
Abstract
Background:
The conventional chest pain protocol using thrombolysis in myocardial infarction score as the risk stratifying tool may not perform well in the emergency department in which a mix of low- and high-risk patients are encountered. Newer chest pain scores such as HEART pathway and Emergency Department Assessment of Chest Pain Score–Accelerated Diagnostic Protocol (EDACS-ADP) are found to have high sensitivity with good specificity.
Objectives:
This study aims to validate and compare two chest pain scores: HEART pathway and EDACS-ADP in the Accident and Emergency Department of a local hospital in Hong Kong.
Methods:
A prospective cohort study was carried out at the Accident and Emergency Department of Kwong Wah Hospital in Hong Kong from 1 June 2016 to 31 May 2017. Patients ⩾18 years old with chest pain lasting 5 min or more who were observed with chest pain protocol on observation ward were recruited.
Results:
A total of 238 patients were recruited; 231 eligible patients completed follow-up. There were five patients with major adverse cardiac events in 30 days of follow-up. The sensitivity, specificity, and negative predictive values of HEART pathway and EDACS-ADP were 100%, 74.3%, 100% and 100%, 73.5.0% and 100%, respectively. Both scores had almost the same performance in terms of major adverse cardiac events at 30 days (area under the curve = 0.87).
Conclusion:
Our study showed both EDACS-ADP (modified) and HEART pathway achieved high sensitivity (~100%) for detecting major adverse cardiac events in 30 days while being able to discharge more than 70% of patients as low risk for early discharge.
Introduction
Chest pain is an important complaint in patients attending the Accident and Emergency Department. According to a study in the United Kingdom, it accounts for around 6% of attendance to Emergency Department but ~27% of all admissions, 1 while in Hong Kong, it is estimated that 41,000 visits to all Accident and Emergency Departments in 2010 were due to chest pain. 2
The recommendation in American Heart Association 2015 guidelines for managing a patient with chest pain suspected of acute coronary syndrome is to observe the patient with serial electrocardiogram (ECG) and cardiac biomarker, referred to as chest pain protocol, followed by further risk stratification with a non-invasive test for inducible myocardial ischemia or anatomic evaluation of the coronary arteries. 3 The use of ECG together with cardiac biomarker alone cannot rule out acute coronary syndrome with 100% confidence because of the low sensitivity of the former in diagnosing acute myocardial infarction, with nearly 50% of transmural myocardial infarction demonstrating a normal or non-diagnostic ECG finding, 4 and the inability of the latter to rule out unstable angina. Thrombolysis In Myocardial Infarction (TIMI) score is traditionally incorporated into chest pain protocol to classify patients into low- or high-risk group. However, use of TIMI score in emergency department patients had been studied before but outperformed by newer risk scores. 5 There are a number of newer risk scores derived by emergency physicians to rule in an acute coronary syndrome with a high level of confidence (with an aim of >99% sensitivity and negative predictive value of >99%).6–9 HEART score (or pathway) and Emergency Department Assessment of Chest Pain Score–Accelerated Diagnostic Protocol (EDACS-ADP) are two which have better performance compared to others. The HEART score (Appendix 1) takes into account the History, ECG findings, Age, Risk factors for coronary artery disease, and Troponin level at 0 h. HEART pathway, in addition, differs from the HEART score, in that an extra troponin level test is taken at 3 h for testing. The HEART score (pathway) can identify up to 20% of patients as low risk for acute coronary syndrome while maintaining a good level of sensitivity (~99%) for 30-day major adverse cardiac events (MACE).10,11
EDACS-ADP score (Appendix 2), which stands for Emergency Department Assessment of Chest pain Score and 2 h Accelerated Diagnostic Protocol, was derived with logistic regression and its parameters included age, sex, risk factors for coronary artery disease, and clinical features of chest pain. The EDACS score was then combined with ECG findings and troponin levels at 0 and 2 h (the ADP) with a final sensitivity (⩾99%). The score derived was internally validated in another cohort of subjects in a local population of Australia. The EDACS-ADP score has excellent performance in classifying 40% to 50% of patients as low risk with a sensitivity of 99% to 100% for 30-day MACE. 12
While the HEART score (or pathway), having been externally validated,10,13 has a strong level of evidence and the EDACS-ADP score is a relatively new scoring system, there is scarce evidence to support the use of both scores in the local emergency departments. Thus, a study is carried out to investigate the applicability and comparison of the two scores in the emergency department of a local hospital in Hong Kong.
Methods/design
The study was a prospective cohort study. It was carried out at the Emergency Department of Kwong Wah Hospital which was an ~1400-bed hospital, providing a full range of acute service. The study period was from 1 June 2016 to 31 May 2017 inclusive. Approval was obtained from the Research Ethics Committee of Kowloon West Cluster before the study began. Patients recruited were those who presented to the emergency department with a complaint of chest pain. Inclusion criteria included patients who were ⩾18 years old, with chest pain lasting 5 min or more and the attending emergency physician decided to proceed to chest pain protocol in the observation ward. Exclusion criteria included patient with definite ST elevation myocardial infarction, obvious non-cardiac cause (e.g. Herpes zoster, pneumonia, trauma), mentally incapable of giving consent, terminal illness, pregnancy, or previously being recruited.
