
Abstract
Background:
Many feedback devices have been designed to improve the resuscitation outcomes. None have been implemented as a standard in patient care.
Objectives:
The aim of this study was to evaluate the chest compression depth and rate during cardiopulmonary resuscitation with and without a feedback device and to evaluate differences regarding the impact of a feedback device based on provider experience.
Methods:
The study was performed on 20 men divided into two groups: group A (n = 10)—paramedics; group B (n = 10)—non-paramedics, trained to provide resuscitation. Participants were examined during resuscitation with Ambu Megacode manikin and with or without the feedback device—CPRmeter. Depth of compressions was evaluated in the first and fourth minute of resuscitation with a BTS Smart DX7000 motion capture system. For statistical analysis, summary statistics, Shapiro–Wilk Test of normality, dependent samples t-test, Levene test, t-test for independent samples, or Welch’s t-test were used. Accepted level of significance was α = 0.05.
Results:
Statistically significant greater depth of chest compressions in group A was observed in the first minute of resuscitation with the device versus the first minute without the device. Significant differences in compressions rate between attempts with and without the device were observed in both groups in the first and fourth minute.
Conclusion:
Only the group of paramedics showed in time some benefits of the device related to the depth, whereas for the group of non-paramedics, the device seemed to have even a deleterious effect. The group of paramedics met the 2015 recommendations related to compressions rate all the time, while the non-paramedics only in the fourth minute of the procedure.
Introduction
Basic life support (BLS) has changed over the last 15 years. Appropriate BLS increases the probability of survival twofold to threefold. 1 Chest compression during cardiopulmonary resuscitation (CPR) is the dominant mechanism to generate forward blood flow important for good neurological outcomes in cardiac arrest victims. 2
The American Heart Association (AHA) and European Resuscitation Council (ERC) 2015 guidelines emphasize the following: provide chest compressions at an adequate rate and depth—which means 100–120 compressions/min at a depth of 5–6 cm, avoid excessive ventilation, and allow complete chest recoil after each compression.3,4
A number of audiovisual feedback devices have been designed to improve the quality of CPR and resuscitation outcomes. 5 Data obtained from some of these devices can also be used in further training and to achieve a higher standard of CPR. 5 A study by Kramer-Johansen et al. 6 showed that the use of automated verbal and visual feedback based on measured quality with a prototype defibrillator improved CPR quality. Yeung et al. 7 indicated that the use of pressure sensor feedback device improved compression depth. However, this technology has not been well-established in out-of or in-hospital settings. Although many feedback devices have been developed to assist CPR, none have been implemented as a standard in patient care.
The aim of this study was to evaluate the chest compression depth and rate during CPR, with and without the CPRmeter feedback device, performed by paramedics and non-paramedics with similar physical characteristics. The additional aim was to assess if there was a difference in the impact of the feedback device between experienced and non-paramedics CPR providers.
Methods
Participants
About 20 men divided into two groups:
Group A (n = 10)—paramedics, students of the fifth year of Public Health with specialty: Emergency Medicine;
Group B (n = 10)—men who were not paramedics but trained to provide CPR.
Inclusion criteria were related to physical characteristics:
Age: between 23 and 26 years
Weight: between 65 and 85 kg
Height: 170–190 cm
The Ethics Review board at the Medical University of Lodz approved the study (approval no. RNN/22/14/KB). The protocols and procedures were explained to all participants who voluntarily provided a written, informed consent to participate. However, participants were blinded to the aim of the study.
Study protocol
Resuscitation was performed with an Ambu Megacode manikin placed on the ground. Participants, in kneeling position on the floor, were examined during resuscitation with and without the CPRmeter feedback device. This position was recommended in the study of Oh et al. 8
The manual CPRmeter with Q-CPR technology is used for CPR. When attached to the bare chest, the CPRmeter provides feedback on CPR compressions including: depth, release, and rate of chest compressions. The CPRmeter has two embedded sensors: the first sensor measures acceleration and the second one measures force.
The sequence of resuscitation methods was randomized. Each participant drew 1 card from 10. If a green card was picked, the participant performed 5-min-resuscitation with CPRmeter. After 1-h break, he was asked again to perform resuscitation but without the device. If a red card was picked, participant performed 5-min resuscitation without CPRmeter first, and after 1-h break, he was asked to perform compressions with the device.
Depth and rate of compressions were evaluated with a BTS Smart DX7000 motion capture system. Reflective markers were put on bony structures of the wrists and hand seen by cameras.
Data processing was performed with the use of SMARTtracker (version: 1.10.451.0), SMARTanalyzer (version: 1.10.0225), Microsoft Excel 2010, and Statistica 10.
