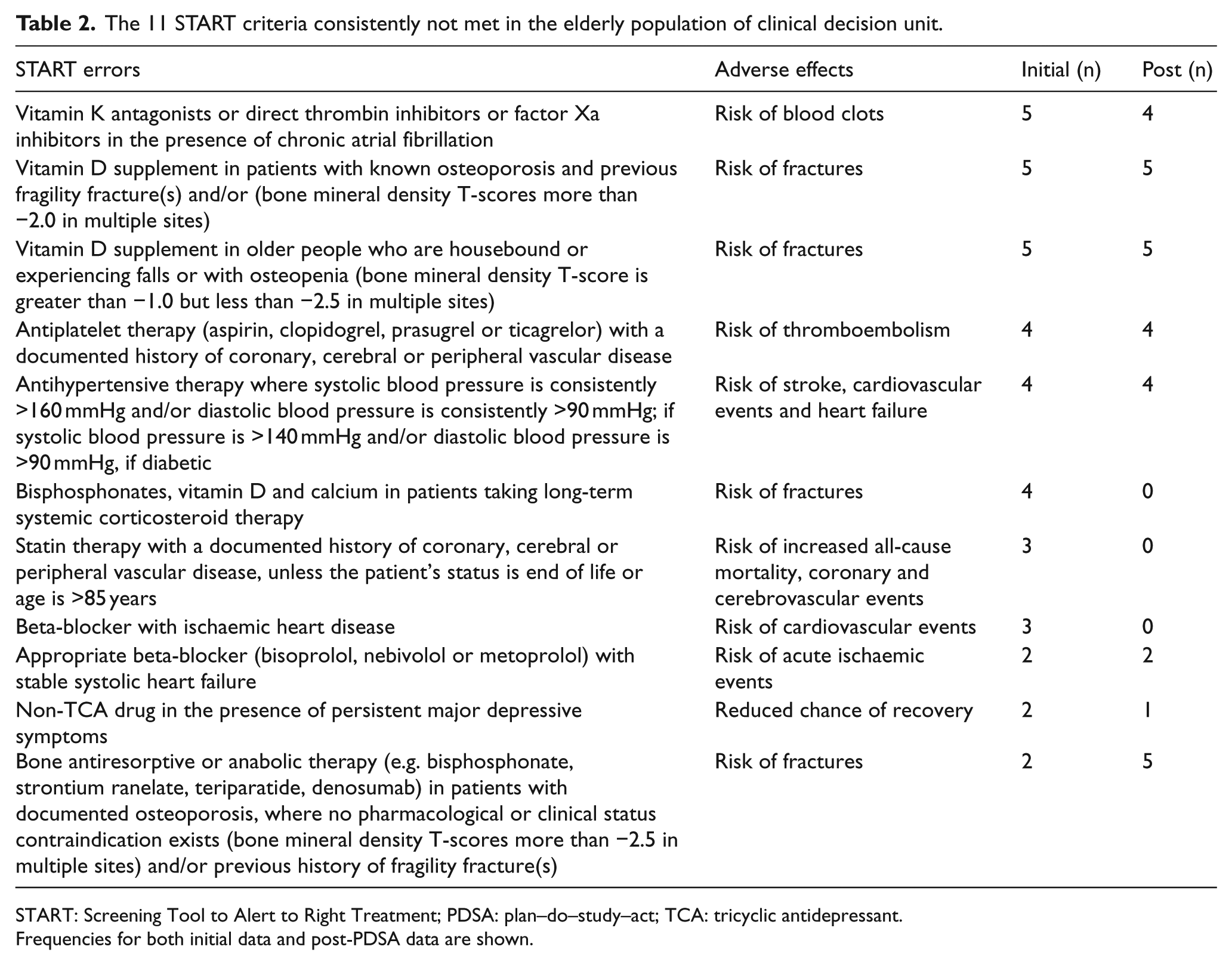
START: Screening Tool to Alert to Right Treatment; PDSA: plan–do–study–act; TCA: tricyclic antidepressant.
