
Abstract
Objectives:
To report and analyse the poisoning data of Hong Kong Poison Information Centre in 2017.
Methods:
In 2017, all poisoning cases received by Hong Kong Poison Information Centre were retrieved from its database (Poison Information and Clinical Management System) for analysis.
Results:
A total of 3956 poisoned cases were analysed. There were 1789 male patients (45.2%), 2159 female patients (54.6%) and 8 sex-unspecified patients (0.2%). The majority of cases (59.9%) were between 20 and 59 years old. The common causes of poisoning were suspected self-harm/suicidal attempt (36.2%), unintentional exposure (18.6%) and abusive substance use (13.7%). Excluding the common co-ingestant ethanol, the five commonest types of poison were benzodiazepines, paracetamol, zopiclone, Chinese herbal medicine and household products. Most patients were managed with supportive measures, while 17.4% and 13.2% of consultation cases were treated by decontamination and antidotes, respectively. The majority of the cases had uneventful recovery; 1.1% resulted in death and 4.3% had major outcomes. A total of 13 interesting cases and 1 poisoning outbreak were discussed.
Conclusion:
This 12th annual report provided the updated epidemiological information on poisoning pattern in Hong Kong and highlighted important changes in comparison with our previous reports.
Keywords
Introduction
The Hong Kong Poison Information Centre (HKPIC) was established in 2005. Currently, it provides round-the-clock phone consultation service to health care professionals in Hong Kong for poison information and clinical management advice on poisoning. It also provides onsite clinical toxicology service to poisoned patients in United Christian Hospital where the centre is located. HKPIC also collects important poisoning epidemiological data in Hong Kong from voluntary poisoning reporting in Hospital Authority (HA). It also contributes to the development of clinical toxicology and emergency medicine by organising regular training activities such as monthly seminar, basic clinical toxicology course, certificate course and the 1-year quotable diploma course in clinical toxicology (Dip Clin Tox (HKCEM & HKPIC)) and fellowship training programme in conjunction with the Hong Kong College of Emergency Medicine (HKCEM), as well as training for overseas doctors. Besides, HKPIC published four articles in peer review journal in 2017, adding up to a total of 99 articles since its establishment. The mission of the HKPIC is to minimise the mortality and morbidity of poisoning by the provision of high-quality clinical toxicology service and to become one of the leading toxicology training centres in Asia-Pacific region.
HKPIC has started to publish its annual reports since 2006. It continues to provide the updated information in poisoning epidemiology and its changing trend in Hong Kong. This 12th annual report of HKPIC covers the data in 2017, and as in the previous reports to focus on the latest poisoning pattern and highlight some important poisoning cases in Hong Kong.
Methods
The HKPIC received its poisoning cases from two primary sources: consultation and reporting. Consultation is defined as poisoning case that health care professional consulted us for the poison information and management advice, while reporting is defined as the poisoning case reported in HA, majority by all accident and emergency department (AED). In 2017, all poisoning cases received by HKPIC were retrieved from its database, that is, Poison Information and Clinical Management System (PICMS) for analysis.
The data of each poisoning case were inputted into PICMS according to the information obtained from the consulting health care professional, medical record, electronic patient record (ePR) of HA and other relevant sources. Data collected included patient demographic data, poison data (poison type and dose, route, time, place and reason of exposure), clinical data (clinical features, investigation results), management data (use of decontamination, antidotes and other specific treatments) and outcome data (AED patient, final outcome and its relationship to the poison exposure) for consultation cases, while only patient demographic data, poison data and outcome data were inputted for the reporting cases.