Statistical analysis
For statistical analysis, elements of summary statistics were used. To evaluate the distribution of particular parameters, the Shapiro–Wilk Test of normality was applied. For comparison of parameters within particular group, dependent samples t-test was chosen when the distribution was consistent with a normal distribution. In case of comparison between groups for normal distribution of particular parameters, the equality of variances was assessed with the use of Levene test. For equal variances, t-test for independent samples was applied. When variances were not equal, Welch’s t-test was used. Accepted level of significance was α = 0.05.
Results
Elements of summary statistics of compression depths for each group are presented in Table 1. On the basis of dependent samples t-test, statistically significant differences related to depth of compressions, in group A, could be observed in the first minute of chest compression without versus with the device (p-value = 0.0051), and in the first minute versus the fourth minute with the device (p-value = 0.0242). Statistically significant greater depth of chest compressions in group A was observed in the first minute of CPR with the device in comparison to the first minute without the device.
Summary statistics of compressions depth with indication of statistically significant differences between attempts with or without the device in particular group (according to dependent samples t-test).
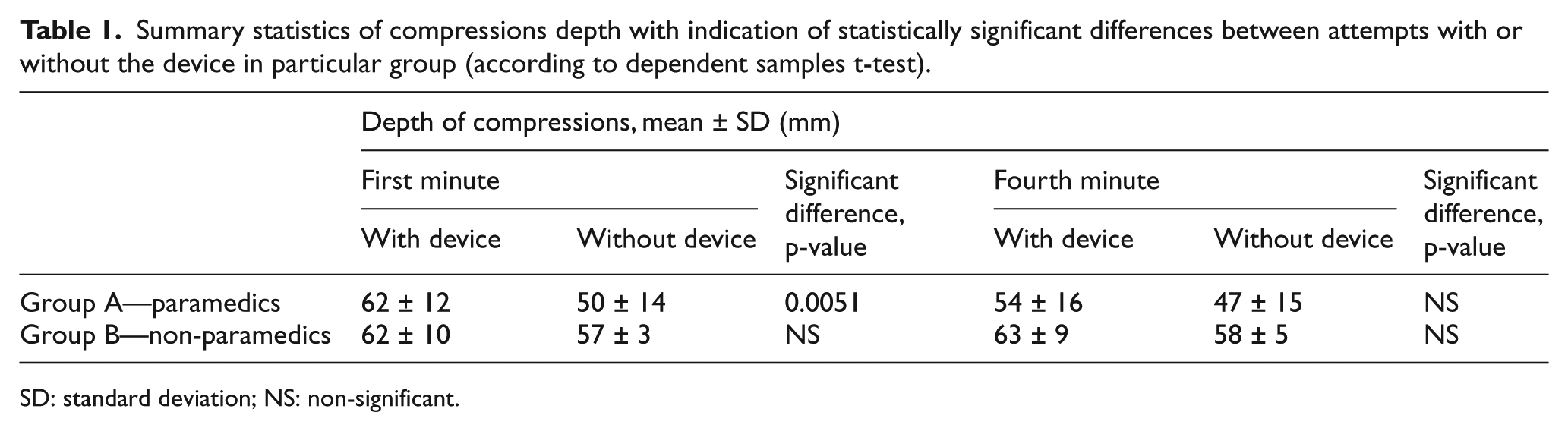
SD: standard deviation; NS: non-significant.
There were no statistically significant differences related to depth of compressions within group B according to dependent samples t-test.
According to t-test for independent samples, there was a statistically significant difference in the first minute of compression without the device between groups A and B (p-value = 0.0378). Moreover, according to Welch’s t-test, there was also a difference between groups in the fourth minute without the device (p-value = 0.0127). In case of both differences, as presented in Figure 1, participants in group B performed deeper compressions.