Frequencies for both initial data and post-PDSA data are shown.
A plan–do–study–act (PDSA) methodology was implemented over the course of 1 month in November 2017, involving spreading awareness via three presentations, five posters and one email. We then reassessed prescribing patterns in the elderly patients in CDU for 1 month (December 2017–January 2018) focusing solely on the 8 STOPP and 11 START criteria which were consistently not met. SPSS statistical software was used to compare pre- and post-intervention groups with a Z-score greater than p ⩾ 0.05, which was deemed significant.
Results
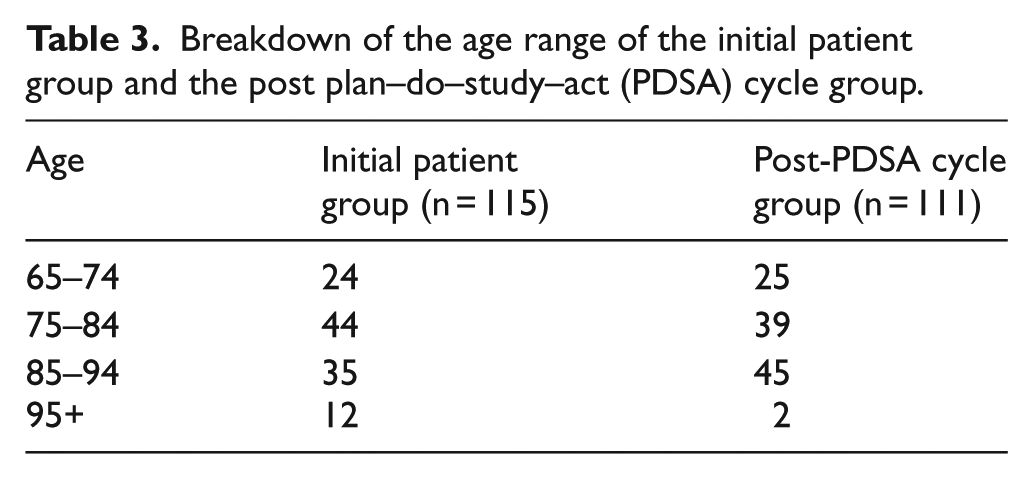
The initial patient group consisted of 115 patients, 67 female and 48 male. The ages in this group ranged from 65 to 101, with the modal age group being 75–84 (Table 3). The post-PDSA cycle group had 61 females and 50 males. The ages in this group ranged from 65 to 98, with the modal age group being 85–94 (Table 3).
Breakdown of the age range of the initial patient group and the post plan–do–study–act (PDSA) cycle group.
Patients in the initial group had a total of 42 patients with errors. The number of STOPP errors in this group was 25, the number of START errors in this group was 39 and therefore the total number of errors in this group was 64. Out of 42 patients, 20 patients had at least one incorrect STOPP error and 28 patients had at least one incorrect START error (Tables 1 and 2).
Patients in the post-PDSA group had a total of 29 patients with errors. The number of STOPP errors in this group was 12, the number of START errors in this group was 29 and therefore the total number of errors in this group was 41. Out of 29 patients, 10 patients had at least one incorrect STOPP error and 23 patients had at least one incorrect START error (Tables 1 and 2). A comparison of errors in the initial study and post-PDSA group can be seen clearly in Figure 1.
