
Abstract
Background:
The anxiety and stress level of both parent and child seeking treatment at the emergency department is assumed to be high. However, it is rarely quantified as to ascertain any need for intervention.
Objective:
The study seeks to quantify anxiety of parents accompanying sick children presenting acutely to the emergency department and to explore possible pre-visit factors that may contribute to anxiety.
Methods:
A 12-month cross-sectional study was conducted at the Emergency Department, Universiti Kebangsaan Malaysia Medical Centre. All parents accompanying a child presenting to the study location, fitting the inclusion and exclusion criteria, were invited to participate. Parents required to fill a self-administered questionnaire on anxiety, State-Trait Anxiety Inventory and any related factors that can influence anxiety.
Results:
A total of 233 subjects were recruited. The mean state anxiety score was 53.48 ± 11.36, compared to the mean score for trait anxiety of 39.85 ± 7.66, suggesting a heightened state of anxiety. Majority of subjects (65.7%) had reported clinically detected anxiety as defined by state anxiety score above 49. There was no significant association between parental anxiety level with pre-visit factors: children’s age, duration of illness, the presence of co-morbidities, time of presentation, prior medical contact and primary care referral. The child’s state of illness was the dominant psychosocial factor associated with parental anxiety reported by the subjects.
Conclusion:
Parental anxiety upon arrival appeared to be significantly higher than expected, suggesting intervention may be needed.
Introduction
Stressful hospital experiences such as emergency department (ED) visit and hospitalisation are linked to child adjustment problems, for example, anger, aggression, panic, anxiety, fear of health personnel and separation anxiety from family. 1 The situation could bring a huge unpredictable impact on the child as well as the entire family. It potentially disrupts the normal flow of family life as parents are frequently exposed to multiple negative emotions.2–4
Parents with negative emotions and behaviours are often exposed to uncertainty, disorganisation, vulnerability, anxiety, depression, anger, helplessness, inadequacy and guilt. 3 Shudy et al. 5 investigated the impact of children’s illness on families, whereby they noted that admission of a critically ill child is a source of distress. Apart from that, the parents find themselves in an unfamiliar environment and their parental role could change.
The concept of child-friendly ED was introduced to eliminate anxiety among children and accompanying parents while seeking treatment in ED. However, the currently available strategies are narrowed on the build-environment or highly specific clinical intervention plans, such as wait time, service provision and delivery of information.6,7 The missing component in these strategies is the modification of the pre-visit anxiety levels and parents’ expectation of the intended ED visit, which is identified as a previously unknown untapped key research area in current research regarding this theme.
This cross-sectional study attempted to quantify the level of anxiety perceived and explored the concept of pre-visit anxiety when seeking treatment at the ED, from the perspective of the accompanying parent. The context of an acute unplanned situation is arguably different from existing work that concentrated on elective situations such as preparation for elective hospitalisation of a child.
Methods
This is a cross-sectional study conducted at the Department of Emergency Medicine, Universiti Kebangsaan Malaysia Medical Centre (UKMMC), which is a tertiary academic medical institution with an average of 72,000 presentations per year. The study was conducted from April 2015 until May 2016 and received an approval from UKMMC Medical Research Ethics Committee (FF-2015-274).
Participants
The subjects were all parents aged 18 and above with patients aged 12 years old and below presented to the ED for a perceived need for acute medical care. Parents with the following child were excluded: (1) critically ill children, (2) a child who was brought death and (3) a child who was abused. The exclusion criteria took into account in situations where the expected anxiety was predicted to be quiet extreme as to cause impairment in judgement. Parents who could not understand or communicate in Malay or English were also excluded.
Measurement tool
The Spielberger State-Trait Anxiety Inventory (STAI) form Y was used to measure parental anxiety. The STAI is a 40-item, self-administered measurement tool consisting of two subscales: state and trait subscales. 8 The state anxiety subscale measures individual’s current state of anxiety that refers to transitory unpleasant feelings of apprehension, tension, nervousness or worry, while trait anxiety subscale measures how prone the individual is to experience anxiety. Each subscale consists of 20 items and rated based on 4-point Likert-type scale. The scores range from 20 to 80, with the higher scores indicating greater anxiety. An optimal cut-off point in clinical setting studies of STAI is 40.9–11 Previous generalisation reliability of STAI demonstrated high internal consistency (Cronbach’s alpha, α > 0.89). 12 A validation study of English STAI among Malaysian subjects showed high internal and test–retest reliability.13,14 For the purpose of the study, we conducted a validation study of Malay-translated STAI and the results were favourable.
