
Abstract
Background:
Acute myocardial infarction is one of the most common causes of mortality in developed countries, and high-sensitive troponin test usually becomes positive within 3 h from the onset of symptoms. Myocardial perfusion index (Tei index) is a parameter measured during the echocardiographic examination.
Objectives:
The aim of this study is to investigate the diagnostic value of the Tei index for early diagnosis of acute myocardial infarction in the emergency department and to evaluate the correlation between the Tei index and Hs-Troponin value.
Materials and Methods:
A total of 129 cases were evaluated, and patients were divided into two groups according to their final diagnosis as “acute myocardial infarction (non-ST segment elevation myocardial infarction)” and “non-acute myocardial infarction” groups. Baseline and third-hour Hs-Troponin levels and Tei index values were determined, and their correlation was analyzed.
Results:
A total of 84 cases were diagnosed with acute myocardial infarction (non-ST segment elevation myocardial infarction), 84.5% had positive Tei index results at the time of admission while the remaining 45 patients were diagnosed as non-acute myocardial infarction and only 48.9% of them had positive Tei index. The diagnostic value of the Tei index and Hs-troponin were calculated as 79.8% and 60%; 67.9% and 60%, respectively. Also, we found that a 0.02 or more increase in the Tei index value has a 97.6 sensitivity and 97.5 specificity for the diagnosis of non-ST segment elevation myocardial infarction. A weak correlation was found between the Tei index and Hs-Troponin values in the acute myocardial infarction group (r = 0.425) and a negative correlation in non-acute myocardial infarction patients at presentation.
Conclusion:
It is suggested that the use of Tei index might be used as a supportive measure for the early diagnosis of acute myocardial infarction, and the deterioration of Tei index seems to be more significant than Hs-Troponin especially in ruling out acute myocardial infarction.
Introduction
In the United States, chest pain is the second most common (9.6%) complaint among emergency department (ED) presentations. 1 However, life-threatening conditions are detected only in a minority of these patients. Several studies have reported that 4% of such cases were diagnosed with acute myocardial infarction (AMI), 7.5% with unstable angina pectoris (USAP) and stable coronary disease, and less than 1% with pulmonary embolism and aortic dissection.1,2
History and physical examination are often not sufficient enough to obtain the final diagnosis. Cardiac markers are currently the most important diagnostic tests. Hs-Troponin is one of the novel markers showing cardiomyocyte necrosis. Unlike other troponin assays, detection is possible even when there are 1000 necrotic cells in the circulation. These new-generation troponin assays have higher diagnostic accuracy, enabling early diagnosis of AMI. 3 However, Hs-Troponin levels can be affected by various conditions including chronic kidney disease, cerebrovascular disease, and congestive heart failure. Besides, the turnaround time is longer. Therefore, other supportive methods are needed for early diagnosis of non-ST segment elevation myocardial infarction (NSTEMI).
In this sense, Doppler echocardiography is one of the most important diagnostic tools used to support cardiac markers in the diagnosis of the acute coronary syndrome (ACS). Its advantages include the possibility to perform at the bedside and the ability to detect other diseases involved in the differential diagnosis. First described by Chuwa Tei in 1995, Tei index, which is also known as the myocardial performance index (MPI), is derived from Doppler echocardiography. It reflects left ventricular global systolic and diastolic dysfunctions, where ejection fraction (EF) performed with echocardiography reflects only the systolic dysfunction. 4 It shows good correlation with invasive cardiac examination findings. In AMI, both systolic and diastolic functions are impaired, and studies have shown that Tei index is a practical, non-invasive method that is not affected by anatomical or geometrical properties of the left ventricle5,6 and a valuable clinical tool.7,8 It was found to be below 0.4 in healthy adults without any comorbid disease.5,9
In this study, the primary aim was to evaluate the diagnostic utility of the Tei index in NSTEMI compared to Hs-troponin levels at the initial presentation, especially in the early phase even when troponin results were negative. Secondarily, it is aimed to investigate the correlation between the Tei index and Hs-Troponin values.
Methods
Study design and setting
This prospective, observational, diagnostic accuracy study was conducted at Fatih Sultan Mehmet Education and Research Hospital, in Istanbul with an annual patient load of 220.000. Our prospective cohort consisted of 200 consecutive patients with ischemic-type chest pain who presented to the ED between 1 December 2015 and 31 June 2016. The local ethics committee approved this study.
Selection of participants
All consecutive adult patients (age ≥18 years) who were admitted to the ED with ischemic-type chest pain during the working shifts of the researchers were eligible for study inclusion. Patients were included in the study if any of the following criteria were not present: ST segment elevation myocardial infarction (STEMI) according to electrocardiogram (ECG), history of moderate to severe aortic insufficiency, recent AMI (3 months), history of heart failure or impaired EF, history of impaired renal function, history of cerebrovascular disease, history of trauma which could cause cardiac contusion, heart rate ≥120 bpm, active infection, suspicion of sepsis and/or shock, or pregnancy. Patients (1) who were diagnosed with USAP by the cardiologist, (2) who developed cardiac arrest during their ED stay, or (3) who had poor echocardiographic imaging were excluded from the study cohort.
Definitions
The third universal definition of myocardial infarction (MI) provided an international consensus on the classification of myocardial injury and infarction. 10 According to clinical classification, MI was categorized into five groups: (1) MI due to a primary coronary event (type I MI), (2) MI secondary to an ischemic imbalance (type II MI), (3) cardiac death due to MI (type III MI), and (4) MI associated with revascularization procedures (type IV and V MI).
