
Abstract
Introduction:
Aortic dissection is a clinical chameleon that can have variable presenting features that require a careful history and physical examination. A non-specific presentation of this life-threatening condition causes a diagnostic dilemma among clinicians especially in the emergency department leading to grave consequences.
Case Presentation:
We present a case of aortic dissection that presented as an acute bilateral blindness that was associated with a sudden onset of loss of consciousness and central chest pain. Bedside carotid ultrasound showed a double lumen carotid artery suggesting an intraluminal flap. Computed tomography angiography revealed extensive dissection of the entire length of the aorta.
Discussion:
This case illustrated the need for a high index of suspicion to diagnose patients with aortic dissection especially as the patient presented with an acute binocular visual loss and chest pain.
Conclusion:
A bedside carotid artery ultrasound in the emergency department was found useful in screening and diagnosing a carotid artery–related pathology.
Introduction
Classically, a patient with aortic dissection (AD) presents with a sudden onset of severe chest pain or back pain. 1 Some may occasionally come with an atypical presentation like blindness that usually manifests concurrently with other neurological deficits such as hemiparesis. 2 The most common visual symptom associated with this phenomenon is amaurosis fugax. Transient painless visual loss in a patient with acute AD is probably related to transient nerve ischemia of hypoperfusion. 2 A high index of suspicion is necessary for identification, timely diagnosis, and early repair of proximal AD to improve the outcome of these high-risk patients. We illustrate a case of acute binocular visual loss due to extensive AD involving bilateral carotid arteries. A combination of a high index of suspicious and prompt bedside carotid artery ultrasonography can be life saving.
Case presentation