Study protocol
All parents accompanying a child presenting to the study location during the study period, fitting the inclusion and exclusion criteria, were invited to participate. The study measured state and trait anxiety of parents as they presented to the ED, requiring each subject to fill the self-administered questionnaire on anxiety (STAI). Recruitments began upon completion of necessary clinical procedures during the early assessment, such as phlebotomy and oxygenation. Parents who agreed to participate and answered the questionnaires were required to give a written consent. Either English or Malay-translated STAI was given as subject’s preference. The questionnaire included six pre-visit factors to potentially associate with parental anxiety: children’s age, duration of illness, the presence of co-morbidities, time of presentation, prior medical contact and primary care referral.
The sample size was calculated based on the estimate that half of the paediatric presentation (accounting for 20% of total presentations to the ED) has a significant level of anxiety. The data obtained were evaluated with IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 233 parents were enrolled. Table 1 shows the demographic characteristics of the subjects. The mean age of subjects was 33.5 ± 6.5 years, with a child’s age ranging from few days to 11 years. The majority, 55.8%, were recruited in the semi-critical area. The subjects were dominantly young Malay mother, educated and employed. Table 2 shows characteristics of the patients. Majority of the patients presented with a respiratory-related illness, followed by gastrointestinal and undifferentiated fever. The median duration of illness was 3 days. In total, 103 (44.2%) patients were hospitalised.
Demographic characteristics of the parents (N = 233).
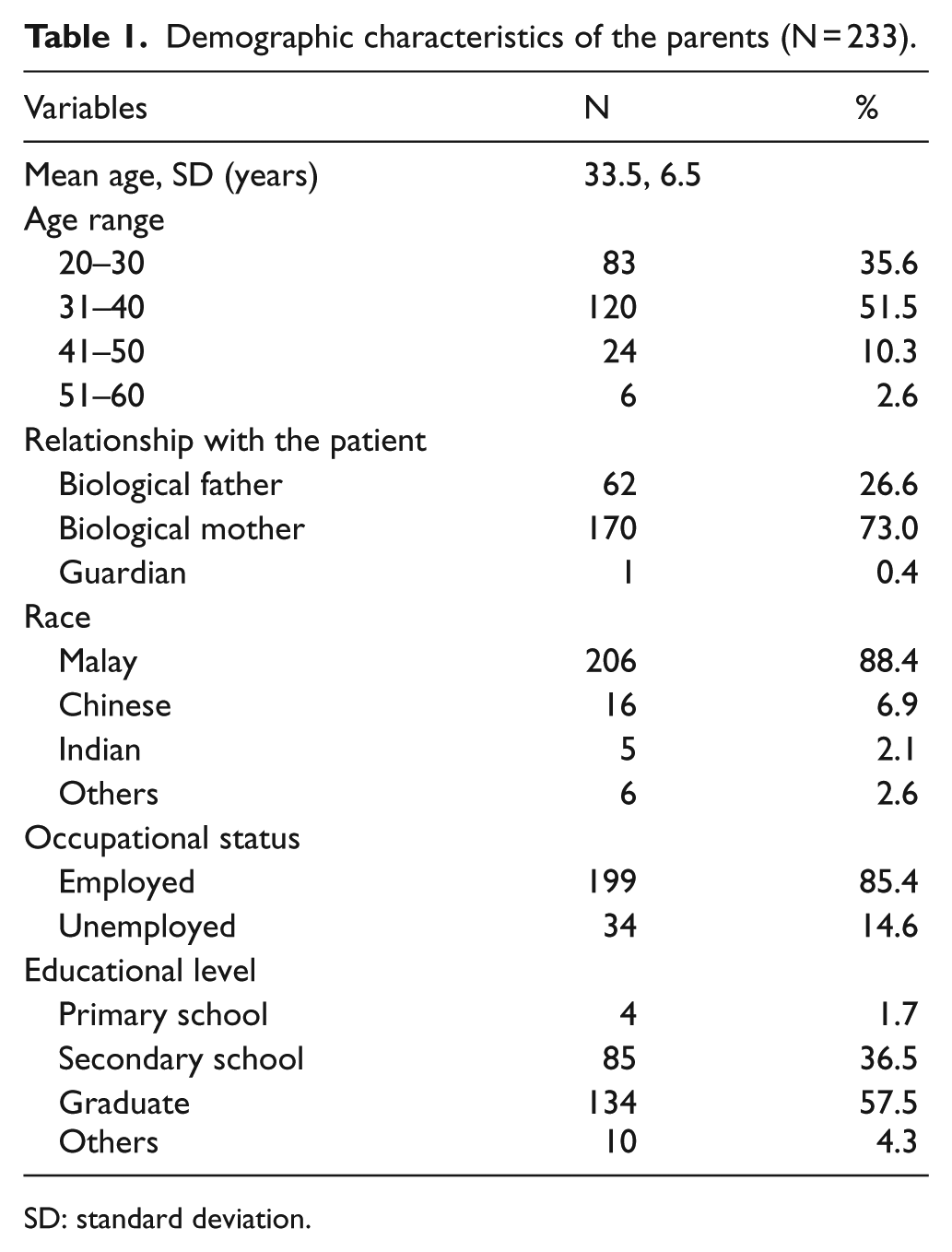
SD: standard deviation.