Ischemic-type chest pain was described in the presence of symptoms suggestive of myocardial ischemia, which often include combinations of chest, jaw, upper extremity or epigastric discomfort with exertion or at rest; and which lasts ≤20 min, which is usually diffuse, not positional, or not affected by movement of the region and which may be presented with associated symptoms such as dyspnea, diaphoresis, nausea, or syncope. 11
The diagnosis of AMI according to the World Health Organization (WHO) was described in the presence of one of the following: (1) ECG showing absolute pathological Q waves and/or ST-segment changes in serial recordings; (2) history of typical or atypical angina pectoris, together with specific changes on the ECG and elevated enzymes; (3) history of typical angina pectoris and elevated enzymes with no changes on the ECG; and (4) pathological evidence in fatal cases, appearance of fresh MI and/or recent coronary occlusion at autopsy. 11
Data collection and study protocol
The baseline characteristics of all patients including age, sex, vital findings, comorbidities, clinical symptoms, risk factors for ACS, and the presence of other diseases were recorded for all chest-pain patients presenting to the ED. Patients were managed by their attending emergency physicians (EP) according to the recent AHA/ESC guidelines, without any intervention in their management decisions. When an eligible patient was presented to the ED according to the criteria mentioned above, a researcher on duty was alerted for the evaluation of the patient for study inclusion. Blood biochemistry, Hs-troponin, and electrocardiography (ECG) were obtained as a part of the routine workup. If STEMI was present, the patient was excluded from the study. At the primary contact, non-AMI and NSTEMI patients were evaluated by transthoracic echocardiography (TTE) as described below. The first echocardiographic assessment was performed at the time of presentation, and the second at the third hour of presentation, if possible. Then, all patients were managed without any intervention. The researchers were blinded to the clinical situations and the treatment plans. In our center, emergency percutaneous transluminal coronary angioplasty (PTCA) was not available. Therefore, patients requiring emergency PTCA were transferred to the nearest PTCA center 11 km away, according to the final diagnosis and decision of the consulting cardiologist. Based on the definitive diagnosis of the consulting cardiologist, patients were evaluated in AMI (n = 84) and non-AMI (n = 45) groups. The AMI group included only cases with the final diagnosis of NSTEMI. Patients with all other diagnoses (pulmonary embolism, myocarditis, pneumonia, pneumothorax, acute pancreatitis, and costochondritis) were included in the non-AMI group. Four myocarditis patients were categorized as lost-to-follow-up as they were transferred to the PTCA center after the initial evaluation. Therefore, those four patients were not included in the analysis of the third-hour control parameters.
Measurements
Echocardiographic measurements
All researchers have completed an echocardiography training, including didactic and practical sessions, with a minimum of 50 examinations as a part of our curriculum. Before the study, the principal researcher (who was an EP) of the project completed 2 h of theoretical and hands-on training with 20 patients led by an experienced cardiologist. The researcher and the cardiologist examined 10 randomly selected patients and calculated the Tei index values blinded to each other. Analysis of these measurements showed 98% agreement between the cardiologist and the EP.
Two-dimensional (2D) and pulse-wave Doppler imaging according to the recommendations of the American Society of Echocardiography using a commercially available system was performed (Philips Medical Systems IE33 Ultrasound, Bothell, USA). Subjects were examined in the left lateral recumbent position using standard apical views (two chambers, four chambers, and long axis) from left fourth to fifth intercostal space with a 2–5 Hz phased array probe. Pulse-wave Doppler imaging was performed from the lateral or medial wall of the mitral annulus. Tei index was calculated from recordings of three consecutive cardiac cycles with simultaneous electrocardiography as previously described5,6,9 (Figure 1). Then, LV Tei index was computed using the following equation: [isovolumetric contraction time (IVCT) + isovolumetric relaxation time (IVRT)]/LV ejection time (ET) = a − b/b (Figure 2). In our study, we accepted LV Tei index > 0.40 values as a proof of LV dysfunction.12–14
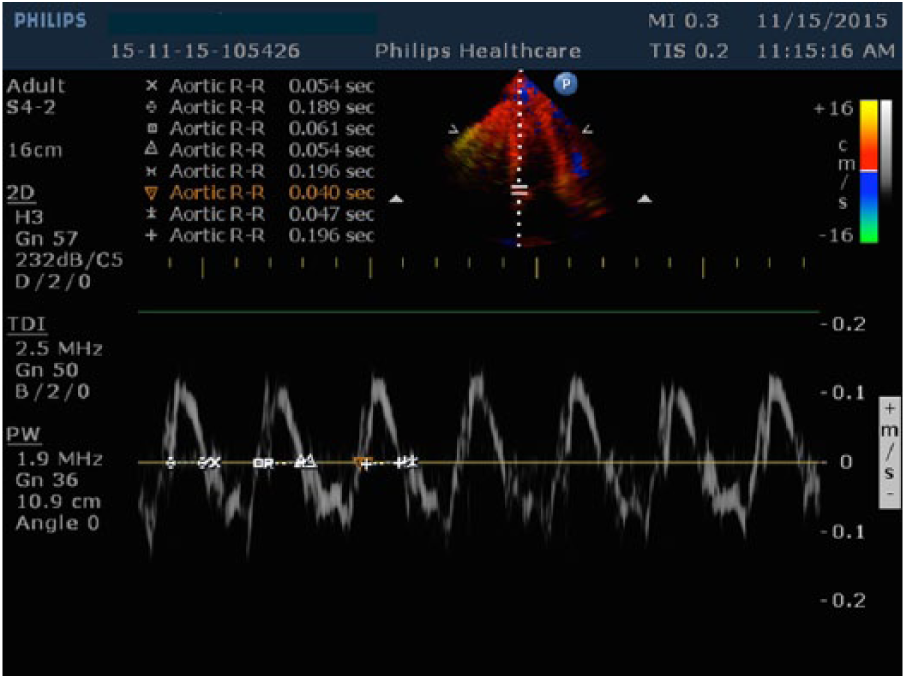
Calculation of Tei index from medial wall of mitral annulus in PW-Doppler mode.
