
Abstract
Objective:
This study aimed to verify the effect of introducing a feedback device during adult and infant cardiopulmonary resuscitation training.
Methods:
A feedback device was introduced in the cardiopulmonary resuscitation training course of our medical school in the middle of the last semester. The cardiopulmonary resuscitation training course consisted of 2 h of instructor-led cardiopulmonary resuscitation training and 1 h of self-practice time. All students should complete the adult and infant cardiopulmonary resuscitation skill tests just after the course. Each test consisted of five cycles of single-rescuer cardiopulmonary resuscitation. A feedback device was introduced only in the self-practice session. The cardiopulmonary resuscitation parameters of the skill tests before (n = 40) and after (n = 39) introducing the feedback device were analysed.
Results:
The ratios of correct rate significantly increased after introducing the feedback device in both the skill tests (adult test: 58.5 ± 37.2 vs 85.5 ± 21.4, p = 0.001; infant test: 55.0 ± 32.4 vs 80.2 ± 20.7, p = 0.001). Although the average depths did not significantly differ between those before and after introducing the feedback device in the adult test (58.4 ± 4.0 mm vs 59.0 ± 3.7 mm, p = 0.341), it increased significantly after introducing the feedback device in the infant test (38.3 ± 4.3 mm vs 40.8 ± 1.1 mm, p = 0.001).
Conclusion:
Introducing a feedback device might have enhanced the accuracies of compression rate in adult and infant cardiopulmonary resuscitation training. However, the potential positive effect on chest compression depth was limited to infant cardiopulmonary resuscitation training.
Introduction
The recent cardiopulmonary resuscitation (CPR) guideline recommends the use of CPR feedback devices during training because an inadequate performance of CPR is common. 1
The CPR feedback devices are divided into two different things according to their feedback methods. 1 First, the CPR feedback devices that provide corrective feedback to the trainees. Second, CPR prompt devices that provide only a tone or audible sound to the trainees without corrective feedbacks. The former could improve the quality of chest compressions. Although the latter could improve the accuracy of chest compression rate, one report showed a negative effect such as decreasing chest compression depth. 2
A real-time visual feedback is one of the CPR feedback methods. Using a real-time visual feedback device could improve the quality of CPR, especially chest compression depth. 3 , 4 Our medical school introduced a real-time visual feedback device in the last year to improve the students’ CPR skills. This study was conducted to verify the effects of introducing a real-time visual feedback device during adult and infant CPR training.
Methods
This study retrospectively analysed the CPR parameters of the adult and infant CPR skill tests before and after introducing a feedback device in the CPR training course of our medical school. The study was approved by the institutional review board of our hospital (Approval No. 1802-002-16141).
Our medical school provides a CPR training course to third- and fourth-year students. The CPR training course comprises 2 h of instructor-led CPR training and 1 h of CPR practice by the student themselves (self-practice session). The contents of the course include an adult CPR technique with the standard two-hand chest compression and mouth-to-mouth ventilation and an infant CPR technique with the two-thumb encircling hand technique or two-finger technique and mouth-to-mouth and nose technique. Resusci Anne QCPR (Laerdal Medical, Stavanger, Norway) is used as the adult manikin, and Resusci Baby QCPR (Laerdal Medical) is used as the infant manikin. The instructor-to-student ratio is 1:2 or 1:3. The instructor emphasizes several CPR conditions to the students, such as pushing hard (at least 5 cm in adults and approximately 4 cm in infants), accurate position (lower half of the sternum), pushing fast (100–120/min), complete chest wall recoil, avoiding hyperventilation and minimizing hands-off time. All students should complete the single-rescuer adult and infant CPR skill tests by using the two-hand and two-finger techniques just after the course. Each test comprises five cycles of CPR with a 30:2 compression-to-ventilation ratio. The ventilations are performed using a face shield. The CPR skill test score (range: 0–100) and CPR parameters are collected during the skill tests. The test scores are calculated automatically using the SkillReporter software. The parameters include total chest compressions (n), ratio of correct hand position (%), average rate (/min), ratio of correct rate (%), average depth (mm), ratio of correct depth (%), ratio of complete recoil (%), total ventilations (n), average volume (mL) and chest compression fraction (%).