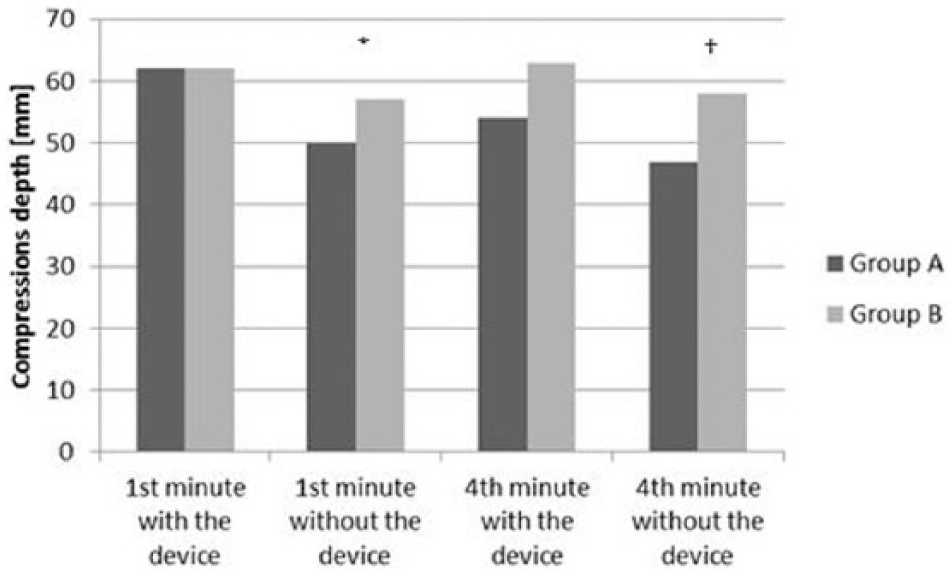
Analysis of compressions depth between groups.
Summary statistics of compressions rate for each group are presented in Table 2. On the basis of dependent samples t-test, statistically significant differences related to rate of compressions, in group A, could be observed in the first minute of chest compression with versus without the device (p-value = 0.0001) and in the fourth minute with versus without the device (p-value = 0.0031). Statistically significant greater rate of chest compression in group A was observed in the first minute of CPR without the device in comparison to the first minute with the device. The same statistical dependence was noticed for CPR in the fourth minute without the device versus the fourth minute with the device.
Summary statistics of compressions rate with indication of statistically significant differences between attempts with or without the device in particular group (according to dependent samples t-test).
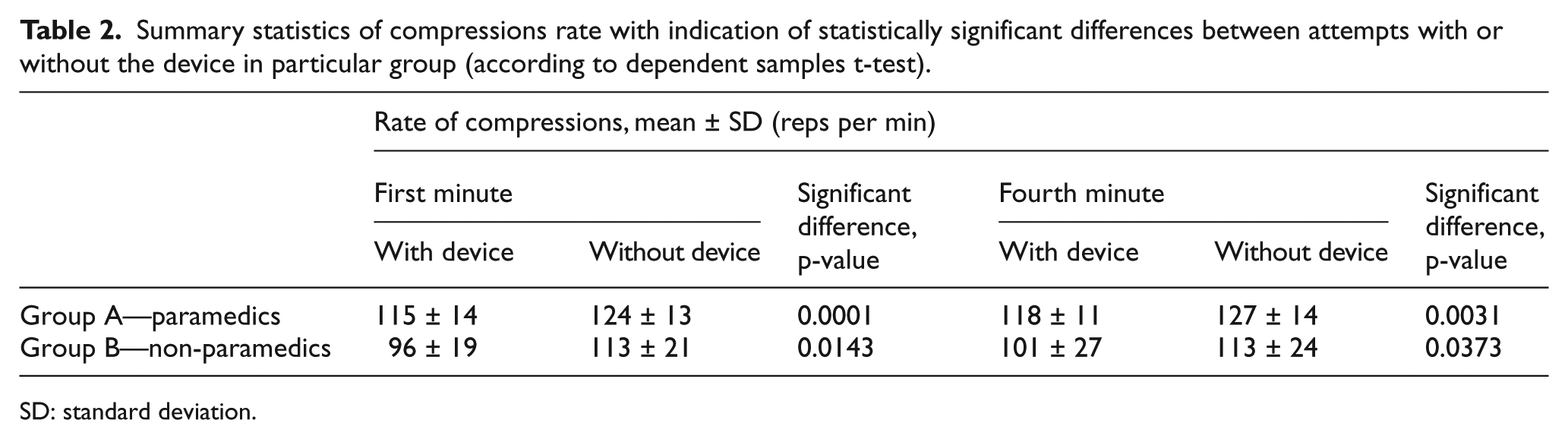
SD: standard deviation.
According to dependent samples t-test, statistically significant differences related to rate of compressions, in group B, could be observed in the first minute of chest compression with versus without the device (p-value = 0.0143) and in the fourth minute with versus without the device (p-value = 0.0373). Statistically significant greater rate of chest compressions in group B was observed in the first minute of CPR without the device in comparison to the first minute with the device. The same statistical dependence was noticed for CPR in the fourth minute without the device versus the fourth minute with the device.
According to t-test for independent samples, there was only a statistically significant difference in the rate of compression in the first minute with the device between group A and B (p-value = 0.0238). Greater rate presented participants in group A (Figure 2).
