
Abstract
Background:
Scorpion stings are common in countries dominated by rural and coastal settlements with temperate climate. Scorpion stings are usually harmless and can be seen in local findings, but in some cases, systemic, neurotoxic, and cardiotoxic findings can be seen.
Case report:
A 3 year 7 month old girl was referred to pediatric emergency care 2 h after yellow scorpion (species of Leiurus abdullahbayrami) sting. In our case, cardiac function insufficiently progressed in spite of the standard inotropic and milrinone treatment. On the third day of hospitalization, levosimendan was initiated with good clinical effect.
Conclusion:
In the literature, the use of levosimendan in pediatric patients has been limited to those with low cardiac output syndrome after cardiovascular surgery. The use of levosimendan in children with scorpion sting has been previously reported only in Banille et al.’s study. Scorpion antivenom should be administered intravenously as soon as possible in cases of systemic findings that develop after scorpion stings. This report suggests that levosimendan is temporally associated with improvement in patients who have severe cardiac dysfunction due to scorpion sting and refractory to current treatment.
Introduction
Scorpion stings are common in countries dominated by rural and coastal settlements with temperate climate. Approximately 50 scorpion species on earth are considered to be dangerous to human beings. 1 In southern and southeastern Turkey, the most common scorpion species are Androctonus crassicauda and Leiurus abdullahbayrami. 2 The poison has a rapid distribution to the extravascular compartment, causing early symptoms. Even though many scorpion stings generally cause only mild local effects, nonetheless, systemic, neurotoxic, and cardiotoxic findings can be seen in some cases. The most common cardiovascular and respiratory complications are myocarditis, pulmonary edema, and shock. Various inotropic and inodilator agents are used in patients with cardiac involvement. Levosimendan can be used as an alternative to catecholamines because it increases cardiac output without increasing heart rate and myocardial oxygen consumption. In adults, despite many well-controlled studies indicated the efficacy of levosimendan, reports are limited to cases with low cardiac output syndrome after cardiovascular surgery in children. The use of levosimendan in children with scorpion sting has been previously reported only in Banille et al.’s study. 3
In this case report, we presented a patient with cardiac dysfunction secondary to scorpion stings who did not respond to current standard treatment and a rapid recovery of cardiac function accompanied by the administration of levosimendan.
Case description
A 3 year 7 month old girl was referred to pediatric emergency care 2 h after being stung by a yellow scorpion (species of L. abdullahbayrami) at the medial side of the left knee. On initial examination, the patient was lethargic and had a Glasgow Coma Score of 11 (E3, M5, V3). The patient’s extremities were pale and cold with 4 s capillary refill time. Swelling and hyperemia were noted at the bite site. The patient exhibited involuntary extremity movements, restlessness, sweating, and hypersalivation. The findings of clinical examinations were as follows: arterial pressure was 60/30 mm Hg, heart rate was 127 beats/min, respiratory rate was 40 breaths/min, body temperature was 36.4°C, and oxygen saturation (room air) was 98%. Electrocardiogram (ECG) showed sinus tachycardia. Bilateral infiltrates suggestive