
Abstract
Background:
South Korea has one of the highest rates of suicide in the world, which poses an immense socioeconomic burden on the healthcare system.
Objectives:
We hypothesized that the implementation of a Crisis Intervention Team would lead to an improvement in completion rates of suicide prevention counseling programs.
Methods:
This is a retrospective before-and-after analysis, and was carried out in the emergency department in the city of Ansan, South Korea. The Crisis Intervention Team, funded by the Ministry of Health and Welfare, counsels suicide attempt patients with the ultimate goal of assuring proper administration of mental healthcare from community suicide support programs. Data on suicide attempt patients were collected using medical records. The primary outcome was defined as completion of the 8-week follow-up period for suicide attempt patients with the community suicide support programs.
Results:
A total of 246 patients from the pre-intervention period and 296 patients from the post-intervention period were included in the study. The completion rates of the 8-week follow-up period increased significantly after the intervention. During the pre-intervention period, 9 patients (3.7%) who were referred to the community suicide support program completed the 8 weeks of follow-up, whereas in the post-intervention period, 56 patients (18.9%) followed up for 8 weeks or more (p < 0.0001). The secondary outcome, overall linkage rates to community suicide support program, did not change significantly, with a minor increase from 46 (18.7%) to 63 (21.3%) (p = 0.45).
Conclusion:
The implementation of an in-hospital Crisis Intervention Team dedicated to active and assertive counseling that begins in the emergency department was correlated with significantly increased completion rates of the 8-week follow-up counseling program.
Introduction
South Korea has the highest rate of suicide in the world among Organisation for Economic Cooperation and Development nations. 1 As the most common cause of death among those in the second and third decade of life, the rate of suicide has increased fourfold over the past 20 years, and poses an immense socioeconomic burden on the healthcare system. 2
While it is preferable to be able to identify patients at a high risk for self-inflicted harm before it occurs, this is not always feasible. Risk assessment for suicide has been extensively studied, yet is still an inexact process. 3 Studies cite healthcare provider factors such as attitudes toward suicide, limited training, the emergency department (ED) environment, and policies as barriers to effectively assessing suicide risk in the ED. 4 Numerous studies have shown that a history of prior attempts at suicide is the strongest predictor of future attempts, and that preventive efforts are needed to target the period immediately after discharge from the ED. 5 Any attempt at self-harm presenting to the ED therefore is a valuable opportunity for an intervention to prevent future deterioration of mental health culminating in a repeated suicide attempt.
In Korea, the Ministry of Health, in conjunction with multiple regional base hospitals, established the Crisis Intervention Team (CIT) project for suicide attempt patients. We hypothesized that the implementation of the CIT would lead to an improvement in completion rates of the standard 8-week suicide prevention counseling program.
Methods
Setting and study design
This is a retrospective before-and-after analysis, and was carried out in the ED of a tertiary academic teaching hospital in the city of Ansan, South Korea. As the only academic hospital in Ansan, serving a population of 700,000, there are approximately 50,000 total ED patient visits per year.
The intervention consisted of the implementation of the CIT. Prior to the creation of the CIT, suicide attempt patients were referred to community suicide support programs (CSSP) directly from the ED for counseling after discharge. One of the senior daytime nurses was a designated point of contact with the CSPP, and for suicide attempt patients who would visit the ED during day shifts, this nurse would fax patient information and consent forms for follow-up to the CSPP. For suicide attempt patients who visited the ER outside of regular hours, the nurse would compile a list of the patients from the previous night or weekend, and fax it in with the relevant forms the following business day.
The CIT intervention consisted of two full-time government-funded social workers, who begin counseling in the ED and continue to do so for up to 4 weeks after discharge, with the ultimate goal of assuring linkage of patients to proper administration of mental health counseling from CSSP. The CIT operates during regular business hours. For patients who visit the ED outside of regular hours, the CIT would review all of the previous day’s electronic medical records for self-harm and suicide attempts, and contact the patients and/or guardians to begin counseling, by telephone initially, and if deemed necessary, by visit. Patients who were admitted received the same intervention by the CIT as patients discharged from the ED. The CIT was dispatched to their ward and in-hospital counseling, with post-discharge follow-up, was conducted in the same manner as ED patients.