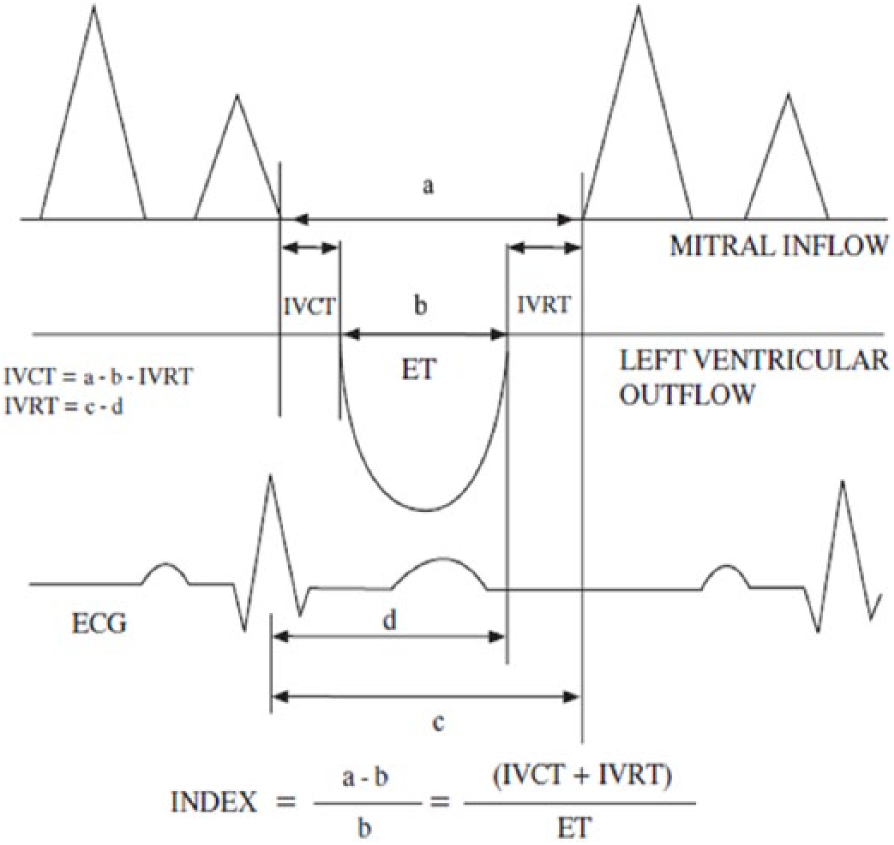
LV Tei index was calculated as: [Isovolumetric contraction time (IVCT) + isovolumic relaxation time (IVRT)]/LV ejection time (ET) = (a − b)/b (12).
Biochemical measurements
Hs-Troponin levels were measured using the Abbott Architect Hs-Troponin assay. According to the European Cardiology Association 2015 NSTEMI guideline, the cut-off values are specific to the assay. As recommended in European Cardiology Association 2015 NSTEMI guidelines, blood samples for measurement of Hs-Troponin were obtained at the time of presentation and the third hour. 15 Also, according to the same guideline, a hs-troponin level of 15.6 pg/mL for women and 34.2 pg/mL for men was accepted as the threshold for a positive result.
Statistical analysis
Continuous variables were reported with means, standard deviations, and 95% confidence intervals (CIs) or medians and interquartile ranges according to the distribution pattern of the variable assessed by the Shapiro–Wilk test. Normally distributed variables were compared among independent groups with Student’s t-test or analysis of variance (ANOVA), and Mann–Whitney U test or Kruskal–Wallis test for non-normal distributions. Dependent groups were compared using paired sample t-test, or Wilcoxon sign test for normal and non-normal distributions, respectively. Proportions were compared among discrete groups by chi-square test and Fisher’s exact test with Continuity (Yates) Correction. The association between parameters was evaluated with Pearson’s r. The sample size was estimated as 112 for the non-inferiority of two diagnostic tests within a margin of 0.15 in the sensitivities for the power of 80% with a Type 1 error of 5%. 16 Statistical analysis of the data was performed using IBM SPSS Statistics 22 (IBM, USA). In this study, the accepted Type 1 error was 5%.
Results
A total of 200 patients were enrolled, 71 patients were excluded, and 129 cases were evaluated in this study. The flow diagram of the patients is presented in Figure 3. Demographics, medical history, outcomes, measurements, and laboratory findings are summarized in Table 1. Hs-Troponin levels were obtained, and Tei index measurements were performed in 129 patients at the presentation and in 125 patients at the third hour (Tables 1 and 2). The minimum Tei index value observed in the NSTEMI group at the third hour was 0.42.