Consent from patients for enrolling into the study was taken by the investigators when they were admitted into observation ward for chest pain protocol observation. Parameters including gender, age, clinical features of chest pain, ECG findings, troponin levels at 0 and 3 h of observation, and risk factors for ischemic heart disease were collected. A checklist was prepared to aid investigators to collect the necessary data about the patient. Clinical features of chest pain were input by investigators after a direct interview with the patient. The ECG was reviewed by two emergency physician investigators separately. Any discrepancy in ECG findings between the two investigators was discussed and a final conclusion was reached. If no conclusion could be made, further opinion would be sought from a cardiologist.
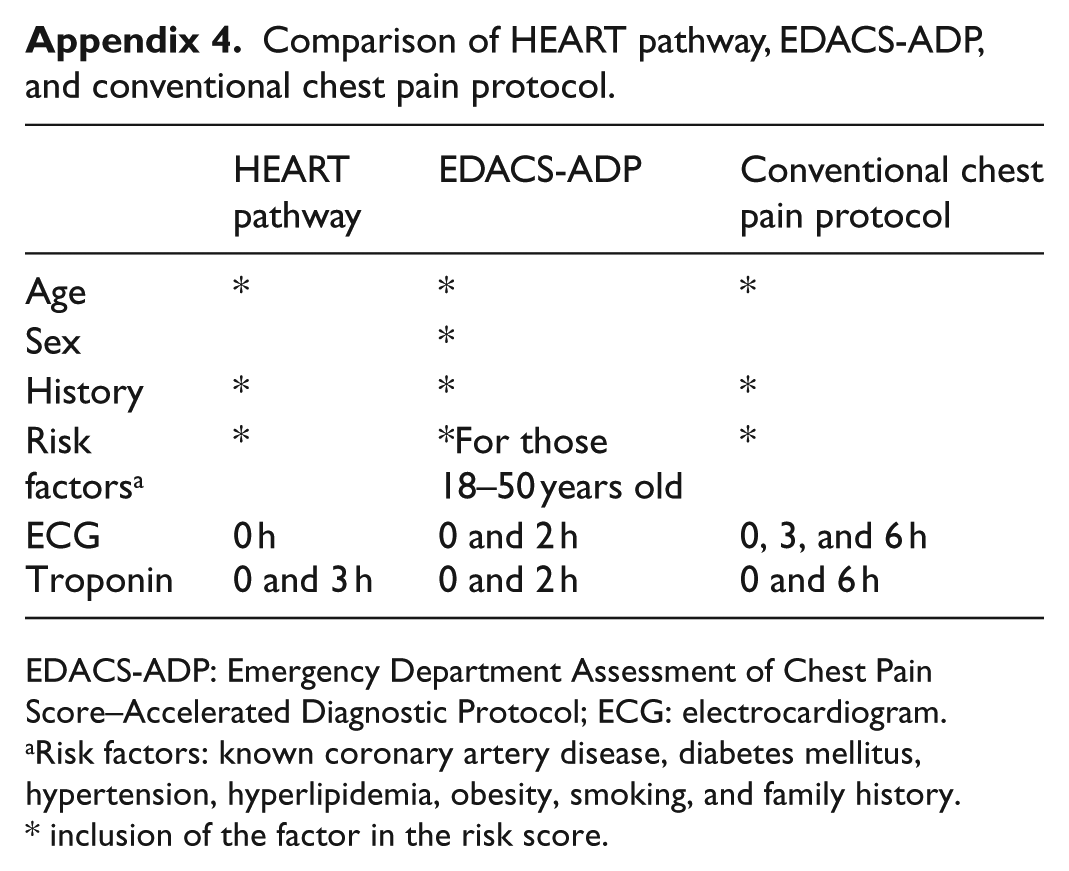
The conventional chest pain observation included serial troponin level tests at 0 and 6 h (Appendix 3). However, the HEART pathway and EDACS-ADP required second troponin level at 3 and 2 h, respectively. We decided to take extra troponin level test at 3 h only for calculating both algorithms to prevent the patient from multiple blood taking. Moreover, troponin level at 3 h would be more sensitive to detect myocardial infarction than the level at 2 h because it would rise with time after myocardial infarction. 14 A comparison of the three risk scores has been given in Appendix 4. The blood specimen was sent to the chemical laboratory of the hospital for analysis, which performed tests for troponin I with a reference of normal value <0.04 ng/mL (99th percentile). Computer medical record system (Clinical Management System), which provided linkage to the database in all public hospitals in Hong Kong, was used for aiding data collection.
The clinical judgment of the attending emergency physician was not affected by the two scores calculated initially. However, if the extra troponin level at 3 h was elevated, the patient would be admitted.
Outcome measures were defined as MACE in 30 days, which was in accordance with that adopted by the American Heart Association 2015 Guidelines. MACE referred to any cardiac arrest, ST elevation myocardial infarction, non-ST elevation myocardial infarction, emergency percutaneous coronary intervention, and coronary artery bypass graft that occurred within 30 days of subject recruitment. For every subject, the occurrence of MACE in 30 days was followed by retrieving the computer medical record at the Clinical Management System and telephone call. Telephone calls were made to identify those patients who had MACE in 30 days and attended private medical sector for management. The investigators who did the follow-up were blinded to the risk scores calculated.
Statistical analysis
The data collected were entered into and analyzed with SPSS, Version 23. Baseline analysis of the age, sex, clinical features of chest pain, ECG findings, troponin levels, and risk factors for coronary artery disease was done.