All patients during both the pre- and post-intervention periods were evaluated by the psychiatry department during their stay in the ED as a matter of hospital protocol for suicide attempts. Consent for CIT follow-up was obtained independent of whether patients agreed to continue care with the psychiatry department.
The CIT initially tracks and counsels patients with weekly telephone calls for 4 weeks upon discharge. After, or during, this initial period of “pre-counseling,” patients who consent are linked with a community mental health center. The CIT obtains progress reports from the mental health center case officer at 2, 4, and 8 weeks to ensure that proper follow-up care is being administered, such as therapy counseling sessions, provision of information for government financial support for medical bills, referrals to psychiatrists as necessary, and monitoring for repeat suicide attempts. The 8-week time frame for follow-up was based on literature review and the consensus of an expert opinion panel discussion.
Study population
Eligible patients were those who had visited Korea University Medical Center Ansan hospital for attempted suicide during the study period. We included all patients who stated that the intent of their actions was “to die.” Cases that were discharged from the ED, or admitted to psychiatry or other departments, were included. We excluded patients who were either dead on arrival to the ED, or whose outcome resulted in death, legal minors under the age of 19, and patients with foreign nationality, due to their ineligibility for government-subsidized health care support after discharge.
The intervention group was defined as suicide attempt patients visiting the ED from January to December 2015, and the control group as suicide attempt patients visiting the ED from August 2013 to July 2014. The implementation of the CIT took place in August 2014, and therefore a lead-time of approximately 5 months was given to allow for a period of integration.
Data collection
Data on suicide attempt patients were collected using ED electronic medical records. Demographic variables such as age, gender, and type of insurance were collected, along with prior history of psychiatric illness and/or suicide attempt, method of ED visit, initial mental status, mechanism of injury, and final disposition result from the ED. Information on duration of follow-up at the health care centers, and completion rates of the 8 weeks of suicide prevention counseling was obtained from the databases of CSSP. The study was approved by the internal ethics review board of Korea University Medical Center Ansan Hospital (IRB No. 2017AS0044).
Outcome measures
The primary outcome was defined as completion of the 8-week follow-up period for suicide attempt patients with the community mental health centers. The 8-week period was defined as beginning upon CSSP linkage. The secondary outcome was defined as the overall linkage rate of patients discharged from the ED to community support programs. Linkage was defined as the transfer of patient case information to the CSSP.
Data analysis
Descriptive statistics between the before and after periods for categorical variables are presented as frequency distributions and percentages. Continuous variables are reported as median and interquartile ranges (IQR). Univariate comparisons in the distribution of demographic and clinical factors were analyzed using chi-square for discrete variables and Wilcoxon rank-sum test or Kruskal–Wallis test for continuous variables. For variables with high proportions of missing data, and subjects with complete data that differed to those with missing data, a multiple imputation technique was used, in which we included age, gender, types of medical insurance, types of suicide methods, and ED result. 6 This approach was used for the following variables: previous suicide attempt (missing n = 87) and history of psychiatric illness (missing n = 191). A multivariable logistic regression analysis was used to compare outcomes between the two groups, adjusting for potential risk factors such as sex, age, insurance level, pre-suicide psychiatric medical history, and previous suicide attempt history.