A middle-age patient with underlying hypertension presented to the emergency department (ED) complaining of bilateral blindness after an episode of sudden loss of consciousness that lasted over an hour. She initially went to a general practitioner and was referred to a tertiary medical center for further management. Upon arrival, she was very concerned about her vision as the symptoms persisted. It occurred in association with a sudden onset of chest pain that radiated to the neck and epigastric area after she regained her consciousness. She graded her chest pain as moderate initially which later became severe throughout her visit in the ED. She denied other neurological deficits. Her blood pressure was 160/80 mmHg with a pulse rate of 90 beats per minute. Her oxygen saturation was 95% on room air but, and she was not tachypneic. On physical examination, she had a carotid bruit. There was no radio-radial or radio-femoral pulse delay, and no murmur was heard on precordial auscultation. Examination of her lungs revealed normal findings.
Electrocardiographic (ECG) examination showed left ventricular hypertrophy without evidence of acute ischemic changes. Serial ECG examination revealed no evolving ST-T segment changes. Chest radiograph revealed widened mediastinum with double density at the aortic knob and cardiomegaly (Figure 1). Non-contrast computed tomography (CT) of the brain also showed no significant abnormality.
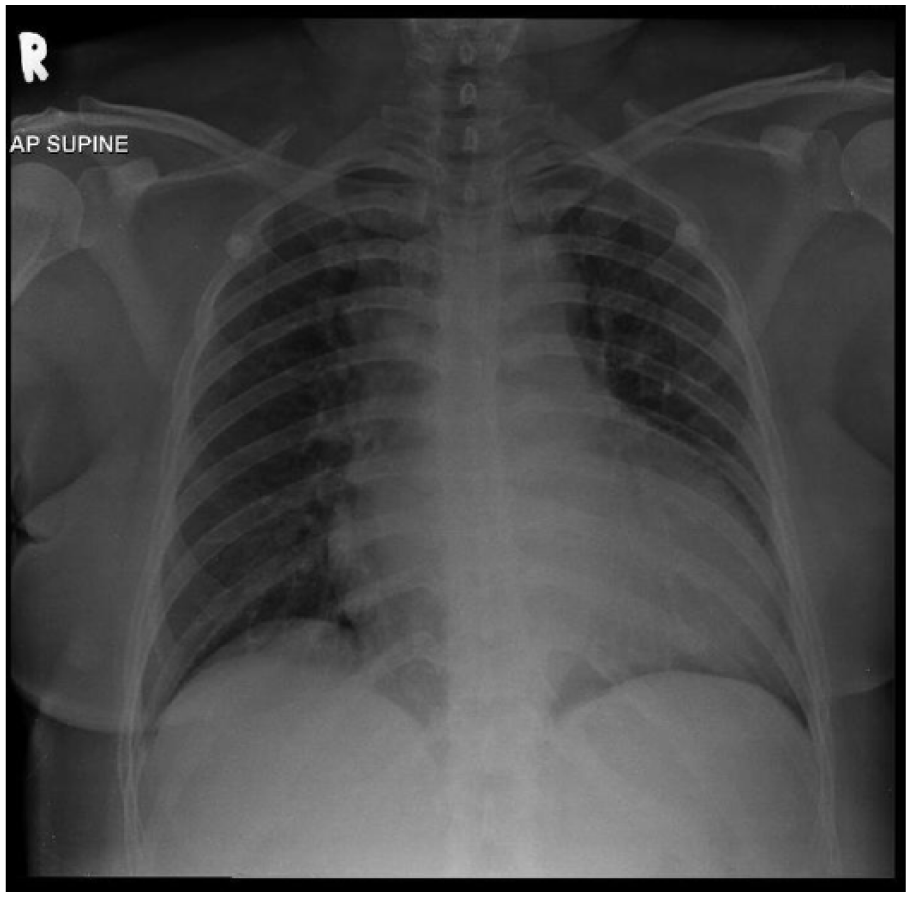
Chest radiograph anteroposterior view.
Her chest pain worsened despite a repetitive dose of analgesia. Bedside carotid ultrasonography revealed two lumens on her right and left carotid arteries suggesting a carotid artery dissection (Figure 2). The diagnosis was confirmed on CT angiography of the carotids, thoracic and abdominal aorta. It showed extensive dissection of the entire length of the aorta from the root of the aorta (Valsalva sinus) to the bilateral common iliac arteries. The dissection extended into both the common carotid arteries, internal and external carotids bilaterally. Other finding included a left renal artery thrombosis with left kidney devascularisation and infarction (Figure 3).
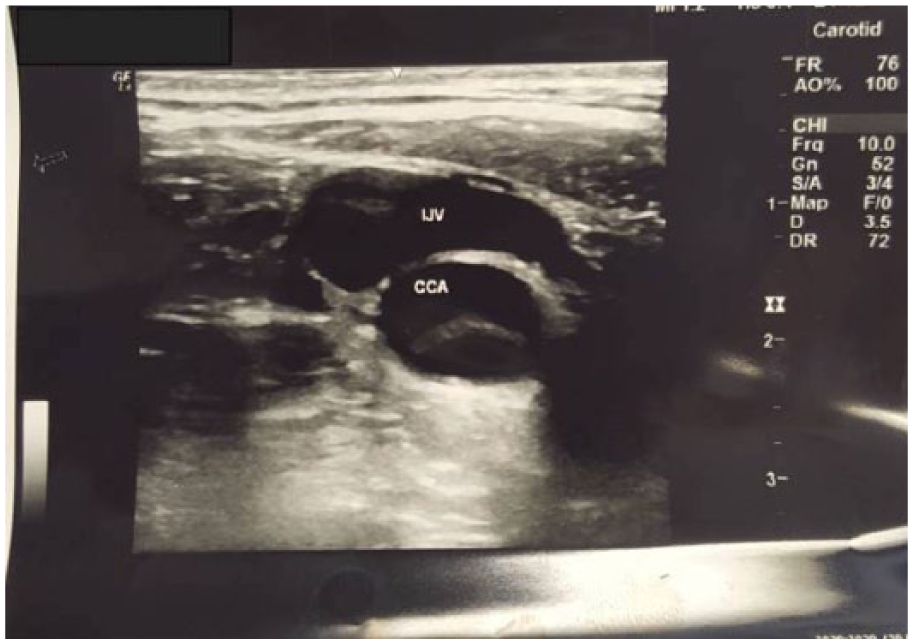
Carotid ultrasound image.