The HEART score and EDACS score were generated from the data with the SPSS program. Together with subsequent troponin and/or ECG results, the two scores were converted into HEART pathway and EDACS-ADP in which patients were categorized into low or high risk. The investigators doing the data entry and calculation of the risk scores were blinded to the MACE outcome. Patients with missing data were followed up to determine any MACE on them.
MACE in 30 days predicted using the two algorithms was compared to assess for their sensitivity, specificity, and negative predictive value. Sensitivity analysis was done for patients who were lost to follow-up to evaluate the effect on the final result.
Area under the curve (AUC) with its 95% confidence interval (CI) was calculated and receiver operating characteristic curve (ROC) was generated to assess and compare the diagnostic accuracy of the two algorithms.
The STARD (Standards for Reporting Diagnostic accuracy studies) 2015 reporting guideline was followed in the manuscript writing.
Results
During the period from 1 June 2016 to 31 May 2017, there were 238 subjects recruited (Figure 1). Three patients had missing ECG at 3 h in the computer system, and thus investigators were not able to review these ECGs. They did not have MACE in 30 days. Two patients had the patient record form incompletely filled for the part of chest pain characteristics, and thus the risk scores could not be calculated. One patient was recruited the second time into the study and was thus excluded. One patient was lost to follow-up. The patient who was lost to follow-up had mildly elevated troponin level (0.07 ng/mL, normal 99th percentile < 0.04 ng/mL) at 0 h and was admitted to the medical ward. However, he requested early discharge the same day and returned back to his own country. Since the troponin level test at 0 h was elevated, he was categorized as high risk for both EDACS-ADP and HEART pathway. The sensitivity and negative predictive values of the two risk pathways were not affected (both remained 100%) irrespective of whether MACE was assumed to have occurred in this patient when sensitivity analysis was done. Apart from this patient with borderline elevated troponin level, there was no MACE in the remaining six patients. Finally, 231 patients who had the full risk score calculated completed follow-up for MACE at 30 days through computer record retrieval and telephone call. Their baseline features were summarized in Table 1. HEART score and EDACS score were calculated for the 231 patients, and the patient distribution within each score was summarized in Figures 2 and 3. The majority of patients belonged to low-risk group. The distribution of patients was similar for both scores, with 171 patients (74.0%) belonging to low risk according to HEART score (⩽3) and 173 patients (74.9%) belonging to low risk according to EDACS score (<16).
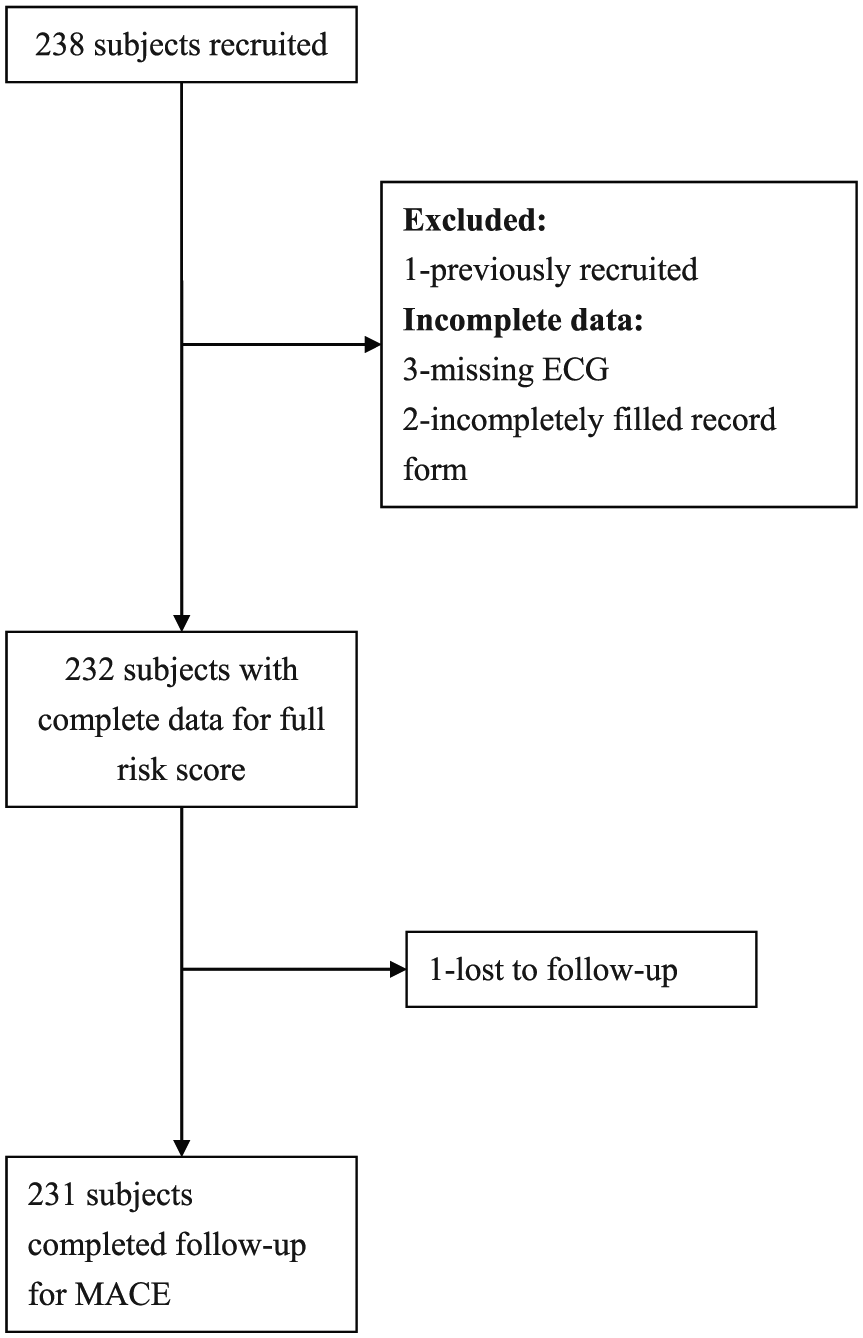
Enrollment flow diagram.