Results
Characteristics of study subjects
Of the total 47,911 patients visiting the ED during the pre-intervention period, 294 (0.7%) patients (control group) attempted suicide, and among the 49,534 patients from the post-intervention period, 335 (0.7%) patients (intervention group) attempted suicide. After excluding patients under 19 years of age (before period n = 22, after period n = 16), dead-on-arrival patients and patients who ultimately expired (before period n = 9, after period n = 14) and non-Korean nationals (before period n = 17, after period n = 9), a total of 246 patients from the pre-intervention period and 296 patients from the post-intervention period were included in the study (Figure 1). The most common suicide attempt method was poisoning in both groups (pre-intervention n = 154, 62.6%; post-intervention n = 176, 59.5%). There were no significant differences between the two groups in terms of gender, age, insurance status, mechanism of attempt, previous psychiatric illness, or prior suicide attempt history (Table 1).
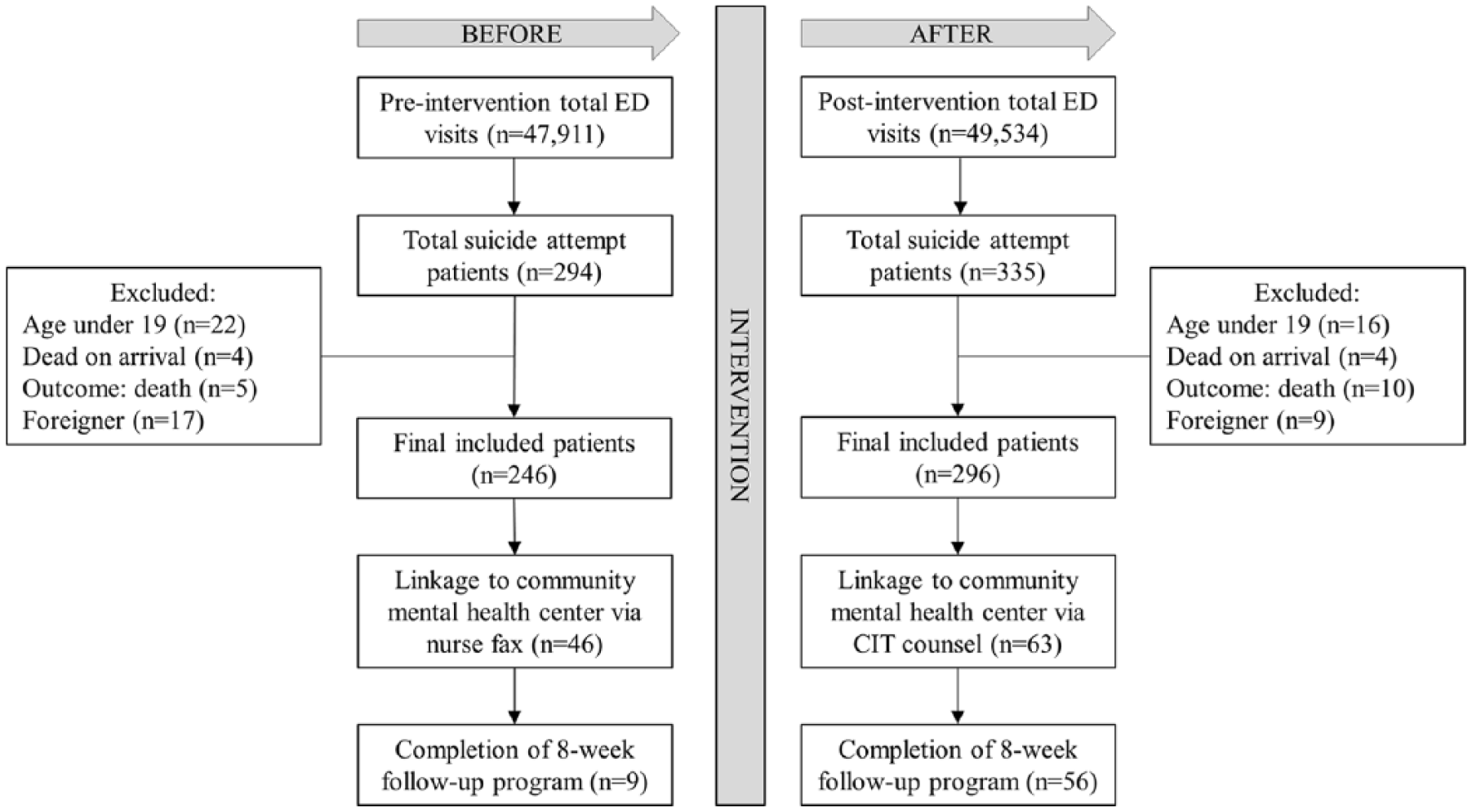
Flow diagram of participant inclusion and exclusion.