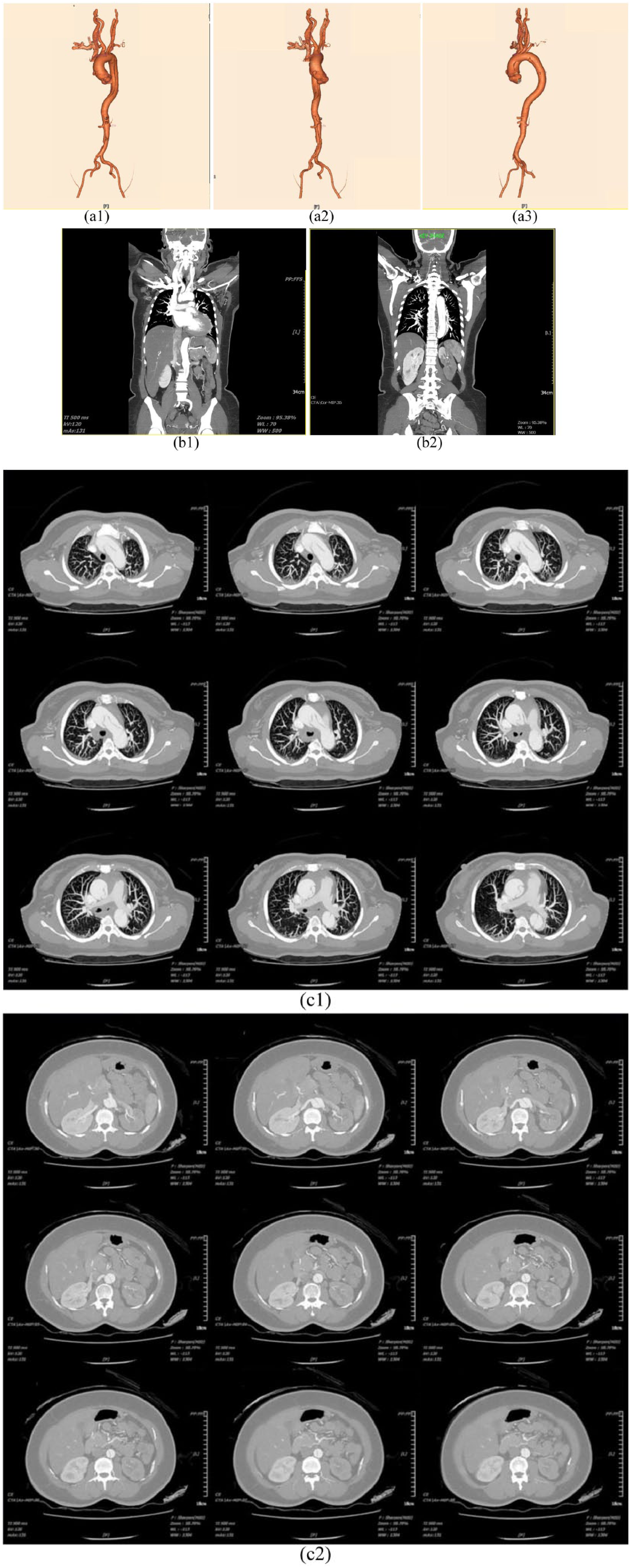
Computed tomography angiography of the carotids, thoracic and abdominal aorta. ((a1–a3) Three-dimensional reconstruction. (b1 and b2) Coronal view. (c1 and c2) Transverse view).
Her blood chemistries were unremarkable except for a serum potassium of 2.7 mmol/L. Her urea was 4.8 mmol/L, sodium 140 mmol/L, chloride 103 mmol/L, and creatinine of 76 mmol/L. Her total white cell count was 18.7 × 109/L, hemoglobin was 131 g/L, and platelet was 310 × 109/L. She was commenced on intravenous beta-blocker to control her blood pressure and her heart rate, and an opioid analgesic for pain relief and referred to the vascular team for further management. Her vision recovered spontaneously before admission to the vascular ward.