Baseline features of patients.
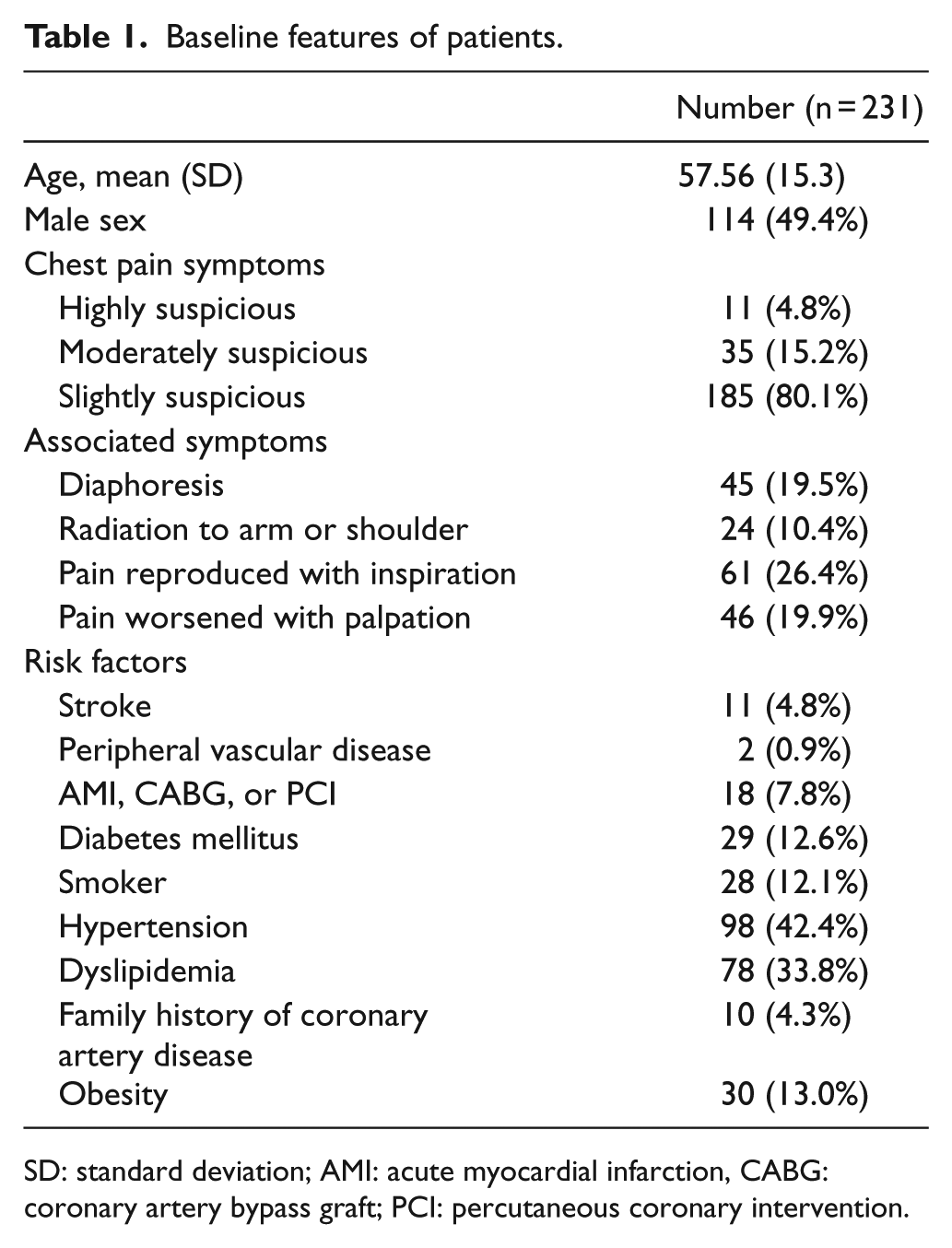
SD: standard deviation; AMI: acute myocardial infarction, CABG: coronary artery bypass graft; PCI: percutaneous coronary intervention.
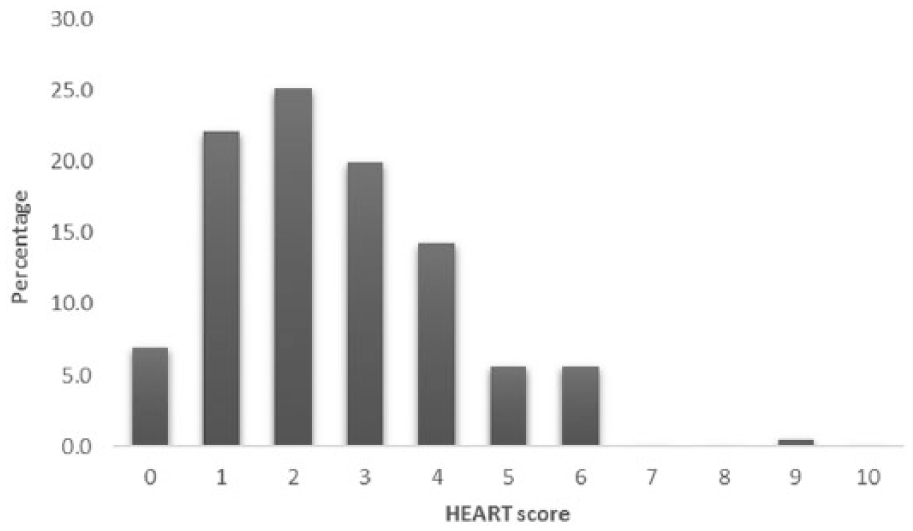
Percentage distribution of patients using HEART score (n = 231).