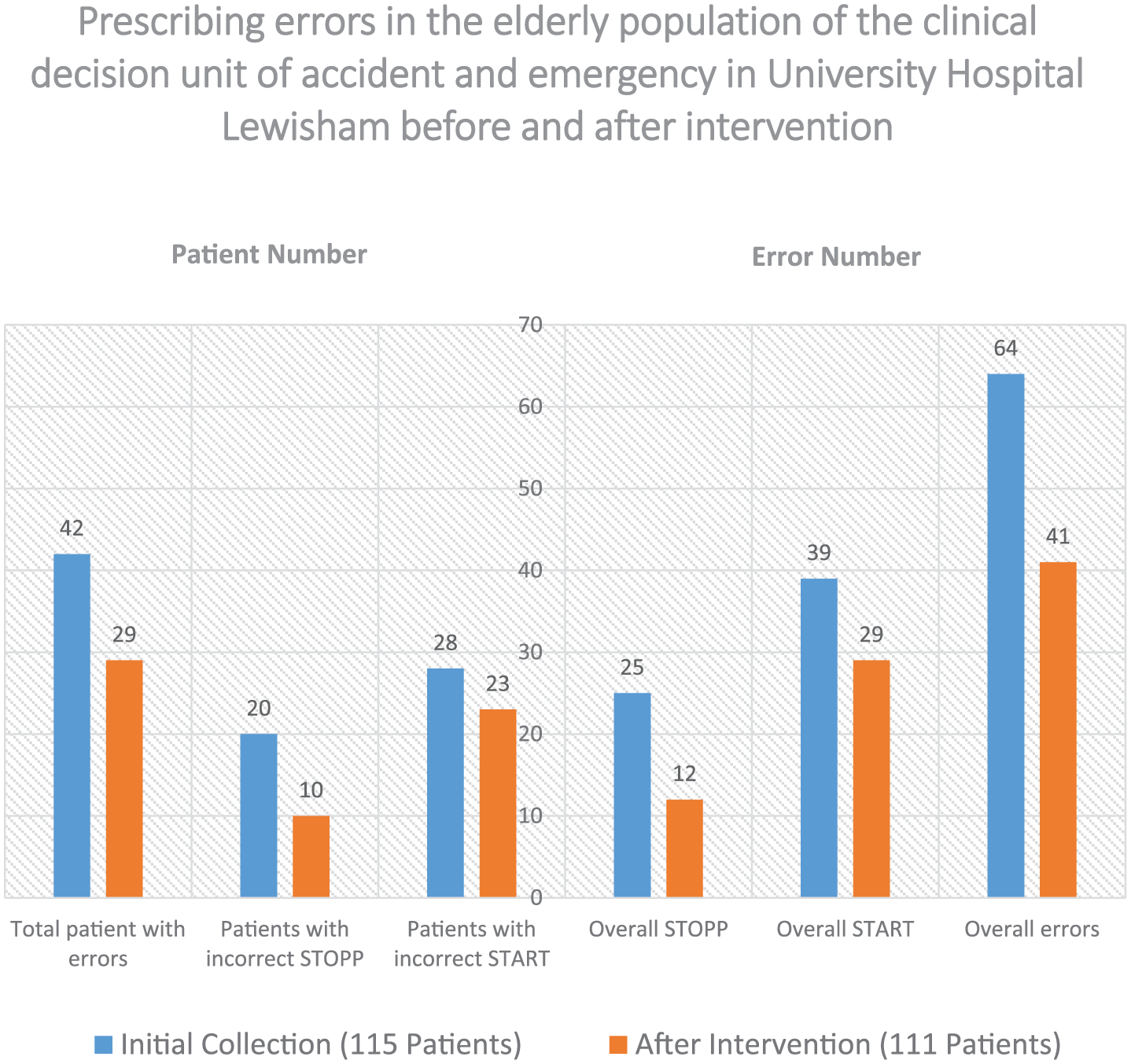
A comparison of prescribing errors pre-intervention and post-intervention in the elderly population (>65) admitted to CDU.
There was a significant reduction in the number of patients with at least one prescribing error (37% to 26%, p = 0.04). The proportion of patients with at least one STOPP error significantly reduced from 17.5% to 9.0% (p = 0.03). The reduction in the proportion of patients with at least one START error was insignificant (24.6% to 20.7%, p = 0.24).