Demographic characteristics of the children (N = 233).
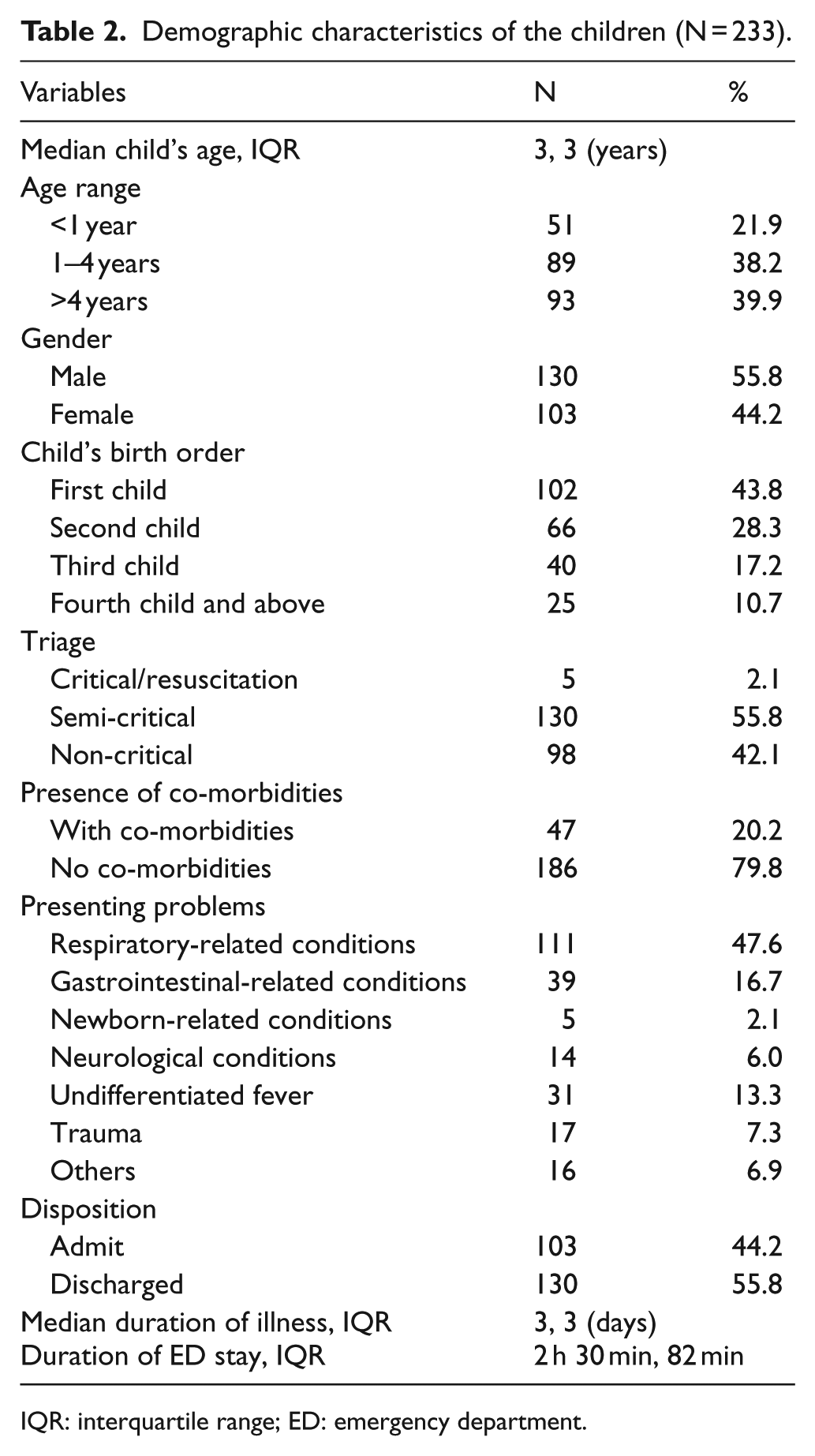
IQR: interquartile range; ED: emergency department.