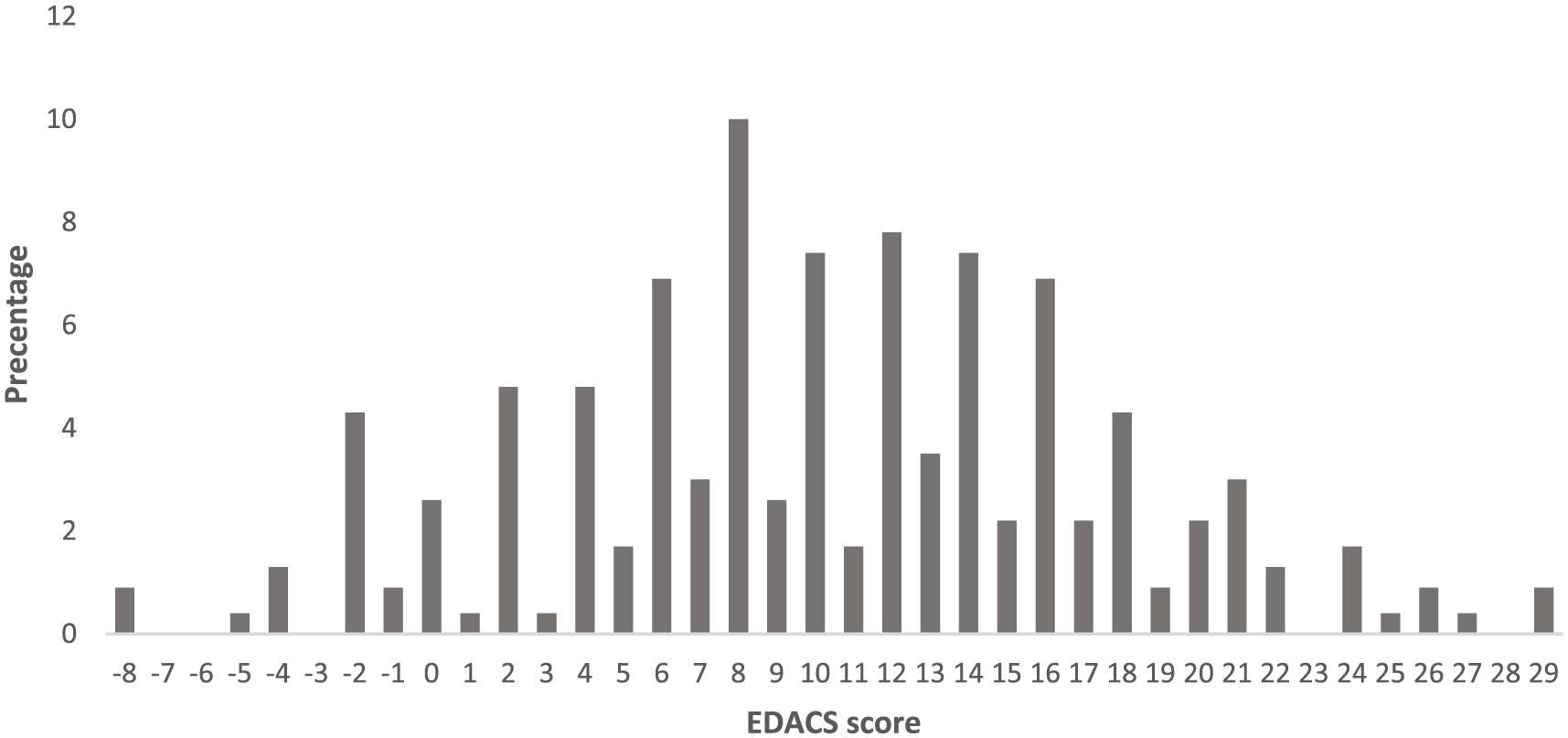
Percentage distribution of patients using EDACS score (n = 231).
There were five MACE, all were non-ST elevation myocardial infarction, in 30 days of follow-up. Two of the cases were categorized as low risk in both HEART score and EDACS score. The first patient was a 59-year-old man with a history of diabetes mellitus, hypertension, and peripheral vascular disease. He had a total EDACS score 13 and HEART score of 3 which made him low risk in both risk scores. The second patient was a 57-year-old man with a history of hypertension. He had an EDACS score of 14 and HEART score of 2. Both had a positive second troponin test at 3 h, leading to re-categorization into high risk in HEART pathway and EDACS-ADP (Table 2). The sensitivity, specificity, and negative predictive values of HEART pathway and EDACS-ADP were 100%, 74.3%, 100% and 100%, 73.5.0% and 100%, respectively. The ROC curve of the HEART score (pathway) and EDACS score (-ADP) were plotted in Figure 4. AUC with the 95% CI for both scores and the resultant HEART pathway and EDACS-ADP were calculated (Table 3). Both scores had almost same performance in terms of MACE at 30 days, with AUC = 0.87, 95% CI = 0.80–0.95 for HEART pathway and AUC = 0.87, 95% CI = 0.79–0.94 for EDACS-ADP.