Baseline characteristics for patients in pre- and post-intervention periods.
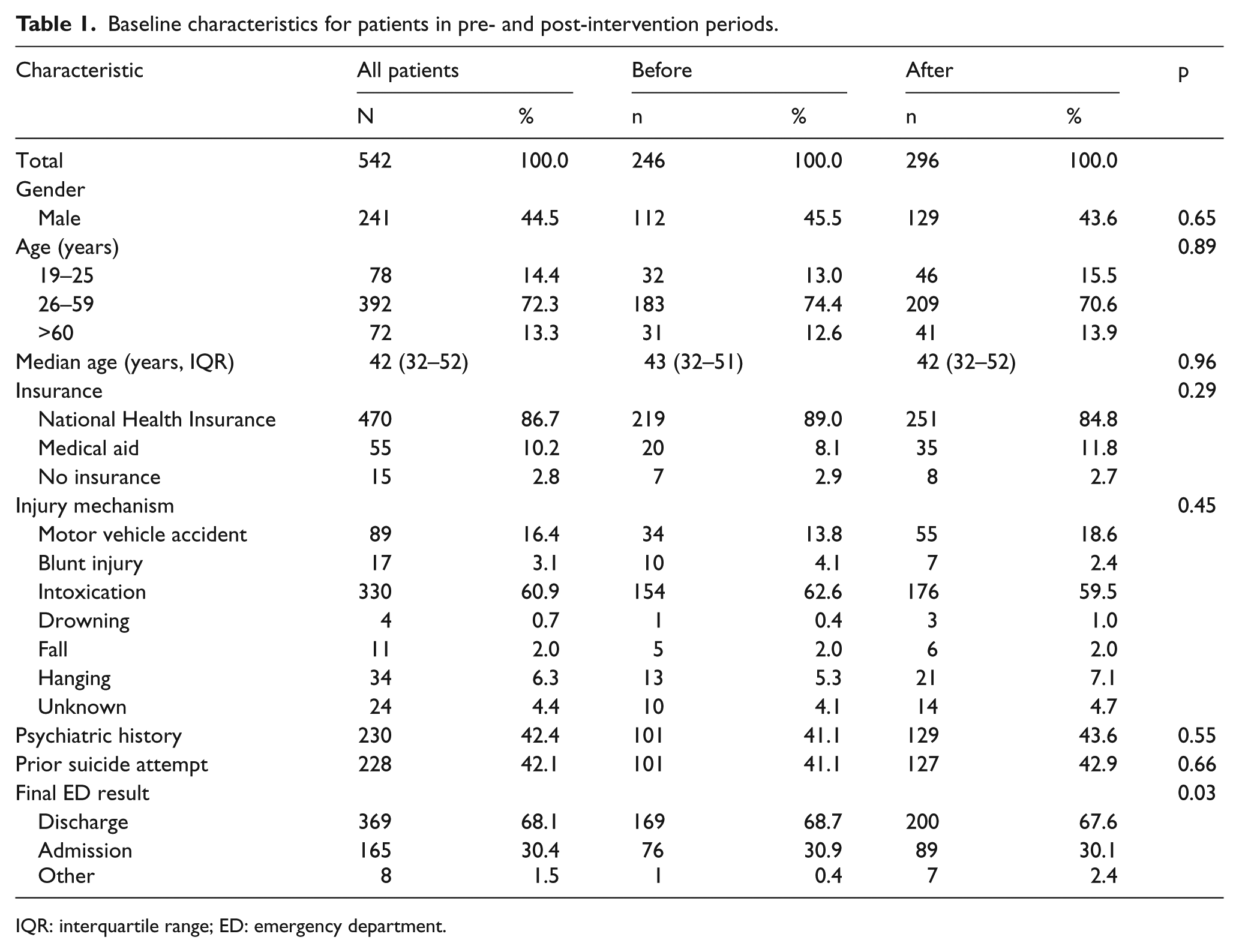
IQR: interquartile range; ED: emergency department.