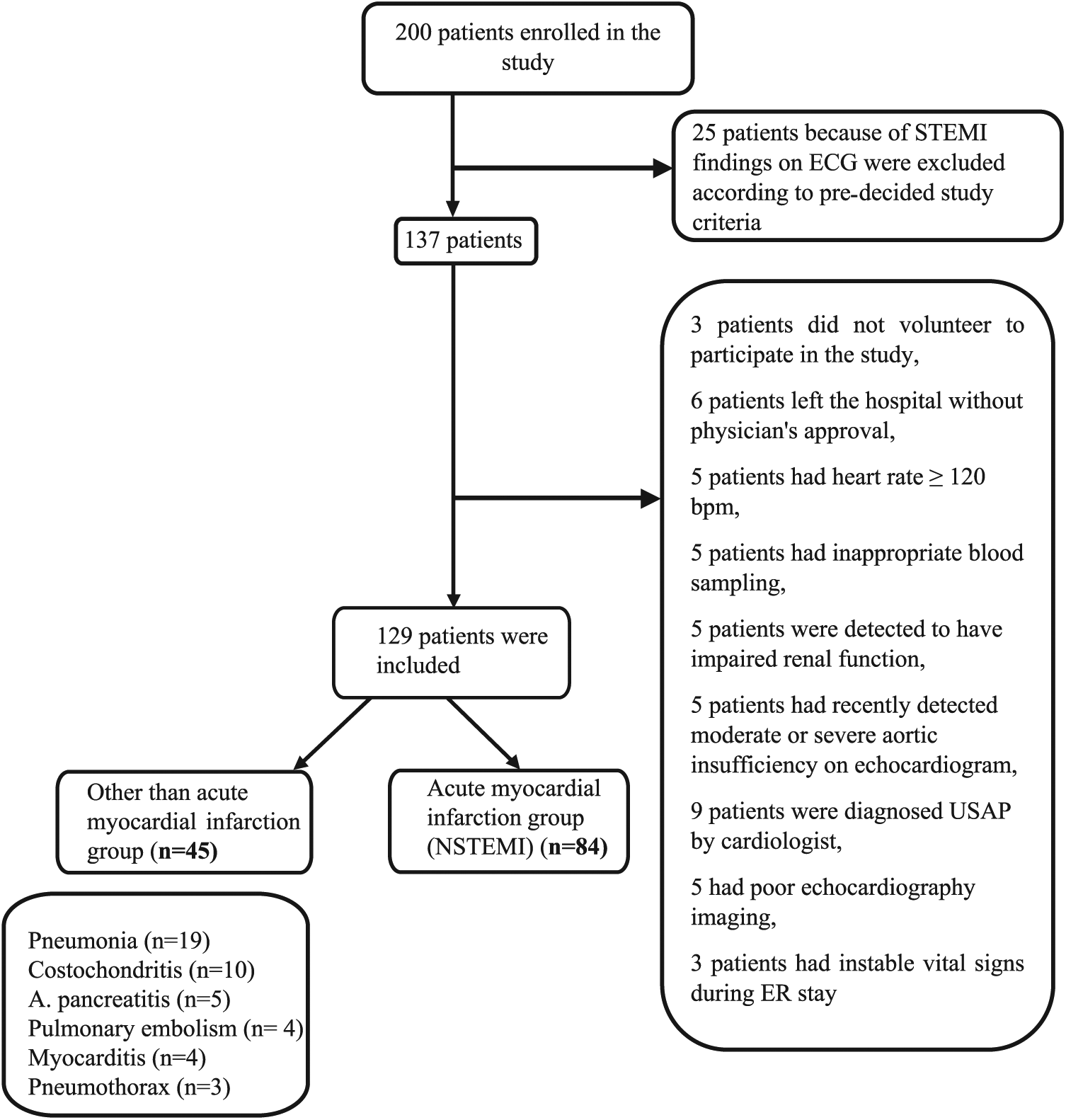
Patient flow diagram.
Demographics of the patient population according to outcome measures.
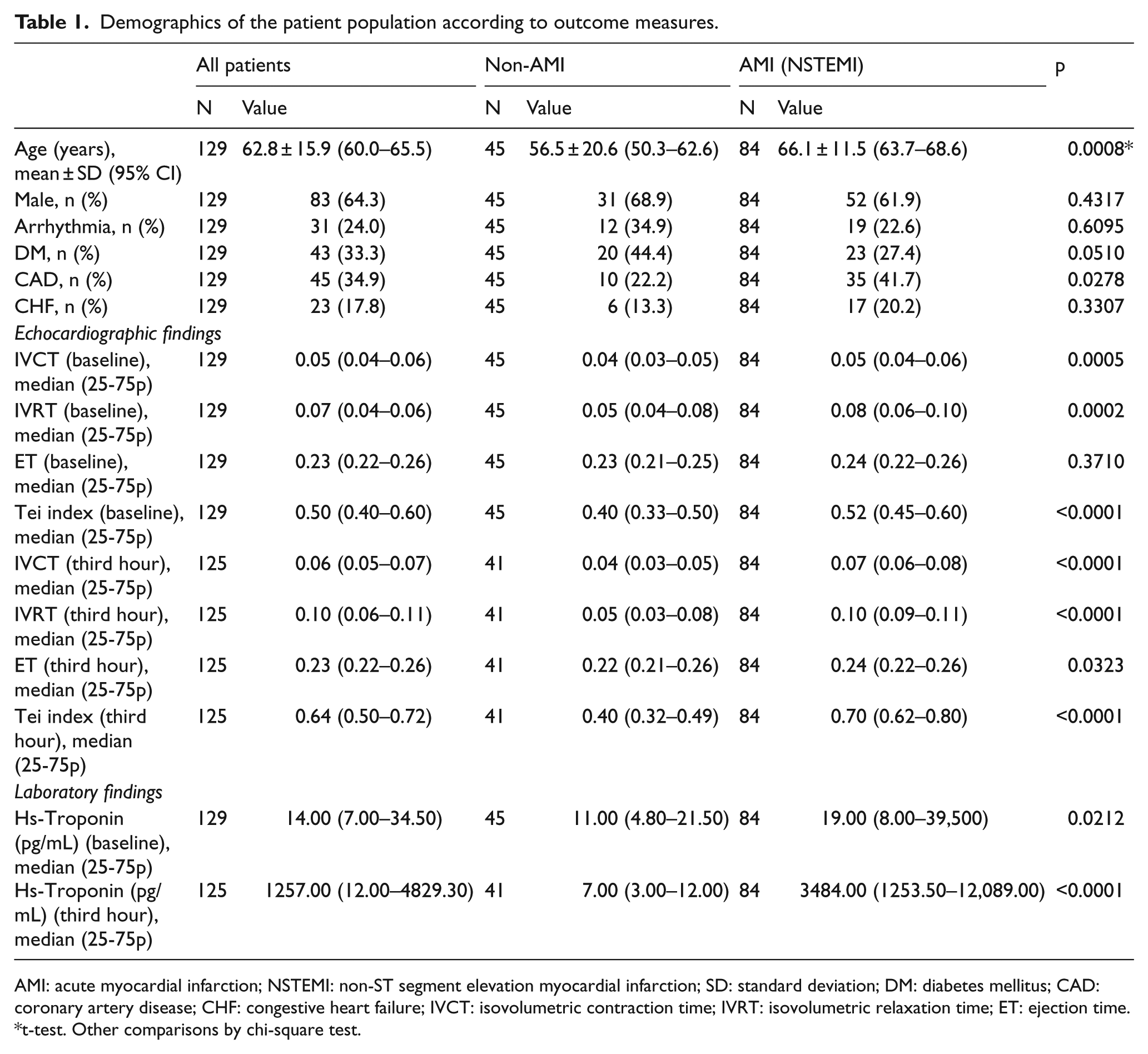
AMI: acute myocardial infarction; NSTEMI: non-ST segment elevation myocardial infarction; SD: standard deviation; DM: diabetes mellitus; CAD: coronary artery disease; CHF: congestive heart failure; IVCT: isovolumetric contraction time; IVRT: isovolumetric relaxation time; ET: ejection time.
t-test. Other comparisons by chi-square test.