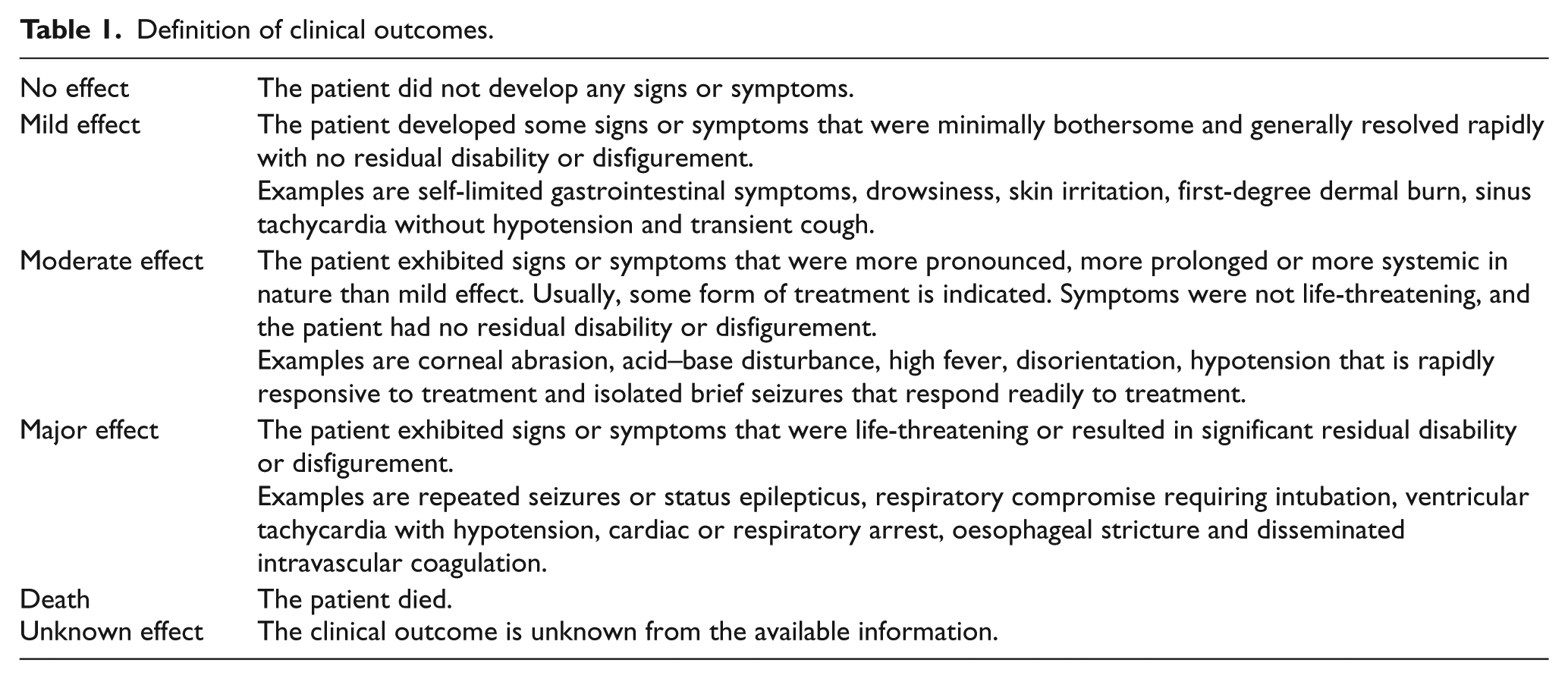
Senior doctors from the HKPIC would classify the outcome of the cases into five categories: no effect, mild effect, moderate effect, major effect or death with reference to the American Association of Poison Control Centers’ National Poison Data System 1 (Table 1). Besides, the relationship between the poison exposure and clinical outcome was graded as definite, probable, possible, not related or undetermined/not applicable according to the available information. All death or major effect cases were further reviewed by a second senior to ensure that the grading was appropriate.
Definition of clinical outcomes.
Information used in this annual report was considered as a part of the usual clinical data obtained by HKPIC and was passed to the researchers in a fully anonymised format.
Results
After excluding duplicate and invalid cases, the PICMS generated 3956 (100%) valid cases, including 2114 (53.4%) consultation cases and 1842 (46.6%) reporting cases for analysis in the year 2017.
The age and gender distributions of the cases are shown in Figure 1. There were 1789 male patients (45.2%), 2159 female patients (54.6%) and 8 sex-unspecified patients (0.2%). A female predominance was noted in the majority of the age groups except for the children of age 0–12 years and for elderly from age 60 to 79. Concerning the age distribution, the middle-aged group (30–39 years) was the commonest, and the majority (59.9%) of them were between 20 and 59 years. Around one-tenth of the cases (11.4%) were children from the age of 0–5 years.