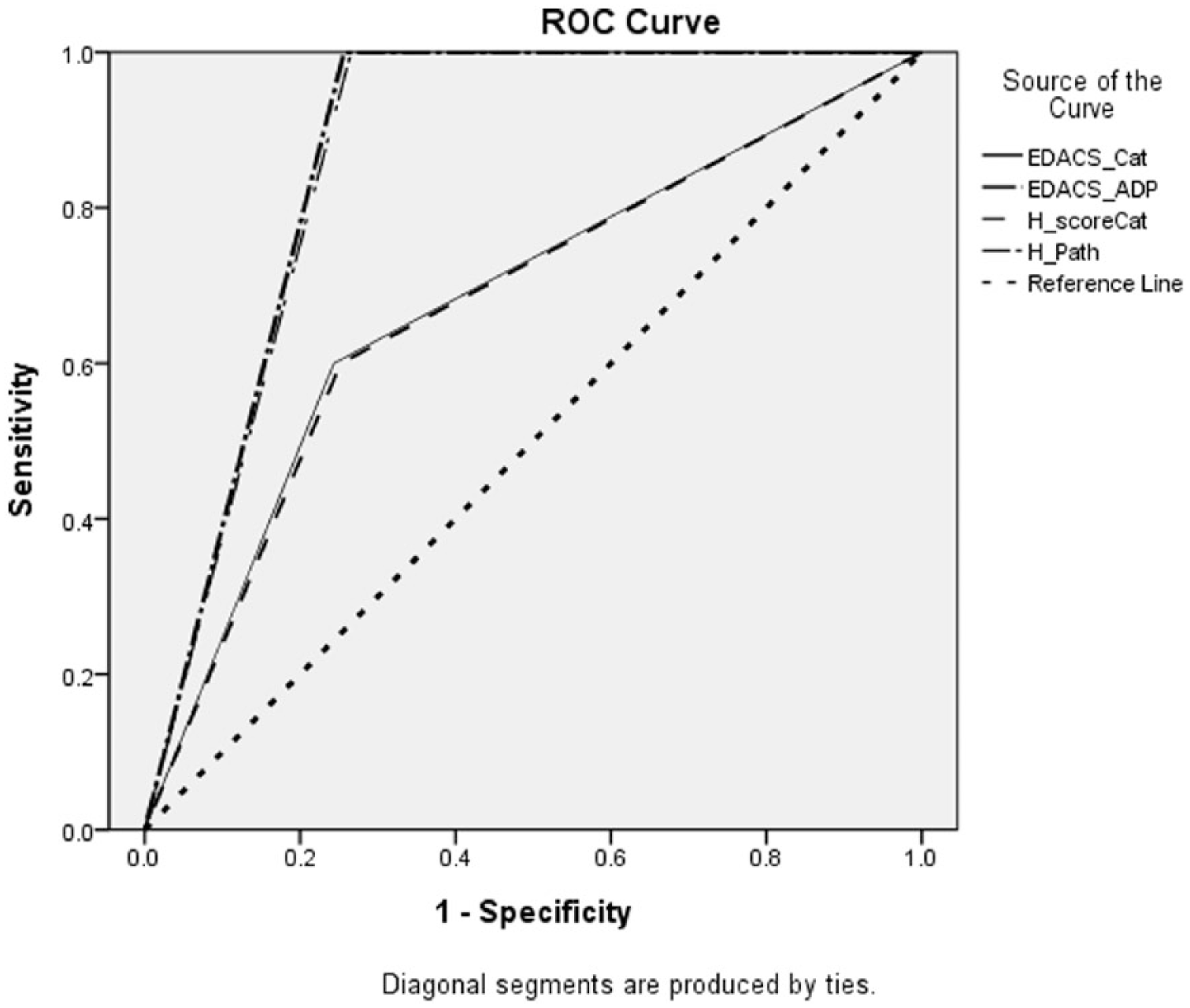
The ROC curves for HEART and EDACS algorithm.
Occurrence of MACE in 30 days in risk categories of HEART pathway and EDACS-ADP.