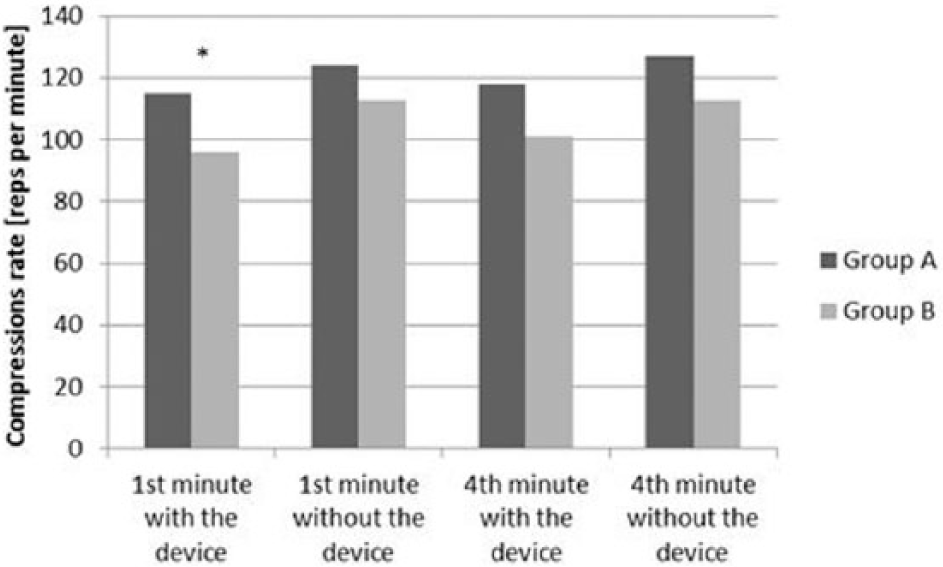
Analysis of compressions rate between groups.
Discussion
According to the past research, there is no difference in outcomes between no CPR and poorly performed CPR. 9 Moreover, results of cardiac arrest are worsened when CPR quality is suboptimal. 10 Therefore, effective chest compressions are essential for providing appropriate blood flow and increase the likelihood of successful resuscitation.
Rapid advances in technology are having a profound effect on the CPR quality. One strategy to gain success in resuscitation involves the use of a feedback device to provide proper depth and rate recommended by the 2015 guidelines. 3 Yeung et al. 7 examined different types of feedback devices and stated that the pressure sensor device improved compression depth and rate, the accelerometer device decreased chest compression depth, and the metronome had no effect. In contrast, Bohn et al. 11 claimed that even metronome and visual feedback may be beneficial to improve CPR. We examined a CPRmeter equipped with an accelerometer and a force sensor, providing therefore real-time information about depth, release, and compressions rate. Our study shows that in the paramedic group (A), there was statistically significant greater depth of chest compressions (above 2015 recommendations) in the first minute of CPR with the CPRmeter in comparison to the first minute without the device. In this group, with time, a significant decrease of chest compressions depth with the device could be noticed. In group B, trials with the CPRmeter exceeded the current recommendations. Differences between group A and B in regard to CPR depth could be observed only in trials without the device.
Mean compression depth with the device was deeper than 6 cm in the first minute of CPR in group A and in both trials in group B, not meeting, therefore, the AHA and ERC criteria.
Mean values of compression rate indicated that attempts without CPRmeter met the criteria of AHA and ERC in the first and fourth minute of compressions in group B, whereas in group A, the rate was too high in both trials. Mean compression rate with the CPRmeter feedback device met the criteria of AHA and ERC in both groups in the fourth minute instead, and only in group A, in the first minute.
It was proved that every 0.5-cm increase in compression depth doubled the chance of successful resuscitation, so a difference of 0.5 cm was considered clinically significant. 12 Reduction of compression depth below recommendations could be the effect of fear of injuries related to increased compression depth. 13 However, increased compression depth is also considered to improve survival and is crucial for the restoration of spontaneous circulation during CPR. Moreover, in out-of-hospital cardiac arrest (OHCA), deeper compressions are associated with higher chance of survival to hospital discharge. 14
According to the past research, professional rescuers in reality compress too shallowly, but during simulated cardiac arrest, they tend to compress too deep. 15 However, in the presented study with a manikin, deeper compressions were performed only with the feedback device. Oh et al. 16 noticed that chest compression depth without the automated audiovisual feedback system was less than when performed with the feedback system. This outcome is similar to the result of this study. Some research suggests that deeper compression improve CPR outcomes.2,14 However, feedback systems may be unreliable, especially during prolonged CPR, because they can increase the risk of thoracic and abdominal injury. 10 Presumably, rescuers proprioception is changed because of the addition of the device under their hands. Due to this, they may underestimate the compression depth and apply excessive compression forces. While researchers present different results related to the association between compressions depth and CPR improvement, the optimal depth is still unknown. In relation to our results, we observed a decreasing depth of compression with the device from the first to the fourth minute in group A.