Comparison of Hs-Troponin and Tei index values among AMI and non-AMI patients at the baseline, at the third hour, and comparison between the two.
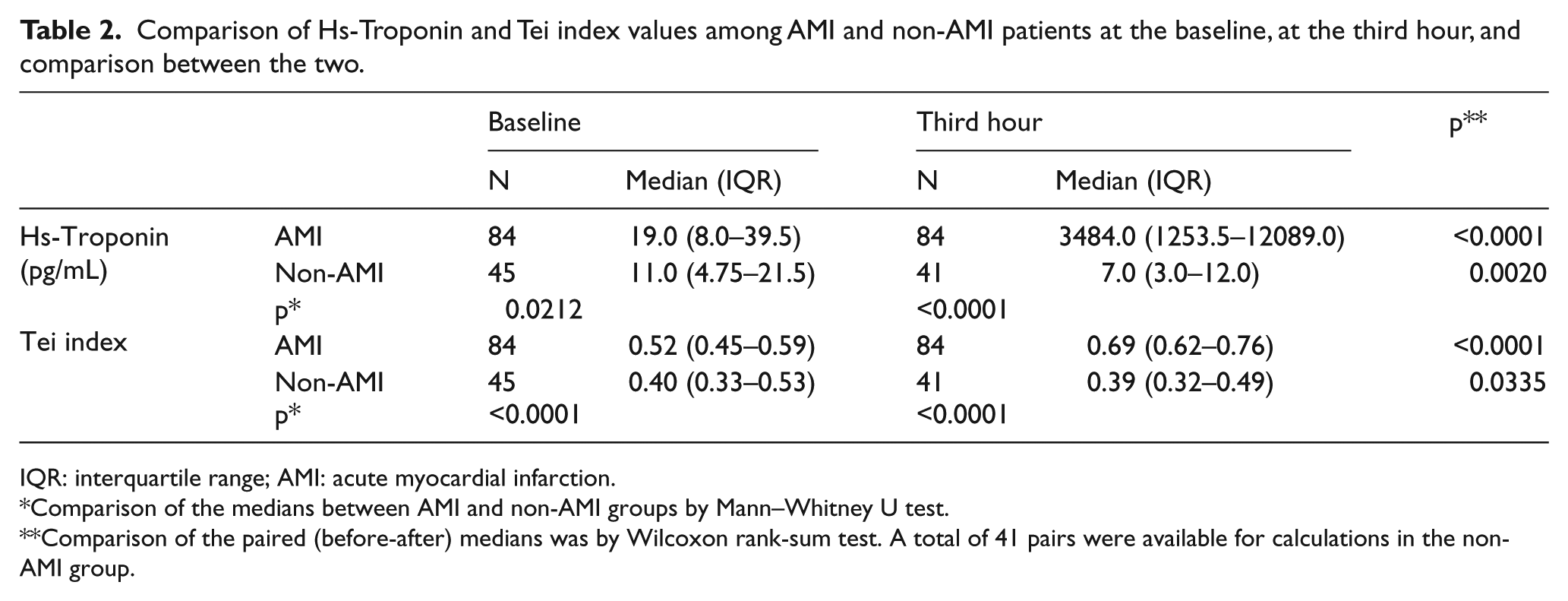
IQR: interquartile range; AMI: acute myocardial infarction.
Comparison of the medians between AMI and non-AMI groups by Mann–Whitney U test.
Comparison of the paired (before-after) medians was by Wilcoxon rank-sum test. A total of 41 pairs were available for calculations in the non-AMI group.
For the primary aim of this study, the Tei index was found to have a high sensitivity (79.8%) but a low specificity (60%) for the diagnosis of NSTEMI. The Tei index and Hs-troponin were positive in 71 (85%) and 37 (44%) of the 84 NSTEMI patients at presentation, respectively. The +LR of the Tei index was higher (1.99 vs 1.70) and −LR was lower than (0.34 vs 0.54) Hs-troponin at presentation. Pairwise comparison of the receiver-operating characteristic (ROC) curves of the Tei index and Hs-troponin at the baseline revealed a statistically insignificant difference in area under the curve (AUC) of 0.11 (n = 129, AUC: 0.73 vs 0.62; 95% CI: −0.03 to 0.25, p = 0.1299, Figure 4(a)). The +LR of the Tei index increased to 5.0 and −LR decreased to 0.03 at the third hour, which revealed a statistically significant increase in the AUC of the Tei index (n = 125, AUCs: 0.75 to 0.94, difference: 0.19, 95% CI: 0.12 to 0.26, p < 0.0001, Figure 4(b)). All diagnostic utility metrics are summarized in Table 3.