Main results
The completion rates of the 8-week follow-up period increased significantly after the intervention (Table 2). During the pre-intervention period, 9 patients (3.7%) who were referred to the CSSP completed the 8 weeks of follow-up, whereas in the post-intervention period, 56 patients (18.9%) were followed up for 8 weeks or more (p < 0.0001). The secondary outcome, overall linkage rates to CSSP, did not change significantly, with a minor increase from 46 (18.7%) to 63 (21.3%) (p = 0.45).
Pre- and post-intervention outcomes.
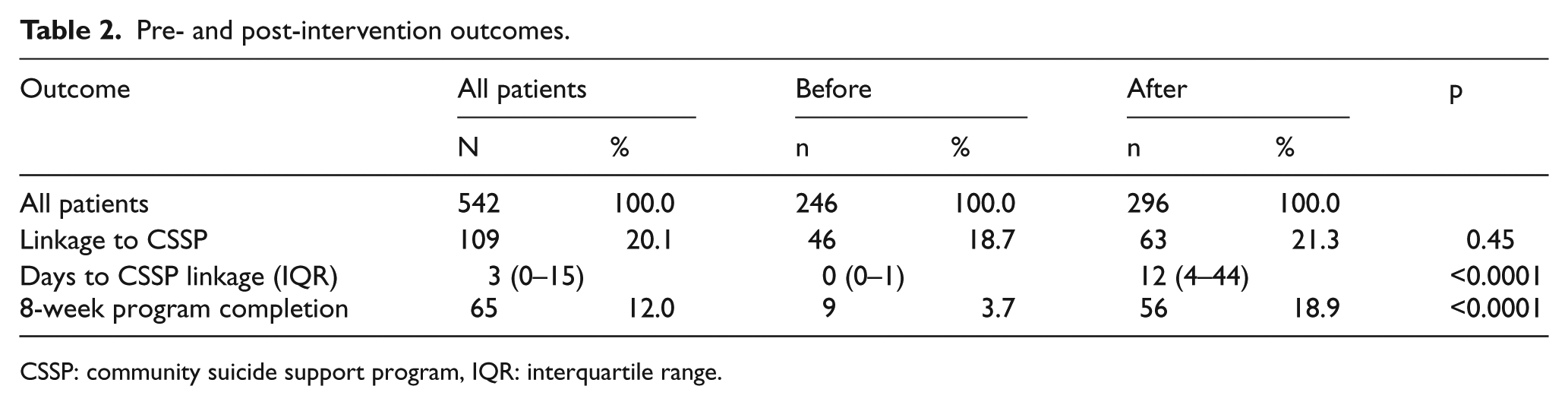
CSSP: community suicide support program, IQR: interquartile range.
After adjusting for possible suicide risk factors such as gender, age, insurance status, previous psychiatric illness, and prior suicide attempt history, CIT intervention showed a higher odds ratio of completion of the 8-week follow-up program (adjusted odds ratio (aOR) 6.39, 95% confidence interval (CI) of 3.06–13.37). Patients with a history of pre-existing psychiatric illness and patients with a prior suicide attempt were both more likely to complete the 8 weeks of follow-up with an aOR of 2.21 (95% CI 1.21–4.05) and 2.65 (95% CI 1.21–3.93), respectively. CIT did not have a significant effect on overall community support program linkage rates (aOR 1.14, 95% CI 0.74–1.76). Time to CSSP linkage was set at 0 in the control group, as patient case information was faxed either on the same or next business day that the patient visited the ED. In the post-intervention group, the CIT counseling period accounted for the 12-day mean leading to CSSP linkage.