of pulmonary edema without cardiomegaly were noted in the bedside chest radiograph. The patient was first reviewed at an interim medical facility where she was provided with one vial of antivenom that was incorrectly administered. One vial had been divided with one-half (2.5 mL) injected into the sting site, and the other half provided intramuscularly. Laboratory investigations showed white blood cell 38.3 × 109/L, hemoglobin 14 g/dL, platelets 533 × 109/L, glucose 14.6 mmol/L, ALT 23 UI/L, AST 46 UI/L, blood urea 549 µmol/L, and blood creatinine 59.5 µmol/L. Arterial blood gases showed pH 7.31, PaCO2 33 mm Hg, HCO3 17.2 mEq/L, and BE −9.2. Serum creatine kinase (CK)-MB was 31.8 nmol/L (n = 3.08–15.7), troponin-I was 0.83 nmol/L (n = 0.03–0.13), and lactate level was 2.0 mmol/L. A vial of scorpion antivenom (5 mL) was administered intravenously—correct way of administration—to the patient in the emergency service admission because of systemic manifestations and inappropriate antivenom administration at the outer center. In Turkey, scorpion antivenom is produced by the Refik Saydam Hygiene Center Presidency and is directed at treatment of A. crassicauda venom. Doxazosin (0.05 mg/kg/dose) was given enterally upon admission and an hour after admission, then the patient was transferred to our pediatric intensive care unit at the second hour of admission to the hospital. Capillary refill time was 3 s and because of coldness of the extremities, doxazosin treatment was continued. Two-dimensional color-flow Doppler echocardiogram revealed mild tricuspid insufficiency, 2–3° mitral valve insufficiency, ejection fraction (EF) was 52%, and left ventricular fractional shortening was 26%. Dobutamine (10 µg/kg/min) and dopamine (10 µg/kg/min) infusions were initiated. An increase in CK-MB and troponin-I levels was detected within the first 24 h. At 24 h after hospitalization, diffuse pulmonary edema (Figure 1), EF 36% (Supplementary File 1), increase in respiratory rate, deterioration of consciousness, hypotension, and decrease in saturation occurred and the patient was intubated. Accompanied by a second dose of scorpion antivenom (5 mL), epinephrine (0.05 µg/kg/min) and milrinone (0.3 µg/kg/min) were added to inotropic treatment because of refractory hypotension and 3 s capillary refill time. On the third day of hospitalization, despite the provided treatment, hypotension, tachycardia, poor peripheral circulation, and decrease in EF (33%) occurred. While dopamine and dobutamine were maintained at the same doses, milrinone treatment was terminated and levosimendan was initiated (6 µg/kg loading and 0.05 µg/kg/s maintenance dose), and continued for 48 h. After initiation of levosimendan, heart rate decreased from 190 to 165, mean arterial pressure increased, and EF escalated from 33% to 59% within 48 h. The clinical chart of the patient recovered from day to day, dopamine and dobutamine were terminated, and the patient was extubated on the sixth day of hospitalization. On the 12th day of hospitalization, the findings of clinical examinations were as follows: arterial pressure was 99/62 mm Hg, heart rate was 82 beats/min, and respiratory rate was 24 breaths/min. The patient was discharged with normal Doppler echocardiogram findings (EF was measured 72%), and troponin-I levels were within the normal range. Troponin levels, daily EF measurements, and vasoactive inotropic scores (VIS) are shown in Table 1.
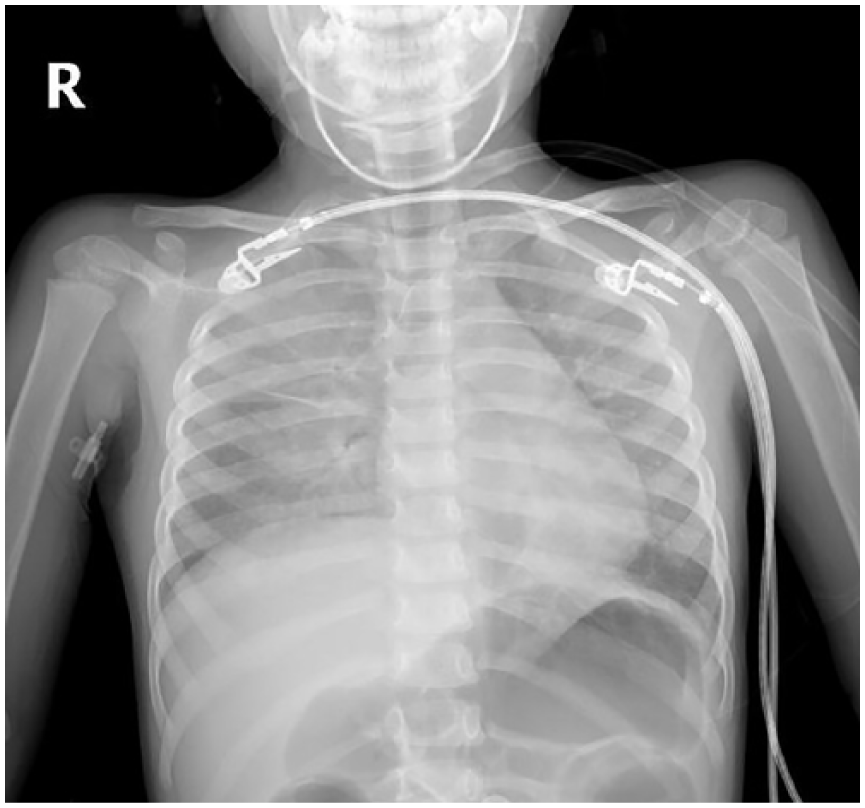
Diffuse pulmonary edema in chest radiograph.
Troponin levels, daily EF measurements, and VIS.