Discussion
This study was conducted in an elderly population within a busy CDU at a London hospital. The total prevalence of prescribing errors was shown to be greater than one in three, which was a significant proportion of patients. To our surprise, it was prescribing errors under the START criteria which were more prevalent, despite the general notion that the elderly population is prescribed too many, rather than too few medications. This trend is also demonstrated in prescribing errors in The Irish Longitudinal Study on Ageing (TILDA), with prescribing omissions being twice as prevalent as inappropriately prescribed medication. 15
The 2015 National Institute of Health and Clinical Excellence (NICE) guidance on Medicines Optimisation recommends using a screening tool, for example, the STOPP/START tool, in older people to identify potential inappropriate prescribing. 16 However, O’Mahony et al. 14 mentioned that the STOPP/START criteria have some limitations in real clinical practice and are best used together with expert medication review by physicians and pharmacists. A systematic review by Hill-Taylor et al. 8 found that there is currently limited evidence related to the clinical and economic impact of the STOPP/START criteria. 17 In contrast, the same team later found that the use of the criteria reduces falls, delirium episodes, hospital length of stay, care visits (primary and emergency) and medication costs, but no evidence of improvements in quality of life or mortality. 18
This intervention significantly reduced the overall number of prescribing errors, as well as the number of patients with at least one STOPP criterion. Appropriate prescribing not only improves the general quality of life of the patient, but can also reduce the burden on the National Health Service (NHS) by reducing costs due to polypharmacy, inappropriate prescribing, adverse drug reactions and hospitalisation. We found that spreading awareness via simple interventions was effective in improving appropriate prescribing even in busy departments such as CDU.
Unfortunately, the impact on prescribing errors from the START criteria did not significantly improve. Thus, tackling START criteria prescribing errors is more challenging and may require a different approach. There are a multitude of factors that may explain the difference in improvement seen between the STOPP and START criteria. One reason may be simply because the STOPP criteria are targeting errors in prescriptions which are more easily recognised. This is because they rely on the automatic subsystem of error recognition. This subsystem relies on implementing schemata in response to specific predetermined conditions leading to a unique response to each schema. 19 This schemata-based automatic response has good retention in long-term memory. 19 START criteria errors are errors of omission and perhaps the single most common human error. 20 This type of error relies on the attentional subsystem of error recognition. This subsystem is harder to sustain over longer periods of time, requires more effort to implement and is a slower cognitive process. 19
Another reason why START criteria may be more difficult to improve when compared to STOPP criteria may be due to the fact prescribing medications inappropriately puts patients at a more immediate risk of adverse reactions and thus may be perceived as more important. 21 Finally, although we strive as clinicians to take a holistic approach when managing patients, this may not be realistic in busy environments with time constraints. Thus, managing comorbidities in an emergency setting may not be a priority. 22
For future interventions, it may be useful to spend extra time on specifically targeting prescribing errors from the START criteria, as improvements in this area would have a significant impact on overall prescribing errors. The EQUIP study of 2009 which investigated the causes of prescribing errors in junior doctors (staff in training) recommend tackling prescribing errors through interprofessional education among other measures. 22 Because there is a high turnover of junior medical staff, dilution of the efficacy of an intervention may occur. 23 Therefore, an education programme which included all junior doctors, other hospital departments, primary care physicians and pharmacists may maximise chances of finding and improving these prescribing errors.
Footnotes
Acknowledgements
A poster on this research has been presented at the International Conference of Emergency Medicine 2018 in Mexico City.
Author contributions
A.K., J.O., S.S., S.S. and H.C. participated in the design of the study, data collection and data analysis. J.O., S.S., B.A. and A.K. wrote the manuscript. H.C. reviewed, edited and approved the manuscript. J.O. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
Data and materials can be supplied by J.O. at
Informed consent
This study did not require informed consent as this was an audit with anonymised patient details.
Ethical approval
Ethical approval was not necessary for this type of study.
Human rights
Human rights approval was not necessary for this type of study.