Discussion
A spontaneous AD is a lethal condition if left untreated. It is uncommon but a prompt diagnosis is essential. The incidence for AD is estimated at 5–30 cases per 1,000,000 population. This may however be an underestimate as almost 38% an AD has been misdiagnosed during first presentation. Many patients die before the admission or prior to the diagnosis of AD. 3 Similarly, a case of spontaneous internal carotid artery dissection is also rare. It has been estimated to occur in 2.5–3 cases per 100,000 population. 4 A internal carotid artery dissection usually affects a unilateral side. Only 2%–10% of internal carotid arteries dissection are bilateral. 5 The percentage of extensive AD involving carotid arteries has not been documented; however, there is literature on the condition. 6
This patient’s initial symptoms included chest pain, blindness, and loss of consciousness. Chest pain is the most frequent presentation in AD. Almost 95% of patients described the pain as an excruciating, tearing-like sensation that radiated from the back to the front. 3 In general, the nature and severity of the pain depend on the location of the dissection. Nevertheless, some cases of an AD may present with atypical or no pain. 3
Several published literature reported unilateral blindness as a rare presentation of an AD. To the best of our knowledge, there is no published report on an AD that presented with bilateral blindness as per this case. Kumar et al. described two cases of AD presenting with monocular blindness of the right eye. Both reported CT scan findings that revealed an AD extending from ascending aorta to the right common carotid artery. 7 Our patient presented with a history of loss of consciousness. Up to 13% of patient with AD may present with syncope due to symptoms of transient cerebral hypoperfusion. 3
During physical examination, we noted bilateral carotid bruits. We proceeded with a bedside ultrasonography that suggested a carotid artery dissection. Ultrasonography has indeed been used to diagnose AD. It is often the initial screening tool for unstable patients. Visualization of an intimal flap by ultrasound has a sensitivity of 67%–80% and specificity of 99%–100% for dissection. 8 Despite the lower sensitivity as compared to CT or magnetic resonance imaging (MRI), it has the advantage of being able to exclude other differential diagnoses in critically ill patients. Clinicians must keep a high index of suspicion for an AD when performing ultrasound involving any of the vasculatures such as looking for an intimal flap on an abdominal aorta examination or a dilated aortic root on a cardiac examination. In this case, a carotid ultrasound using a curvilinear probe revealed the hallmark of the AD, an intimal flap. The dissection was then traced to the origin of the aorta using a phased array probe utilizing both the standard transthoracic echocardiography views and the suprasternal notch as a window to the superior portions of the aortic arch. With the use of multiple image planes including unusual imaging windows such as the right parasternal, left parasternal, and paraspinal, the thoracic aorta can be imaged in its entirety increasing the accuracy of ultrasonography. 9 The usage of bedside ultrasonography is helpful in assisting the diagnosis of extensive AD. Positive ultrasound finding can lead to a prompt confirmation with a CT angiogram.
Conclusion
Prompt detection of an atypical presenting AD can be life saving. Extensive AD can present with bilateral blindness. Bedside carotid ultrasonography proved to be helpful especially in the such as this patient with clinical findings suggesting of carotid artery pathology. This can be accomplished only by an eyeballing technique without the need for complicated measurement of the carotid artery.
Footnotes
Acknowledgements
The authors wish to express their gratitude to the multidisciplinary members of emergency medicine team, cardiothoracic team, internal and anesthesiology team for their contribution, dedication, effort, and support in managing this case. Special thanks to Prof Dr Rusli Ismail and Dr Wan Zulkifli Wan Ibrahim for their contribution in scientific information in this article. All authors participated sufficiently in work and agreed to take public responsibility for appropriate portions of the contents.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data were primary and could be provided if required.
Informed consent
The patient was admitted for patient’s care, and she had been consented for investigation. However, she urgently referred to other institution for life saving surgical intervention. The authors have tried to obtain a consent to publish. Unfortunately, it was suspended due to failure to make contact with the patient or her relatives (consent form attached as a supplementary document). Patient’s anonymity was preserved, and this article does not contain any personal or demographic details that can be linked to patient’s identification.