Discussion
The period immediately after discharge from hospitalization is when patients are at a heightened risk for repeat suicide attempts.7–9 The majority of post-hospitalization suicides occur during the first month after discharge, and some studies have shown the rate of suicide during this period to be more than 100 times that in the general population.10–12 The ED in particular discharges a significant number of suicide attempt patients, and according to multiple studies, the risk for repeat attempt for these patients is as high as 25%.13–15
To address this issue, numerous studies have examined the effectiveness of follow-up contact interventions such as telephone contact and postcards, and the evidence base for such contact intervention is promising.16–20 However, to the best of the authors’ knowledge, there has not yet been any documented investigation into the effectiveness of an intervention team dedicated to active post-discharge follow-up and committed to ensuring proper care with mental health professionals.
Our study showed that after CIT implementation, the odds of completing the 8-week follow-up period increase by a factor of more than 6. This can likely to be explained by the fact that the CIT is mandated to pre-counsel patients for a period of 4 weeks with weekly telephone calls before linking them with a community mental health center. This contrasts sharply with the pre-intervention period, during which patient consent forms for follow-up would be faxed to the community mental health centers, and a case officer from a CSSP who had never met the patient before would contact patients by telephone. The median days to CSSP linkage in the pre-intervention period was 0 (because forms were faxed in to CSSP immediately), whereas during the post-intervention period, the median was 12 (Table 2). The authors hypothesize that the pre-counseling, which begins in the ED, prepared patients for long-term follow-up by instilling in them the need to seek help and rendering patients more receptive to mental health care.
This pre-counseling effect can likely be attributed to the fact that the CIT is tasked with meeting the patients face-to-face upon their initial visit to the ED. When suicide attempt patients visit the ED outside of regular hours, contact is made via telephone the very next day. Previous studies have shown that early intervention, especially after an ED visit for a self-harm attempt, can be effective in preventing future suicide attempts,21–23 and this early-access intervention by the CIT likely plays a key role in building the rapport necessary to prepare patients to be more receptive to longer-term counseling with either psychiatrists or CSSP.
Even after patients are linked with community mental health centers, the CIT conducts a form of quality assurance by following up with the case worker at the health center at 2, 4, and 8 weeks post-linkage. The CIT team members inquire as to how the case is being handled, what kind of care the patient is receiving, and whether the patient is responsive to counseling. According to CIT anecdotal reports, there are a significant number of cases where the check-in phone call results in the case worker immediately contacting the patient to check on their progress, thereby preventing potential loss of follow-up. This quality assurance mechanism that ensures continuity of care during the most acute phase of suicidal ideation likely has protective effects for patients who were recently discharged from the ED for a suicide attempt.
Furthermore, the weekly pre-counseling telephone calls by the CIT serve as a form of surveillance. Risk for re-attempt is ascertained by the trained social workers of the CIT, and patients who are deemed high risk (e.g. express detailed plans for an imminent attempt) are encouraged to visit the ED, the CSSP, or the psychiatry outpatient clinic for emergent counseling. The surveillance effect, combined with pre-emptive counseling, likely has the effect of not only building stronger rapport with patients by letting them know they are being cared for, but furthermore may contribute to a potential decrease in overall rates of attempted suicide within the community.
Counseling program completion rates overall remained low, even in the intervention group, at less than 20%. This is likely attributable to the low rate of patient consent for follow-up. Often, patients who are seen in the ED for suicide attempts are acutely emotionally unstable and therefore refuse further care, whether by psychiatry or counseling, despite efforts on behalf of ED and psychiatry staff members. Low health literacy rates, 24 the perception of the suicidal behavior being a social or financial problem rather than a mental health issue, and the social stigma of being labeled a psychiatric patient may all contribute to the refusal to receive proper care. It is an ongoing challenge to explain the benefits of care, the pitfalls of deteriorating mental health, and ultimately obtain proper consent in a hectic ED environment.