For reference, a cut-off value of above 49 for state anxiety score is considered clinically significant. The more divergent between the state and trait score suggests anxiety is heightened. The mean state anxiety score for all parents was high, 53.45 ± 11.36, 34% increment from their baseline (trait anxiety score) of 39.85 ± 7.66. A total of 153 parents (65.7%) had reported clinically detected anxiety. There is a considerable gap in scores between the bottom 25% of the sample population with 45.00 and the score of 62.00 for 75th percentile.
The results of pre-visit factors are shown in Table 3. None of the factors demonstrated a significant association with parental anxiety level. Out of 233 parents, 212 stated the psychosocial factors associated with anxiety level. A total of 11 themes were identified, with majority stating that the child’s state of illness was the cause of anxiety in ED (Figure 1).
Association of pre-visit factors with the anxiety scores.
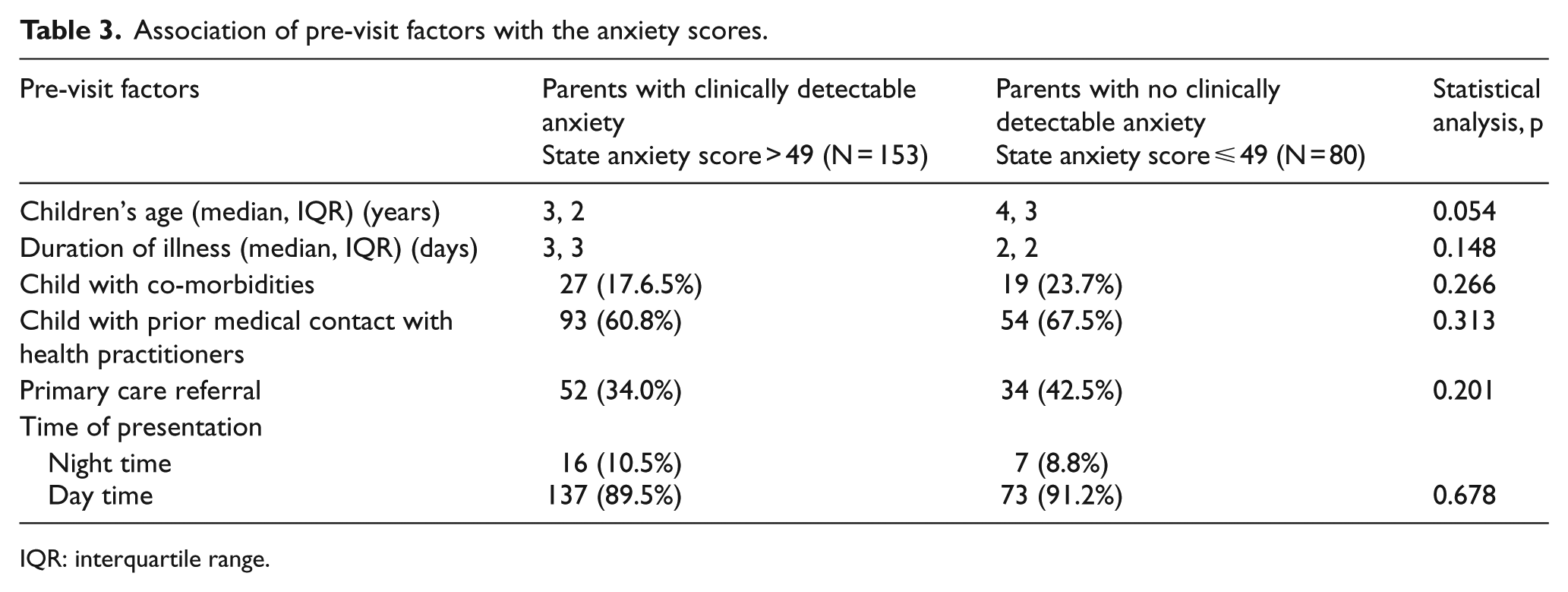
IQR: interquartile range.