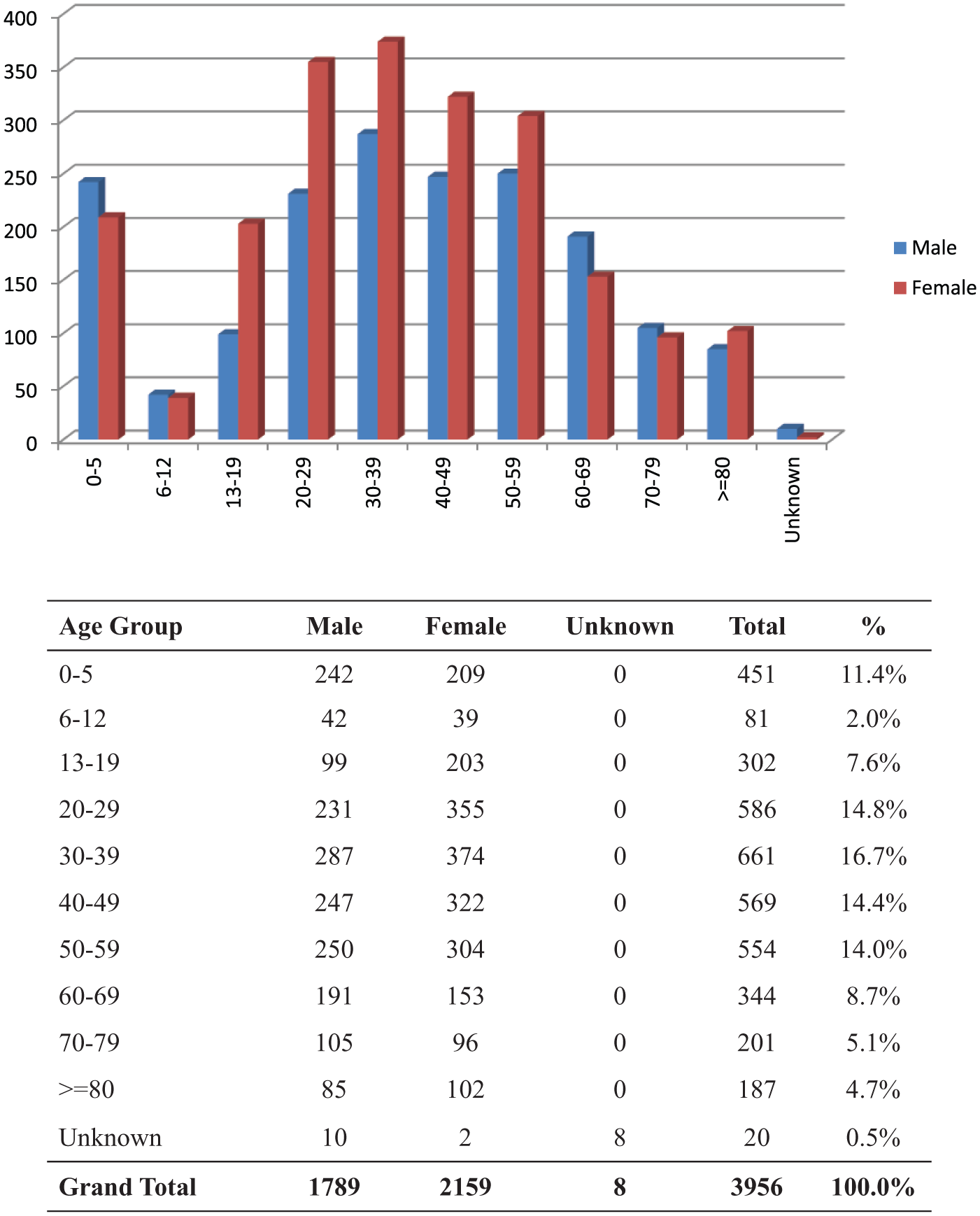
Age and gender distribution.
The reasons for poisoning are listed in Figure 2 with the most frequent cause being suspected self-harm/suicidal attempt which accounted for 36.2% of the cases. Poisoning due to unintentional exposure (18.6%) and abusive use (13.7%) had ranked the second and third commonest causes, respectively. Together with venomous bites and stings (8.7%) and adverse reactions secondary to herbal or proprietary Chinese medicine (7.6%), these five commonest reasons for poisoning contributed to the vast majority (84.9%) of the cases. As shown in Figures 3 and 4, the commonest place of exposure was in the patient’s residential place (59.0%). The commonest route of poisoning was oral exposure (82.5%), followed by inhalational (6.8%) and dermal exposure (6.6%).