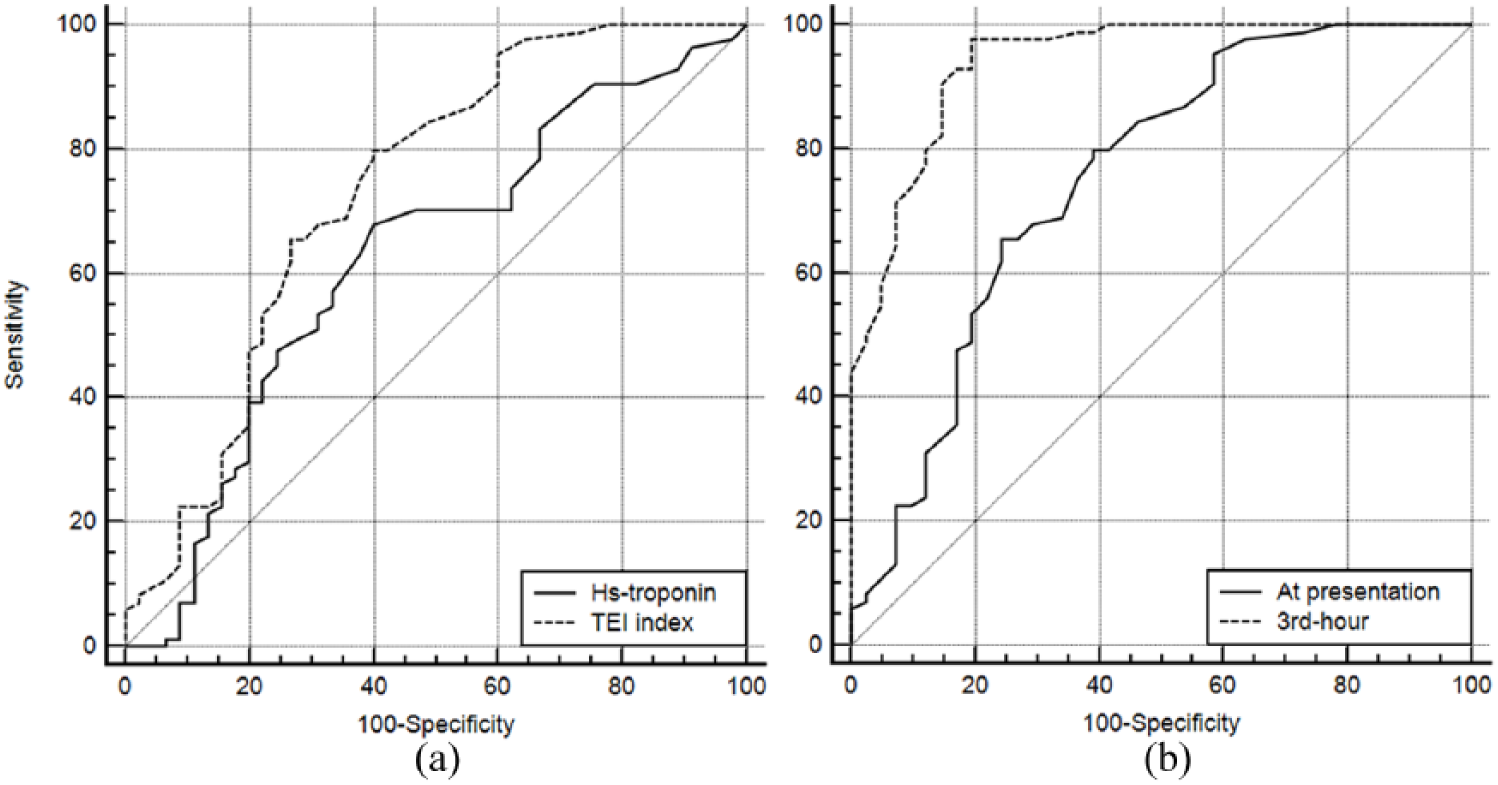
(a) Pairwise comparison of the ROC curves of the Tei index and Hs-troponin for the diagnosis of NSTEMI and (b) pairwise comparison of the ROC curves of Tei index at presentation and at the third hour for the diagnosis of NSTEMI.
Diagnostic utility of the Tei index, Tei change, and initial Hs-Troponin for NSTEMI.
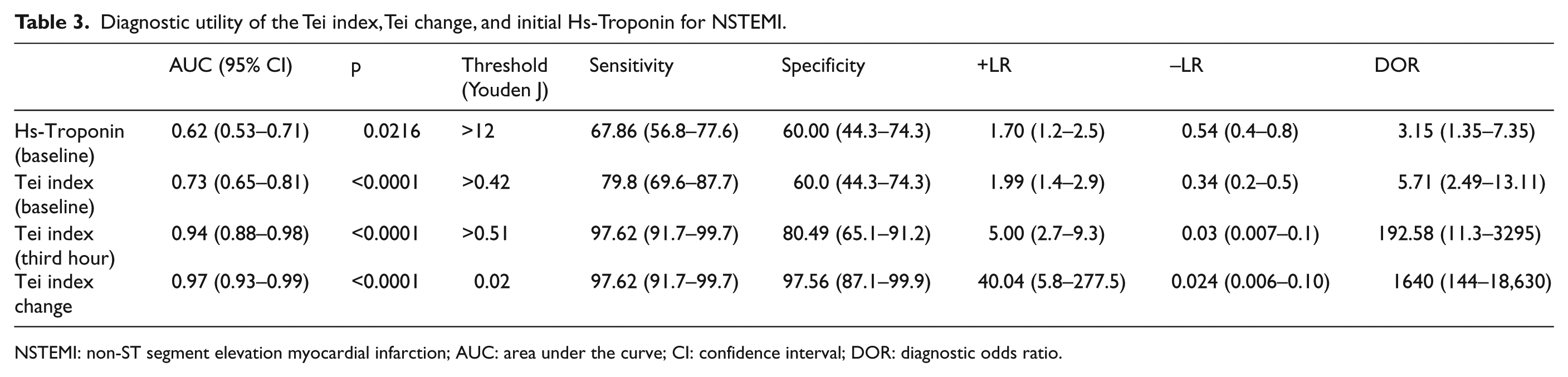
NSTEMI: non-ST segment elevation myocardial infarction; AUC: area under the curve; CI: confidence interval; DOR: diagnostic odds ratio.