The data would seem to suggest that the intervention had no effect on CSSP linkage rates. The authors believe that it is more likely, however, that while the overall quantity of linkages did not increase, the “quality” of the linkages was in fact improved by the pre-counseling effect. The 21.3% of patients who were ultimately referred to CSSP were consenting, prepared, and willing to undergo counseling sessions. On the contrary, the 18.7% pre-intervention referral group were patients whose information and consent forms were merely faxed over to CSSP. These patients were eventually “cold-called” by a CSSP counselor, with varying degrees of success at persuading patients to come in for counseling programs.
Another finding of interest was that patients with either a history of suicide attempt or psychiatric illness were found to be more likely to complete the 8-week follow-up program with CSSP, when compared against patients with no such history (Table 3). After consulting with the CIT team members, the authors hypothesize that this may be due to a more receptive population. Patients who have a history of psychiatric illness have most likely received medical care or counseling in the past, and by better understanding the need for such care, are therefore more compliant with CSSP follow-up than those who do not have psychiatric illnesses. Similarly, the authors believe that those with a history of suicide attempts may be more willing to complete the 8-week program because repeat attempters are likely more cognizant of their condition as a problem and more likely to accept care, as compared to first-attempters who may deny that they have a mental health issue that needs to be addressed.
Logistic regression analysis of pre- and post-intervention outcomes.
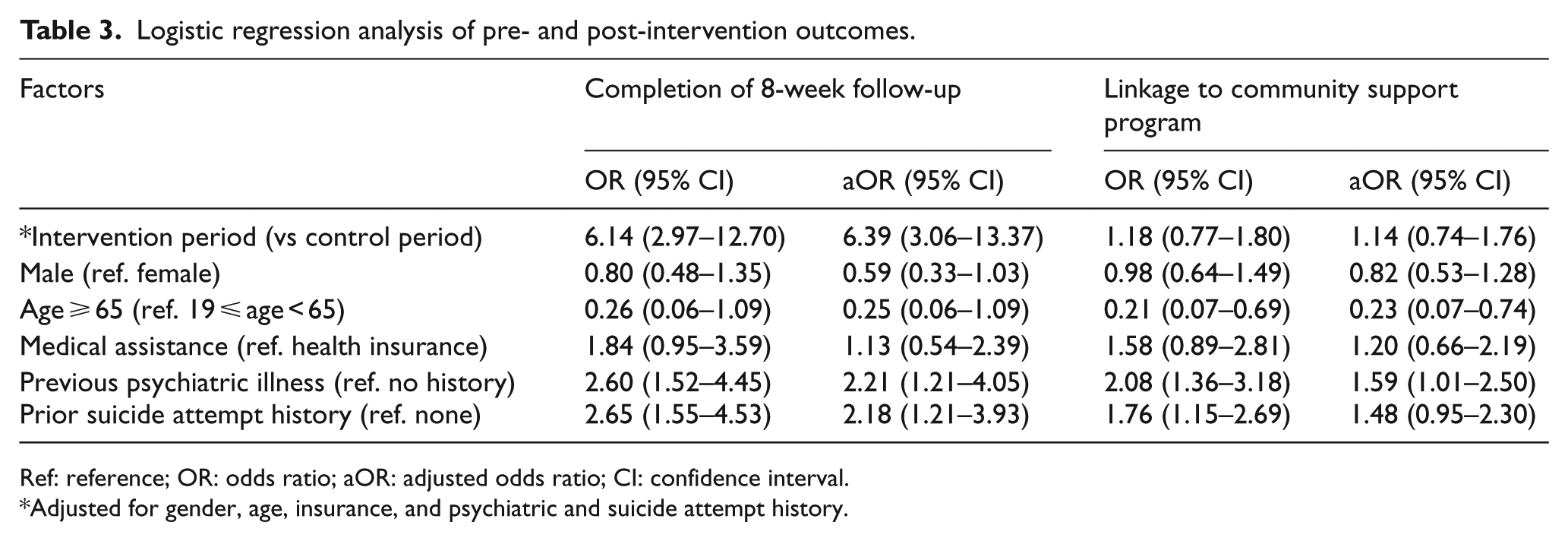
Ref: reference; OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval.