The CPR training courses took place every week from June 2017 to February 2018 in the emergency department. Two or three medical students took part in the CPR training course at one time. To follow the recommendations of the recent CPR guideline, a visual feedback device, SimPad PLUS with SkillReporter (Laerdal Medical), was introduced in the self-practice session of the CPR training course in the middle of the last semester (October 2017). Before October 2017, the students practised CPR only with manikin during the self-practice session (non-feedback group). After October 2017, the students practised CPR according to the visual feedback signals from the SimPad PLUS with SkillReporter during the self-practice session (feedback group). The feedback device was not provided during the CPR skill tests.
The CPR parameters of the two groups (non-feedback group vs feedback group) were analysed. All statistical analyses were performed using IBM SPSS v.20.0 (IBM, Armonk, New York, NY, USA). The data are presented as mean ± standard deviation. Data were analysed using the Shapiro-Wilk test to verify the normality of distribution. For normally distributed data, the Student’s t test was performed to compare outcome variables between the two groups. Otherwise, the Mann–Whitney U test was used to compare variables between the two groups. A p value of <0.05 was considered to indicate the statistical significance.
Results
In all, 40 students completed the course without using a feedback device (non-feedback group) and 39 students completed the course with the use of a feedback device (feedback group). The test score in infant CPR increased significantly after introducing a feedback device (from 81.7 ± 16.6 to 89.4 ± 12.0, p = 0.017, Table 1). However, no significant difference was observed in the test score in adult CPR (Table 1). For the CPR parameters, average rate and ratio of correct rate were significantly different between the two groups in both the tests (Tables 2 and 3). Especially the ratios of correct rate increased significantly after introducing a feedback device in both the tests (adult test: 58.5 ± 37.2 vs 85.5 ± 21.4, p = 0.001; infant test: 55.0 ± 32.4 vs 80.2 ± 20.7, p = 0.001). By contrast, the average depth and ratio of correct depth increased significantly only in the infant CPR test (average depth: 38.3 ± 4.3 mm vs 40.8 ± 1.1 mm, p = 0.001; ratio of correct depth: 58.4 ± 38.4 vs 85.1 ± 22.2, p < 0.001; Table 3). The other parameters did not significantly differ between the two groups.
Comparisons of cardiopulmonary resuscitation test scores.

CPR: cardiopulmonary resuscitation.
Statistical analyses were performed with Mann–Whitney U tests.
Comparisons of cardiopulmonary resuscitation (CPR) parameters of the adult CPR skill test.
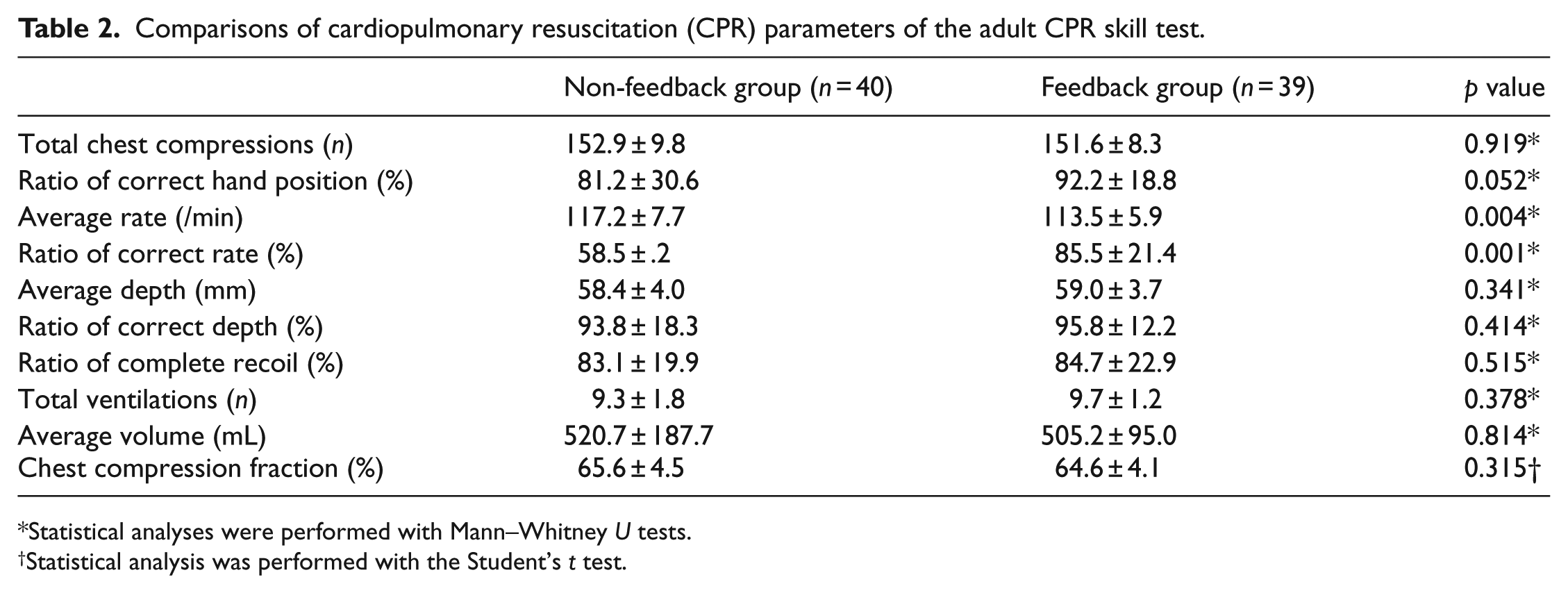
Statistical analyses were performed with Mann–Whitney U tests.
Statistical analysis was performed with the Student’s t test.
Comparisons of cardiopulmonary resuscitation (CPR) parameters of the infant CPR skill test with the two-finger technique.
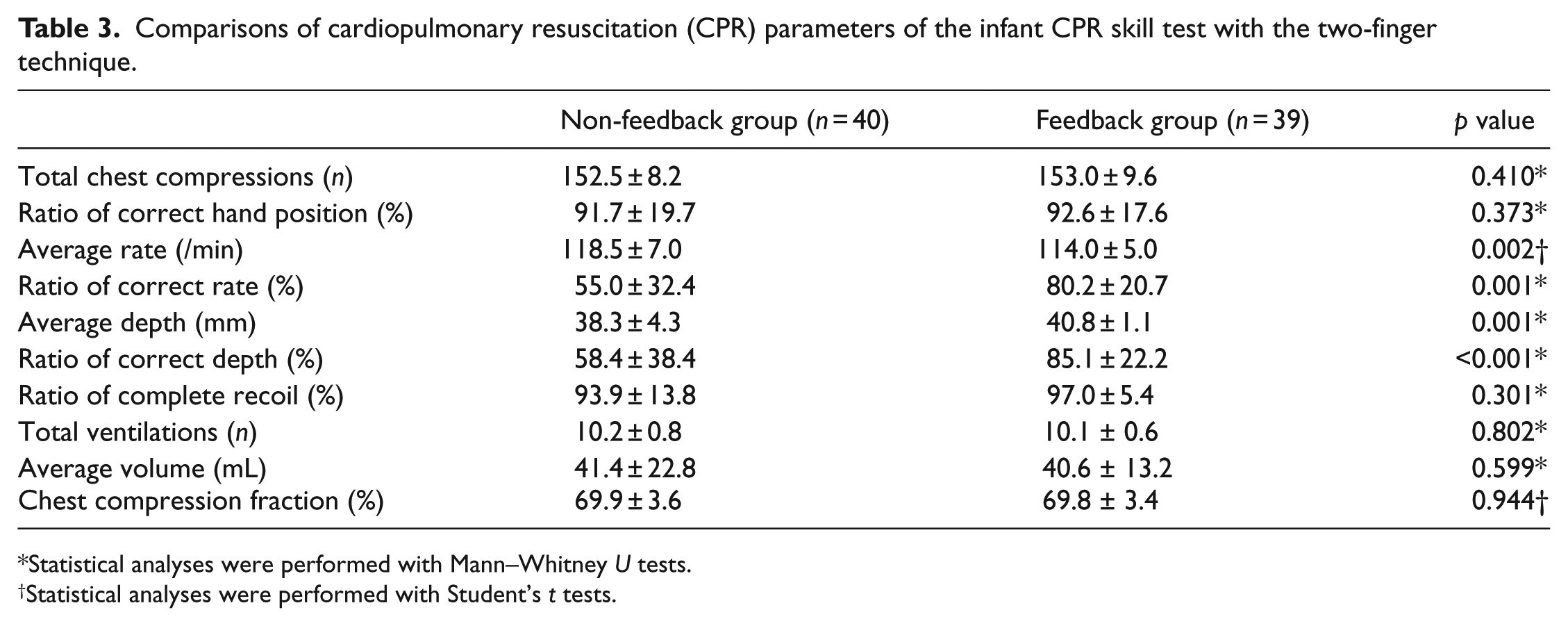
Statistical analyses were performed with Mann–Whitney U tests.