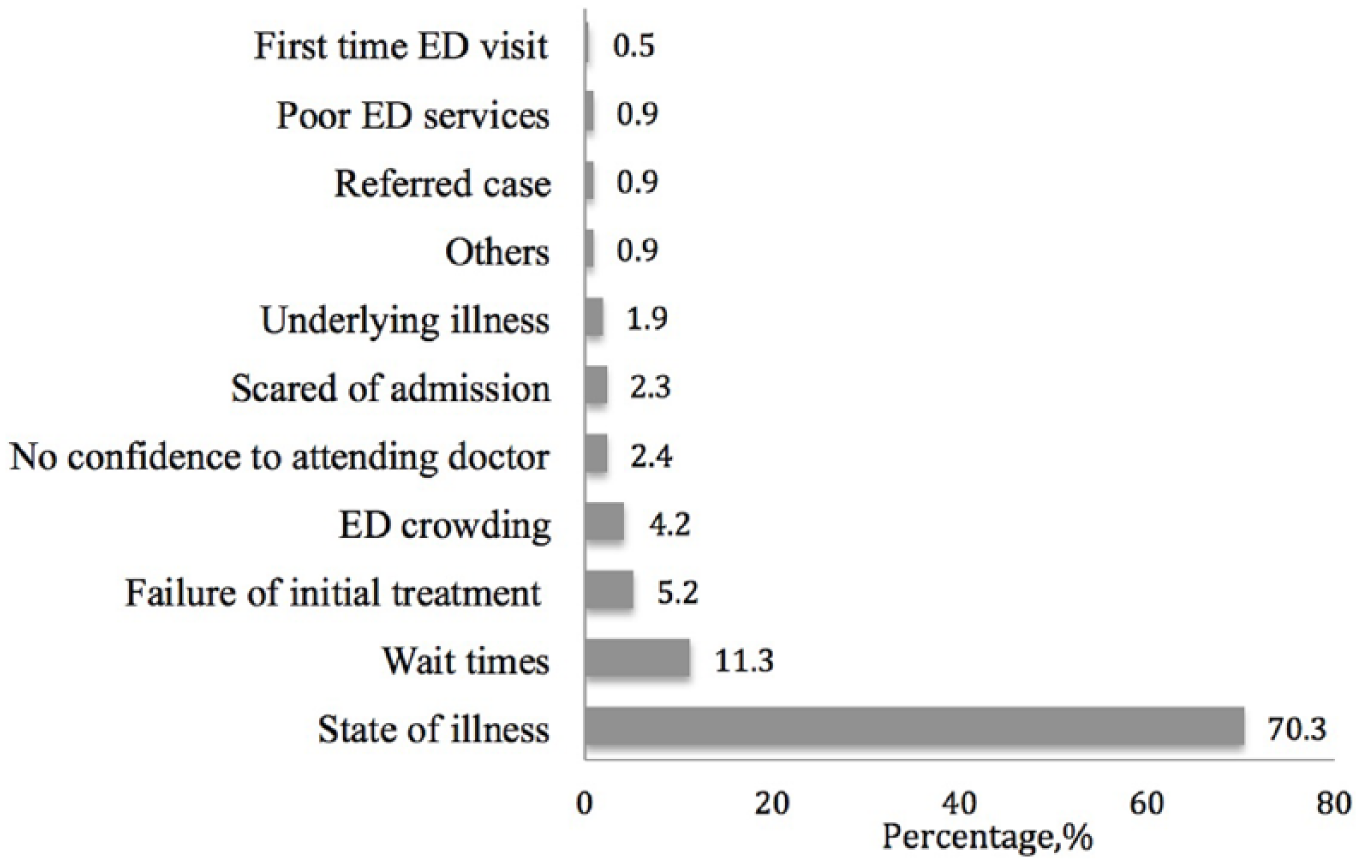
Distribution of psychosocial factors contributed to the parental anxiety.