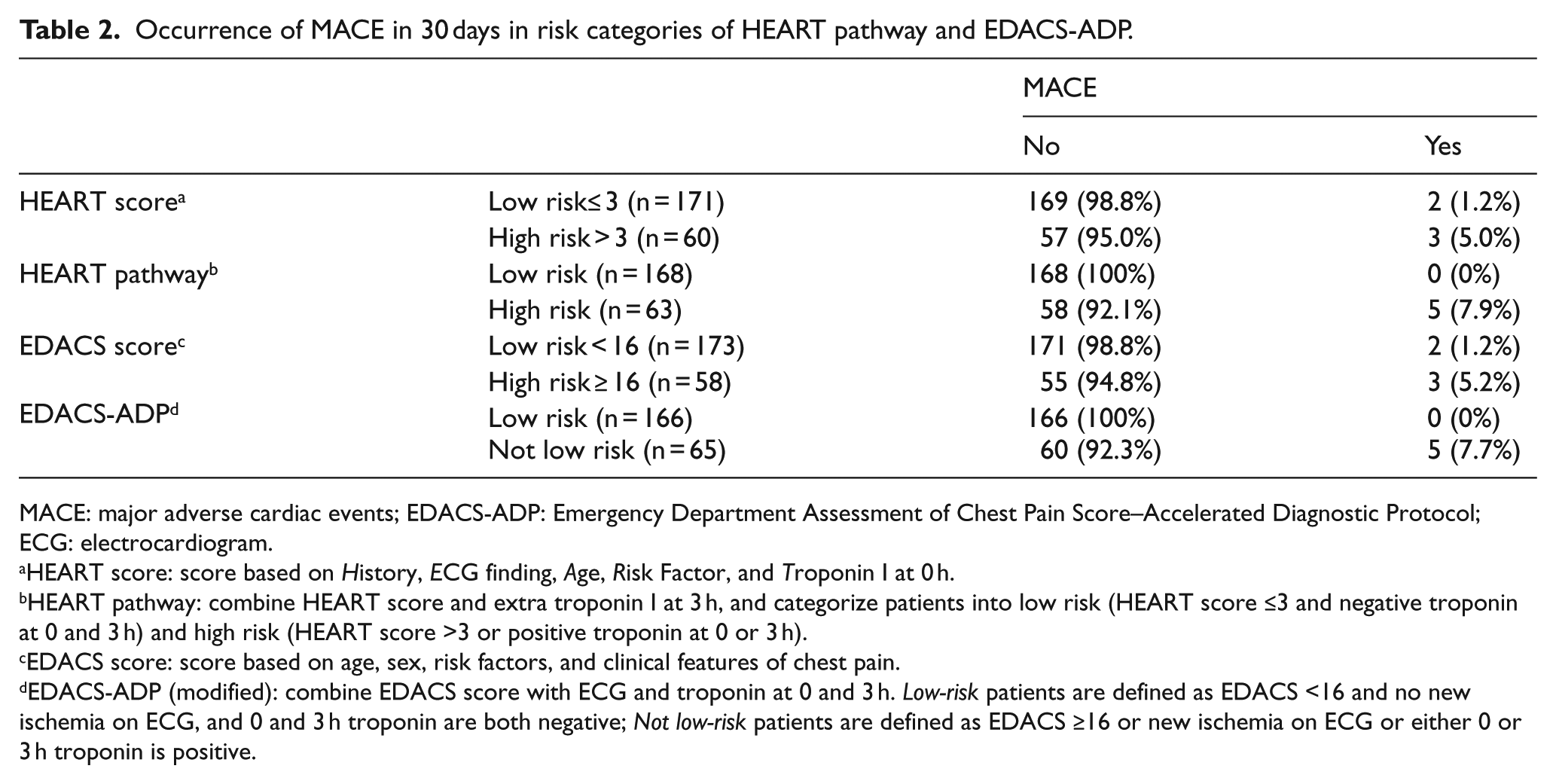
MACE: major adverse cardiac events; EDACS-ADP: Emergency Department Assessment of Chest Pain Score–Accelerated Diagnostic Protocol; ECG: electrocardiogram.
HEART score: score based on History, ECG finding, Age, Risk Factor, and Troponin I at 0 h.
HEART pathway: combine HEART score and extra troponin I at 3 h, and categorize patients into low risk (HEART score ≤3 and negative troponin at 0 and 3 h) and high risk (HEART score >3 or positive troponin at 0 or 3 h).
EDACS score: score based on age, sex, risk factors, and clinical features of chest pain.
EDACS-ADP (modified): combine EDACS score with ECG and troponin at 0 and 3 h. Low-risk patients are defined as EDACS <16 and no new ischemia on ECG, and 0 and 3 h troponin are both negative; Not low-risk patients are defined as EDACS ≥16 or new ischemia on ECG or either 0 or 3 h troponin is positive.
The AUC for HEART and EDACS algorithm.
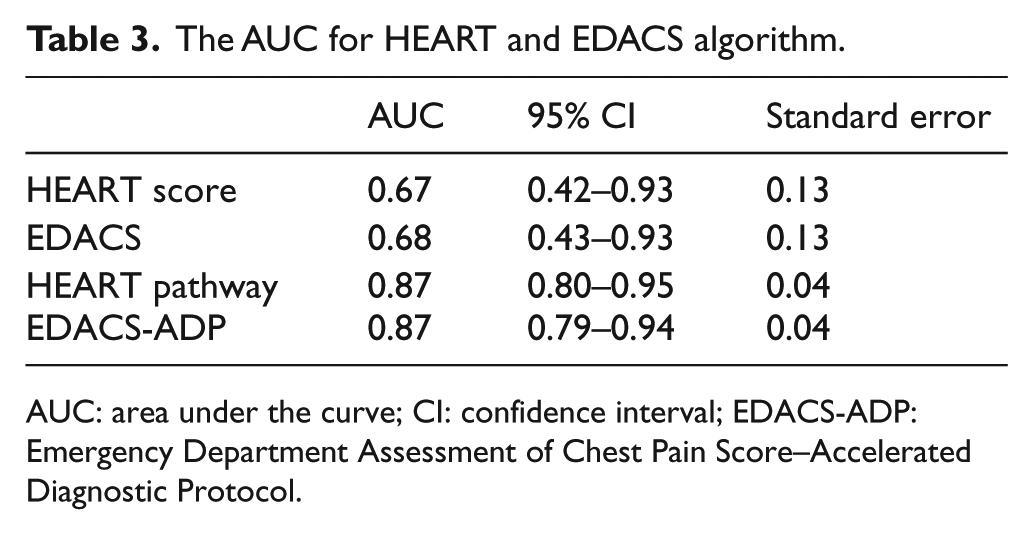
AUC: area under the curve; CI: confidence interval; EDACS-ADP: Emergency Department Assessment of Chest Pain Score–Accelerated Diagnostic Protocol.