The comparison of the change in the mean Tei index values from presentation to the third hour according to the final diagnosis showed that the only statistically significant difference was observed in the NSTEMI group (Table 4). The absolute change in the Tei index values of all patients was plotted according to their final diagnosis in Figure 5, and its diagnostic utility metrics are summarized in Table 3. A 0.02 or more increase in the Tei index value has a 97.6 sensitivity and 97.5 specificity for the diagnosis of NSTEMI.
Tei index values at presentation and third hour according to final diagnoses.
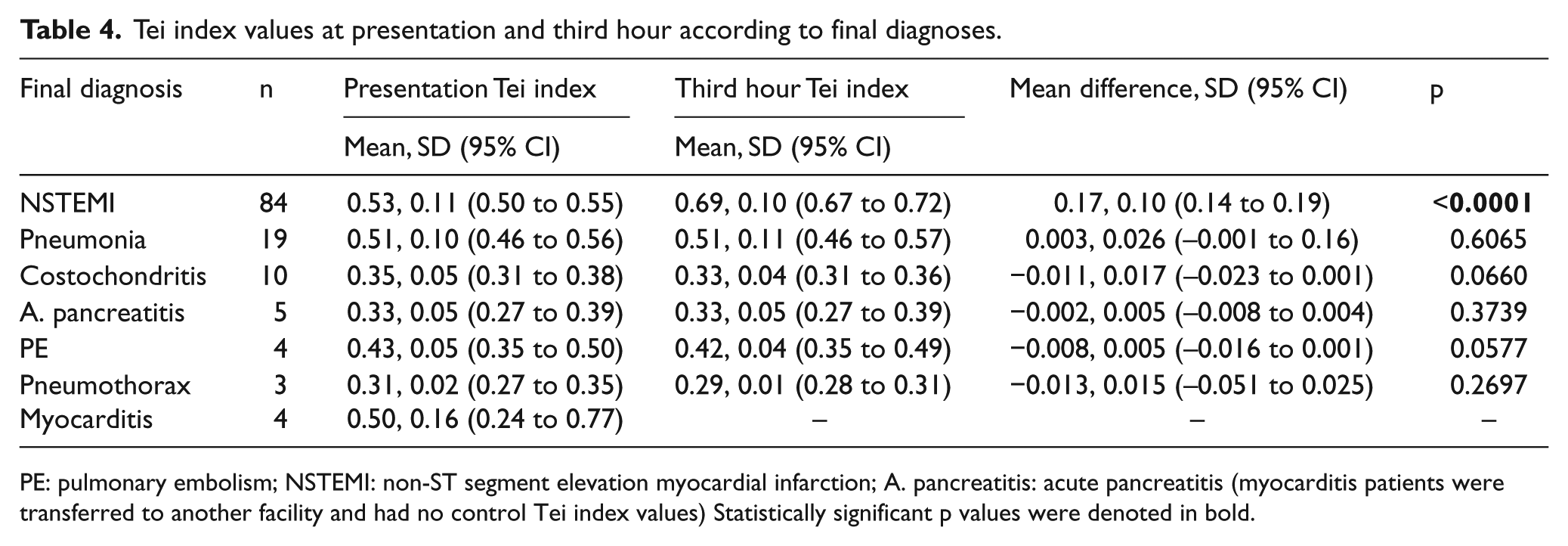
PE: pulmonary embolism; NSTEMI: non-ST segment elevation myocardial infarction; A. pancreatitis: acute pancreatitis (myocarditis patients were transferred to another facility and had no control Tei index values) Statistically significant p values were denoted in bold.
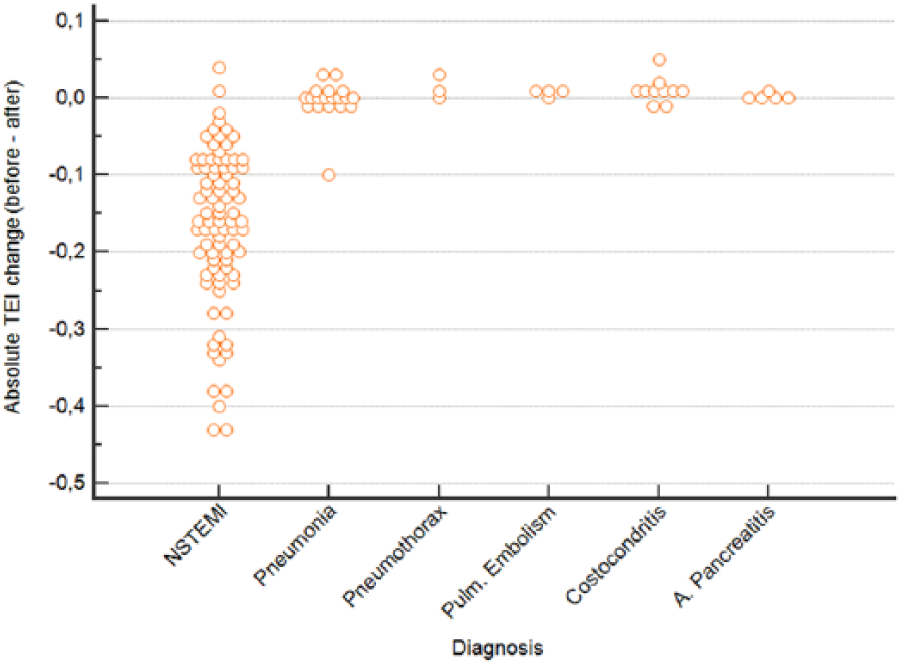
The absolute change in the Tei index values of all patients plotted according to the final diagnosis.