Discussion
The results of this study indicate that parents of a child presented acutely to the ED had a substantial degree of anxiety. This is consistent with other studies performed in ED setting but on specific groups. Save-Pédebos et al. 15 reported higher mean state anxiety score among parents with a child who had the first episode of seizure, 58.7; while parents with febrile children had lower state anxiety score, 50.1. 16 This is in contrast with reported levels of anxiety in non-acute setting.17–20 These include parents of a child who underwent elective surgery17,18 and parents of a child seen in the cardiology clinic for heart murmurs. 19
As expected, the cross-section of the study population has a high proportion of parents with clinically detectable anxiety. This is higher when compared to a sample of adult patients presented to ED with pain-related complaints, in which 48% of patients described moderate to severe anxiety. 21 In a sample of Norwegian parents of children referred for a heart murmur, 58% of them were classified into anxiety group. 19
Our study demonstrated that none of the pre-visit factors had a significant association with parental anxiety. While investigating the effect of children’s age on parental anxiety, Litman et al. 17 demonstrated greater anxiety among parents with a child aged less than 1 year who underwent elective surgery. However, studies performed among parents of a child in an acute care setting including intensive care unit (ICU) and ED have demonstrated no significant association.4,16,17,22–25 It can be argued therefore in the unplanned emergency setting that the influence of the child’s age on parental anxiety is minimal. The nature of the medical condition affecting the child is also likely to have minimal effect.16,26 The timing of presentation may be associated with higher anxiety, 16 but this has not been demonstrated in this study. Late night presentations may be instead a manifestation of increased anxiety, rather than influencing it. The literature so far also do not support the duration of illness or previous contact with healthcare services as influencing factors.16,19
The study also explored other possible psychosocial factors influencing parental anxiety from the parents’ perspective. The results revealed that majority of parents reported their anxiety levels were highly influenced by children’s condition, which included their state of illness, poor response to initial treatment and underlying illness. This is consistent with the literature suggesting the worry of the child’s state of illness was the most influential factor related to parental anxiety in ED. 27 High degree of uncertainty during ED visit, as well as concern relating to possible pain from clinical procedures, may contribute more to their anxiety level. Prolonged waiting times and unsatisfactory waiting room conditions have been shown to lead to restlessness, frustration and boredom, but not necessarily anxiety. 28
A key strength of this study was the successful estimation of parental anxiety at the initial presentation to ED, which was not reported in the literature to date. Similar studies revolving around hospitalised children measured anxiety during less acute phases of care where the child had already received an initial treatment – this can affect the quantum of anxiety score measured. There were several limitations of this study. Our sample comprised all parents of a child admitted to ED regardless of triage and severity. As the majority of our subjects were recruited in the semi-critical area, the accuracy of the mean state anxiety score to reflect all presentations can be argued. The 40-item questionnaire may be cumbersome to fill while attending to a sick child. Future study needs to focus on group-specific parents in ED and apply the short version of STAI to measure anxiety.
Acute hospitalisation of a child can negatively affect child outcomes. A recent meta-analysis revealed only a small number of studies investigating the effect of various coping support intervention to parents in the situation of acute hospitalisation, with mixed success in reducing anxiety. 29 Future study is necessary to observe trends of anxiety throughout patients’ stay in ED. As a conclusion, acute unplanned child admission to ED is a taxing event for parents and associated with a substantial level of anxiety and should not be ignored. A structured intervention focused on parental anxiety reduction can lead to overall positive experience of ED stay.
Footnotes
Acknowledgements
Licensing for use of STAI in this study was obtained from Mind Garden, Inc.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a grant from the National University of Malaysia (UKM) (Institution Young Reseacher’s Incentive Grant; GGPM-2014-061).
Availability of data and materials
The master spreadsheet in SPSS sav format has been uploaded (raw data.sav).
Ethical approval
The study received an approval from the UKMMC Medical Research Ethics Committee (FF-2015-274).
Informed consent
All subjects were required to give a written consent as stated in manuscript.