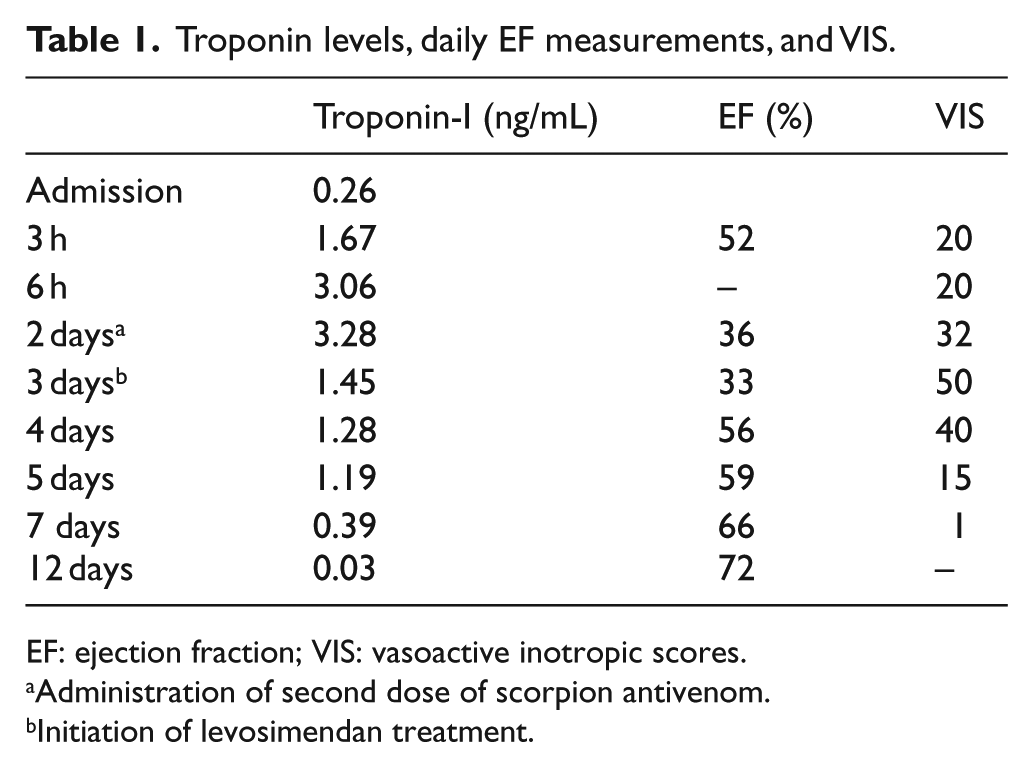
EF: ejection fraction; VIS: vasoactive inotropic scores.
Administration of second dose of scorpion antivenom.
Initiation of levosimendan treatment.
Discussion
In some global areas, scorpion stings constitute a common form of envenoming especially among children who live in rural areas. Children stung by several medically important species may develop serious envenoming that can have a fatal outcome. In Turkey, 8 types are venomous among total of 23 types of scorpions, and the most common scorpion species are A. crassicauda and L. abdullahbayrami in southern and southeastern Turkey. 2 The severity of poisoning due to scorpion stings and the clinical course of the patients may vary. Sweating, agitation, priapism, tremor, vomiting, and diarrhea are the most common systemic findings. While changes in the level of consciousness, limitation of vision, miosis, mydriasis, anisocoria, convulsions, and coma are indications of neurotoxicity, brain edema and brain ischemia are rarely detected by further examination. The most common cardiological complications are myocarditis, pulmonary edema, and shock. The scorpion sting reasoned deaths are generally caused by respiratory and circulatory failures, and the mortality rate ranges from 8.9% to 12.5%.4,5 In these studies, mortality rates are determined to be higher in younger age groups. Gökay et al. 6 reported a retrospective evaluation of 189 scorpion sting cases between 2007 and 2013, which 53% of the patients had antivenom therapy and overall mortality rate was 0%.
While there are no specific diagnostic tests for scorpion stings, investigations should be made for complications that may be a result of scorpion venom. In ECG assessments, sinus tachycardia is the most common finding; however, segment (ST) elevation and depression, T wave changes, and sinus bradycardia are also reported rarely. 4 Left ventricular systolic failure with left ventricular dilatation is the most frequently detected finding by echocardiography. Cardiac troponin-I is the most important diagnostic and prognostic laboratory indicator of myocarditis and acute coronary syndrome. A study on non-envenomed subjects revealed that a normal troponin-I can be generally interpreted as the myocardium being not affected. 7 Patients with cardiac involvement should be monitored closely in intensive care conditions and supportive care should be applied. Recurrent physical examination, thoracic ultrasonography, and echocardiography should be performed to evaluate cardiac functions and pulmonary edema. Bahloul et al. 4 reported a retrospective evaluation of 685 scorpion sting cases in Tunisia between 1990 and 2002, which determined that the most common problem was cardiac failure (79%) in those patients, whereas 75% of patients faced inotropic cardiogenic shock or pulmonary edema. Cardiotoxicity occurs due to continuous beta-receptor stimulation leading to cardiac fatigue and consequently causes a decrease in left ventricular function. Previous studies reported that delayed admission to the hospital and hypotension at the time of admission were associated with more severe clinical signs and myocardial dysfunction.8,9
Although some investigators do not recommend antivenom for envenoming by medically important buthid scorpions, studies have shown the efficiency of antivenom in Turkey.6,9,10 The study in the murine model suggest that an equine antivenom against A. crassicauda may be effective at least against L. quinquestriatus, a closely related congener of L. abdullahbayrami. 11 Scorpion antivenom should be administered as soon as possible in patients with systemic findings. Scorpion antivenom sometimes appears to be applied to the intramuscular or sting site as a misapplication, but in this case, an inadequate response to the scorpion venom can be emerged. In case of delayed administration, antivenom will not be effective because the venom reaches the target organ. Studies have shown that the frequency of pulmonary edema, coma, catecholamine need, and mortality are significantly higher in patients who referred delayed to the hospital following scorpion envenomation.4,12 Antivenom was administered intravenously to the patient who had systemic findings at the emergency department because of non-evidence-based incorrect administration of antivenom given at the initial treating facility.