Discussion
The conventional chest pain protocol using TIMI score as the risk stratifying tool had its limitation. It was derived for use in high-risk patients who had unstable angina or non-ST elevation myocardial infarction. The score might not perform well in emergency departments in which a mix of low- and high-risk patients was encountered. According to a meta-analysis by Hess et al., 15 the sensitivity of TIMI score in identifying patients with MACE in 30 days was ~97%, with ~20% of patients identified as low risk for early discharge if a TIMI score <1 was used as the cutoff line. While the study by Than et al. 16 with a total of 3582 subjects and a TIMI score <1 as the cutoff was able to achieve a sensitivity of 99.3% (95% CI = 97.9%–99.8%), only 9.8% of patients were discharged as low risk. This contrasted with the study of HEART pathway by Mahler et al. 10 in which 1005 subjects were recruited. It had a sensitivity of 99% (95% CI = 97%–100%) for ACS and allowed early discharge of 20% (95% CI = 18%–23%) of subjects. The EDACS-ADP score also had good performance with a sensitivity of 99% to 100% for 30-day MACE and classified 40% to 50% of patients as low risk for early discharge in a study by Than et al. 12 which had a total of 2582 subjects.
An external validation of the HEART pathway by Oliver et al. 17 after implementation of a HEART pathway outpatient disposition pathway included 449 patients with 25 subjects having 6-week MACE. The study had a sensitivity of 100% for 6-week MACE and discharged 36.5% of patients as low risk for outpatient assessment. Flaws et al. 18 studied the implementation of EDACS-ADP at a hospital in Canada. Of the 763 patients recruited, 41.6% were classified as low risk for early discharge and the sensitivity for 30-day MACE was 100%. Our study tried to apply and validate the two scores in a local emergency department. The results from our study were comparable to that in previous studies, in which there was a sensitivity of ~100% for MACE in 30 days. However, we had more than 70% (for HEART pathway: 168/231 = 73%; EDACS-ADP: 166/231 = 72%) of patients identified as low risk for early discharge after 3 h of observation. This percentage was high compared to previous studies.10–12,17,18 This was probably related to the differential admission of high-risk patients with multiple comorbidities into the hospital for further treatment instead of managing them with chest pain observation protocol at observation ward. This explained why there was a higher percentage of low-risk patients in our study and thus a higher percentage of patients allowed earlier discharge. This might also account for the relatively lower percentage of patients (2.2%) with MACE in 30 days in our study compared to other similar studies by Oliver et al. 17 (5.56%) and Flaws et al. 18 (10.4%).
Limitations
This study had several limitations. It had a relatively small sample size and was a single-centered study which might affect its generalization to other centers as other centers may have different mix of patients due to the locality they are situated. Further large-scale multi-centered studies could be carried out in the future to improve the validity. There existed the presence of recruitment bias. Most of the subjects recruited belonged to low-risk patients, in which relatively few MACE were expected to occur. This might reflect the differential admission of high-risk patients with multiple comorbidities into the hospital instead of observing them on the observation ward. Besides, as the second troponin I test in our study was taken at 3 h instead of 2 h, the EDACS-ADP was more accurately called the modified EDACS-ADP scoring. Finally, our study mainly aimed at validating the sensitivity of two chest pain scoring algorithms in detecting MACE in 30 days in a local population. The sample size did not have the adequate power to compare the effectiveness of the two scoring systems, in which the difference might be small. However, this secondary outcome was of less importance in our study.
Conclusion
Our study showed that both EDACS-ADP (modified) and HEART pathway achieved high sensitivity (~100%) for detecting MACE in 30 days while being able to discharge ~70% of patients who belonged to low-risk group for early discharge. This showed that the two chest pain scoring algorithms were accurate and could apply to our local emergency departments. Further large scale multi-centre studies are required to verify the application (external validation) in other hospitals.
Footnotes
Appendix
Comparison of HEART pathway, EDACS-ADP, and conventional chest pain protocol.
| HEART pathway | EDACS-ADP | Conventional chest pain protocol | |
|---|---|---|---|
| Age | * | * | * |
| Sex | * | ||
| History | * | * | * |
| Risk factors a | * | *For those 18–50 years old | * |
| ECG | 0 h | 0 and 2 h | 0, 3, and 6 h |
| Troponin | 0 and 3 h | 0 and 2 h | 0 and 6 h |
EDACS-ADP: Emergency Department Assessment of Chest Pain Score–Accelerated Diagnostic Protocol; ECG: electrocardiogram.
Risk factors: known coronary artery disease, diabetes mellitus, hypertension, hyperlipidemia, obesity, smoking, and family history.
inclusion of the factor in the risk score.
Acknowledgements
We would like to thank Professor Benny CY Zee for the valuable advice on the study and Clinical Research Center of Kwong Wah Hospital for the assistance provided.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Research data can be obtained upon request.
Ethical approval
Approval was obtained from the Research Ethics Committee of Kowloon West Cluster in February 2016 before the study began.
Informed consent
Written informed consent was obtained from each patient included in the study.
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.