Nishiyama et al. 17 suggested that rescuers should change their roles every 1 min to maintain the quality of chest compressions, especially decreasing depth. McDonald et al. 18 as well as Russo et al. 19 supported the recommendation to change CPR providers after 2 min because of the decrease in compression depth over time. Schober et al. 20 stated that more than two rescuers should alternate with chest compressions due to the fatigue and new strategies to improve CPR depth should be investigated. In our study, we did not alternate rescuers due to the short time of the investigation. In future studies, this time of investigation should be increased due to the assumption that the use of CPRmeter can improve resuscitation parameters over time.
Decreased depth of compression during CPR could not similarly be seen in our study for group B in none of the trials. Their results, although stable, exceeded the depth of 6 cm for attempts with CPRmeter.
Some authors failed to sustain chest compression quality according to ERC guidelines even when they used a real-time feedback system, therefore suggesting that the usefulness of a fixed chest compression depth should be investigated. 21
In our study, both groups seemed to benefit from the CPRmeter over time, with the non-paramedics group being though always on the edge of meeting the 2015 guidelines. 3 Generally, paramedics from group A obtained higher rate of compressions than participants in group B. In daily clinical conditions CPRmeter seemed to be useful device to gain stable parameters during prolonged resuscitation.
Buléon et al. 22 examined a CPRmeter feedback device and concluded that it improved chest compression quality in case of people inexperienced in CPR. Those results, related strictly to the CPRmeter, can be subjected to discussion. On one hand, in our study, the parameter related to CPR quality—the depth of chest compressions with versus without the CPRmeter—exceeded 2015 ERC and AHA recommendations in the majority of the trials. On the other hand, a second parameter related to CPR quality—compressions rate with versus without the CPRmeter—improved according to the 2015 guidelines in group A. The device could be recommended for novice paramedics and Emergency Medicine students to improve the quality of resuscitation.
This study had several limitations. It was carried out in laboratory settings and did not replicate all the aspects of a real-life CPR. Attempts were conducted on a manikin; therefore, the application of these data to humans is questionable. While a manikin is a good tool in training, it does not provide the same experience of chest compressions as on patients. It is worth to mention, however, that one manikin was a standardized model for all participants; therefore, the comparisons should be valid. Another limitation was the small sample size of the study, restricted by the inclusion criteria. Nevertheless, data obtained from this sample can be promising for further analyses.
This study had also a number of strengths. In relation to the inclusion criteria, participants were comparable according to height, body mass index (BMI), and age. Differences in those parameters can influence the results of CPR quality. 17 We compared CPR quality in professional and non-professional groups, which gives broader information about the usefulness of the tested feedback device. Finally, we have offered an objective analysis of the CPR depth and rate with the use of an optoelectronic system with high accuracy.
Conclusion
On the basis of obtained results, the following conclusions could be drawn:
As far as the depth of compression is concerned, only the group of paramedics showed in time some benefits of the device, whereas for the group of non-paramedics the device seemed to have even a deleterious effect. However, the non-paramedics group satisfied the recent AHA and ERC criteria in trials without the feedback device, when the paramedics had a worsening of results.
As far as the rate of compression with the feedback device is concerned, the group of paramedics met the AHA and ERC recommendations all the time, while the non-paramedics only in the fourth minute of the procedure. Here again, the group of non-paramedics showed stable and proper results in trials without the feedback device.
Real-time feedback device can be recommended for novice paramedics and Emergency Medicine students because it seemed to improve the quality of resuscitation over time.
Footnotes
Acknowledgements
The manuscript has been read and approved by all authors: M.F-.W.: conception and design of the work, analysis, and interpretation of data for the work (30%). K.K.: revising the work for important intellectual content (20%). A.J.: data acquisition (20%). G.P.: revising the work for important intellectual content (20%). T.G.: final approval of the version to be published (10%).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Submitted work is original and has not been published elsewhere in any language. Raw data are available for editor on request.
Informed consent
All participants gave their written, informed consent prior to their inclusion in the study.
Ethical approval
The study was approved by Ethics Committee of Medical University of Lodz, Poland. Approval number obtained for human investigation is RNN/22/14/KB.
Human rights
Authors declare that human rights were respected according to Declaration of Helsinki.