In our study, 55 of 83 (66.3%) patients with a negative Hs-troponin at presentation had a positive Tei index measurement. The diagnostic utility of the Tei index in this subgroup of patients with an initial negative Hs-troponin level (AUC: 0.71, 95% CI: 0.60 to 0.81, p = 0.0004) was similar to the overall study population (AUC: 0.73, Table 3). Therefore, the use of the Tei index in this subgroup of patients has not increased the diagnostic utility of the overall approach compared to the use of Hs-troponin alone (Table 3).
For the secondary aim, we calculated the Spearman’s rank correlation r-value of the Tei index with Hs-Troponin at presentation as 0.18 (95% CI: 0.01 to 0.34, p = 0.0395), which is significant but low. Correlation coefficients were similar for NSTEMI (r = 0.22) and non-AMI patients (r = −0.16).
Sensitivity analysis
To evaluate the effect of the four patients’ lost-to-follow-up, a sensitivity analysis was performed. Even it was assumed that all four patients’ lost-to-follow-up had positive Tei index at presentation and third hour despite not being NSTEMI, the AUC of Tei index changed just slightly without any statistically significant difference (p > 0.05).
Discussion
The diagnostic utility of the Tei index has been studied mainly on patients with accompanying right ventricular dysfunction. Diagnosis of STEMI in the ED is much easier than NSTEMI since it has well-defined ECG criteria and an apparent clinical presentation. However, the diagnosis of NSTEMI usually necessitates follow up with continuous cardiac monitoring and serial Hs-Troponin measurements. In this study, we found that the accuracy of initial Tei index was 0.11 higher (AUC: 0.73 vs 0.62; difference: 0.11, 95% CI: −0.03 to 0.25, p = 0.1299) than Hs-troponin level for the diagnosis of NSTEMI and was within the predetermined non-inferiority limit (0.15) of this study. To the best of our knowledge, this study is the first in the literature to investigate the diagnostic utility of the Tei index in NSTEMI patients, and it is found that it is non-inferior to Hs-troponin.
This study also sets the foundations for future research. A prospective study for superiority should include at least 154 NSTEMI and 288 NSTEMI chest pain patients with an overall sample size of 442 to achieve the power of 80%. We think that the Tei index might be a useful tool to diagnose NSTEMI earlier than the Hs-Troponin. It also has advantages over other modalities, like computed tomography (CT) angiography and scintigraphy, and it is easier to interpret and perform.
In this study, the Tei index change (from the presentation to the third hour) was also found to be a promising diagnostic parameter for NSTEMI, with sensitivity and specificity over 97%, and a diagnostic odds ratio of 1640. Therefore, Tei index change shows significantly higher diagnostic accuracy compared to both initial Tei index and Hs-troponin levels. AMI is an ongoing ischemic event, and there is myocardial necrosis unless reperfusion or damage completed. At the early phase, the systolic/diastolic function may be preserved.17,18 Hence, it is understandable that the diagnostic value of the Tei index is lower initially, similar to Hs-troponin levels.
Tei index might be useful or sensitive to detect heart failure. In the study of Meric et al., 19 Tei index demonstrated an increase following the deterioration in LV function and also it was found to be superior to left ventricular ejection fraction (LVEF) in differentiating patients with and without heart failure. Yuasa et al. investigated the prediction of complications with AMI by LV Tei index in their study. Regional and global LV function improves after successful treatment. The Tei index was found to be an easy, fast, and applicable method, and among the functional indices, the Tei index achieved the best accuracy in the prediction of complications with AMI. 20 While the Tei index may be useful reflecting the severity of global dysfunction in AMI, the diagnostic accuracy for NSTEMI is not established in the literature. Early prediction is clinically important. This might be related to the ability of Tei index detecting the left ventricular dysfunction earlier than the Hs-Troponin in case of AMI. This foresight should be supported with more extensive studies.
Limitations
There were limitations to this study. First, it was conducted in a single center by an individual researcher. Therefore, the study sample was limited to those who presented when the days principal researcher was on duty. Besides, this study was conducted in a center which did not have a cardiovascular unit. Therefore, the diversity of patients in this study may be limited. Since patients were referred to a PTCA capable center after the diagnosis, their outcomes were not known. Second, this study only included patients with an ischemic type of chest pain, while other chest pain patients were excluded. Therefore, the number of patients in the non-AMI group was limited.
Conclusion
Initial Tei index is non-inferior to initial Hs-troponin level for the diagnosis of NSTEMI. The Tei index change (from the presentation to the third hour) is a promising diagnostic parameter for NSTEMI, with sensitivity and specificity over 97%. Further research is needed to investigate both parameters for superiority.
Footnotes
Acknowledgements
We thank Haldun Akoglu, Associate Professor of Emergency Medicine, MD, for assistance with statistical analysis and for the comments that greatly improved the manuscript. Initials of the contributing authors were listed in brackets after the relevant parts of the research: literature search (A.B.U., E.U.A., R.A., Y.E., H.D., T.C.O.), study design (A.B.U., E.U.A., H.D., T.C.O., Z.D.I., O.O.), legislative applications (E.U.A., T.C.O., H.D., O.O., R.A., Y.E.), data collection (A.B.U., E.U.A., Y.E., R.A.), supervision and quality control (E.U.A., T.C.O., H.D., Z.D.I., O.O.), statistical advice (E.U.A., T.C.O., O.O.), statistical data analysis (E.U.A., H.A.), data interpretation (A.B.U., E.U.A., T.C.O.), and drafting the manuscript (A.B.U., E.U.A., T.C.O.). All authors were involved in the writing and critical revision of the manuscript and approved the final version. A.B.U., E.U.A., and T.C.O. take responsibility for the paper as a whole. This manuscript was presented as an oral presentation at the 5th Eurasian Congress on Emergency Medicine at Antalya, Turkey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
We agree to the conditions of publication including the availability of data and materials in our manuscript.
Informed consent
Informed consent was obtained from the participants or their legally authorized representatives.
Ethical approval
This study was approved by the local ethics committee.
Human rights
The principles outlined in the Declaration of Helsinki have been followed.