Adjusted for gender, age, insurance, and psychiatric and suicide attempt history.
Our study has a number of limitations. First, there was no method to reliably track subsequent suicidal behavior of the patient population. Future attempts may lead to visits to hospitals other than our own, and currently in Korea, privacy of information legislature is such that hospitals cannot share electronic medical records with one another. The authors would have been only be able to track patients who either presented to the same ED or were already enrolled in a counseling program and informed the CSSP of their subsequent attempts. However, it is known that the risk of suicidal ideation and behavior is higher immediately after discharge,7–13,25 and while our study did not track subsequent suicidal behavior, patients were followed up for a significant portion of the high risk post-discharge period. We are currently considering a telephone follow-up survey to conduct a wellness check on these patients to determine outcome. Second, there may be confounding factors that are unaccounted for, which contribute to the difference in outcomes between the control and intervention groups. In particular, because our study relies heavily on medical records, the reasons behind the suicidal behavior of our patients may not be fully accurate or detailed. Furthermore, our study is a before-and-after analysis without any defined controls, and as such, causality cannot be inferred from our study. Finally, as a single center study, our sample size is relatively small, and due to the nature of the socio-psychiatric landscape in Korea, in which suicide is extremely prevalent, our results may not necessarily be generalizable to other populations. Future replication of our methods may yield more conclusive evidence as to the generalizability of the intervention program.
Conclusion
An in-hospital counseling intervention for suicide attempt patients, focused on active and assertive counseling that begins in the ED, correlated with significantly increased completion rates of an 8-week follow-up counseling program. Linkage rates to CSSP programs did not improve significantly. However, in a hectic ED environment where it may be difficult to effectively counsel patients exhibiting suicidal behavior, such a program with dedicated personnel who can provide focused intervention and follow-up during the most delicate and susceptible period immediately after discharge may lead to more effective longer-term counseling and improvement in overall mental health. Further study is warranted to determine its applicability in other institutions, and the long-term re-attempt and mortality rates.
Supplemental Material
Supplement_table1 – Supplemental material for Effect of a Crisis Intervention Team for suicide attempt patients in an emergency department in Korea
Supplemental material, Supplement_table1 for Effect of a Crisis Intervention Team for suicide attempt patients in an emergency department in Korea by Eusang Ahn, Jooyeong Kim, Sungwoo Moon, Young-hoon Ko, Hanjin Cho, Jong-Hak Park, Ju Hyun Song, Han Na Kim, Ju Yeon Jee and Ra Young Han in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
The Crisis Intervention Team (CIT) was funded by the Ministry of Health and Welfare. The sponsor of CIT was not involved in the analysis and interpretation of data, in the writing of the manuscript, or in the decision to submit the manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Original data, materials, and reprints are readily available upon request.
Ethical approval
The study was approved by the internal ethics review board of Korea University Medical Center Ansan Hospital (IRB No. 2017AS0044), in compliance with the Informed Consent, Ethical Approval and Human Rights clauses set forth by the Hong Kong Journal of Emergency Medicine publishing guidelines.
Informed consent
The study was approved by the internal ethics review board of Korea University Medical Center Ansan Hospital (IRB No. 2017AS0044), in compliance with the Informed Consent, Ethical Approval, and Human Rights clauses set forth by the Hong Kong Journal of Emergency Medicine publishing guidelines. Individual consent was waived due to anonymized nature of patient data.
Previous Presentation
This paper was presented at the American College of Emergency Physicians (ACEP) Scientific Assembly in November 2016.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.