Statistical analyses were performed with Student’s t tests.
Discussion
In a previous study, the chest compression depth of the feedback group was deeper than that of the non-feedback group. 3 No effects were observed on the chest compression rate.
In this study, the accuracy of the chest compression rate was improved after introducing a feedback device. However, no effect was observed on the chest compression depth. These opposite results might be caused by the differences in the feedback mechanism or differences of chest compression target (e.g. at least 5 cm in this study vs approximately 4–5 cm in the previous study). 3 The ability of the previous feedback system was limited by providing visual feedback on chest compression depth, hand position and ventilation volume. 3 By contrast, the enhanced feedback system, the SimPad PLUS with SkillReporter, provides various feedbacks such as adequacies of chest compression depth, chest wall recoil, chest compression rate, hand position and ventilation volume. Therefore, the accuracy of the chest compression rate could be increased. Then why would the chest compression depth not be influenced?
The target of chest compression depth increased from approximately 4–5 cm to at least 5 cm since the 2010 CPR guidelines. 5 , 6 The difference between the words at least and approximately might have caused the different effects from using a feedback device. The word approximately might limit the chance of achieving adequate chest compression depth without a feedback device. Our students tried to push hard as much as possible because they should reach at least 5 cm, regardless of a feedback device. Therefore, the positive effect of the feedback device on chest compression depth might be minimized in our students.
In contrast to the adult CPR training, little evidence was found on the effect of the feedback device on infant CPR training. Recently, Austin et al. 7 evaluated the effects of a metronome and visual feedback device on infant CPR. In their study, the metronome had a maximum positive effect on chest compression rate and visual feedback had a maximum positive effect on chest compression depth. However, they examined the effects of feedback during the CPR practice. They did not examine the effects of CPR training with a feedback device.
Our results indicate that using visual feedback during infant CPR training could enhance the accuracies of chest compression depth and rate simultaneously. For adult CPR training, we emphasized pushing hard and at least 5 cm. However, in the case of infant CPR training, we teach students to push the chest wall approximately 4 cm according to the recent guideline. 8 Therefore, the positive effect of the feedback device on chest compression depth might be maximized in the infant CPR training. As a result, the positive effects of using visual feedback during CPR training seem to be higher in the infant CPR training than in the adult CPR training.
This study has some limitations. First, the data were analysed retrospectively and collected before and after the study design. Although we repeated the CPR training course once in a week independently, the arranging sequence of the student might affect the quality of the skill test because the students could communicate with each other outside the training session. Therefore, bias was highly possible. A prospective well-designed study will be needed to confirm the exact effects of feedback during CPR training. Second, the study was approved by the institutional review board on the condition that we should not deal with personal information. We could assess only the results of the CPR skill tests.
Conclusion
Introducing a feedback device during CPR training might have enhanced the accuracy of the chest compression rate in both adult and infant CPR training. However, the potential positive effect on chest compression depth was limited to infant CPR training.
Footnotes
Acknowledgements
The conception and design of the study: J.H.Oh; acquisition of data: J.H.Oh; analysis and interpretation of data: K.H.K., C.W.K. and J.H.Oh; drafting the article or revising it critically for important intellectual content: K.H.K. and J.H.Oh. Final approval of the version to be submitted: K.H. K., C.W.K. and J.H.Oh.
Availability of data and materials
The study data are available on request to the corresponding author (
Informed consent and Ethical approval
The study was approved by the Institutional Review Board (IRB) of Chung-Ang University Hospital in February 2018 (Approval No. 1802-002-16141). The informed consent was waived by the IRB because the present study analysed the results of skill tests retrospectively. The present study did not include the patients.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.