Treatment of serious scorpion envenoming includes antivenom, prazosin, inotropic agents, atropine, nitroglycerin, and benzodiazepines. Due to the less sale of prazosin in Turkey, doxazosin treatment began to our patient for hyperadrenergic situation. In some cases, standard inotropic agents may not be sufficient to improve cardiac function, and other agents may need to be added.
The main mechanism of levosimendan is an increase in the troponin C affinity for Ca2+ and a stabilization of the troponin C conformation. Levosimendan protects the heart against ischaemia–reperfusion damage by the opening of cardiac mitochondrial ATP-sensitive potassium channels. 13 If the effect of scorpion antivenom on myocardium is taken into account, we may think levosimendan can be effective diminishing the effects of scorpion venom.
Levosimendan can be used as an alternative to catecholamines because it increases cardiac flow without increasing heart rate and myocardial oxygen consumption. Although further studies about the use of levosimendan are needed, recent studies have suggested that levosimendan can be preferred in cases with myocardial damage, decreased cardiac output, tachycardia, and inadequate systolic function.14–16 In a study, levosimendan and milrinone efficiency were compared in 50 pediatric patients, which are as follows: applied cardiopulmonary bypass, reported better cardiac output in the levosimendan group, better hemodynamic profile, and fewer complications. 16 The use of levosimendan in scorpion stings has not been reported before. In our case, cardiac function insufficiently progressed in spite of the standard inotropic and milrinone treatment. Our patient did not respond to the current treatment; levosimendan was initiated with good clinical effect. In the literature, the use of levosimendan in pediatric patients has been limited to those with low cardiac output syndrome after cardiovascular surgery. However, Banille et al. 3 reported a study of 25 patients—5 patients post scorpion poisoning—with diagnosis of severe low cardiac output; all patients showed heart rate decrease, mean blood pressure increase, and ScvO2 increase after levosimendan administration.
We presented a patient with cardiac dysfunction secondary to scorpion stings who did not respond to current standard treatment and a rapid recovery of cardiac function accompanied by the administration of levosimendan. Even if the clinical improvement could be related to the nature of the disease, recent studies evaluated the efficacy of levosimendan in patients with inadequate systolic function, and clinical improvement of our case after levosimendan and our clinical experience on scorpion sting make us think that levosimendan could be effective in scorpion sting treatment.
In conclusion, scorpion antivenom should be administered intravenously as soon as possible in cases of systemic findings that develop after scorpion stings. Although further studies about the use of levosimendan are needed, this report suggests that levosimendan is temporally associated with improvement in patients who have severe cardiac dysfunction due to scorpion sting and refractory to current treatment.
Supplemental Material
HKJ827195_online_supplement – Supplemental material for Levosimendan treatment in a child with treatment-resistant left ventricular systolic dysfunction after scorpion sting
Supplemental material, HKJ827195_online_supplement for Levosimendan treatment in a child with treatment-resistant left ventricular systolic dysfunction after scorpion sting by Ahmet Yöntem, Rıza Dinçer Yıldızdaş, Özden Özgür Horoz, Nagehan Aslan, Merve Mısırlıoğlu, Hayri Levent Yılmaz and Sevcan Erdem in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
We wish to thank Celal Varan, pediatric cardiologist, for two-dimensional color-flow Doppler echocardiogram measurements. Thanks to the patient’s parent for allowing us to share the details.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data and materials can be accessed from hospital data processing system.
Ethical approval
Levosimendan has been used as an agent in pediatric patients with myocardial damage in many studies, which are mentioned in the text. For this reason, the approval of the ethics committee has not been obtained.
Human rights
We are committed to human rights.
Informed consent
Written informed consent was obtained from the patient’s father for their anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.