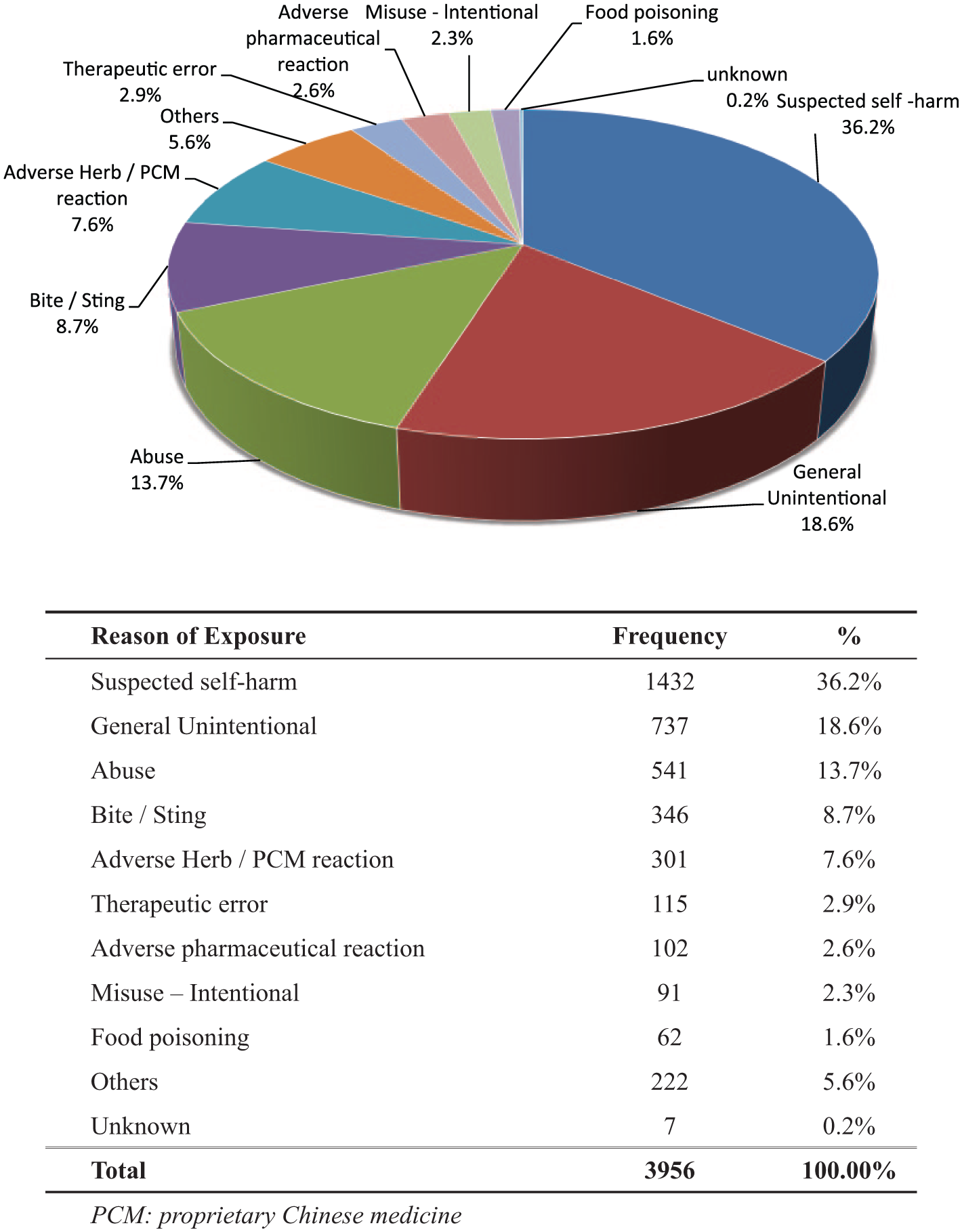
Reason of exposure.
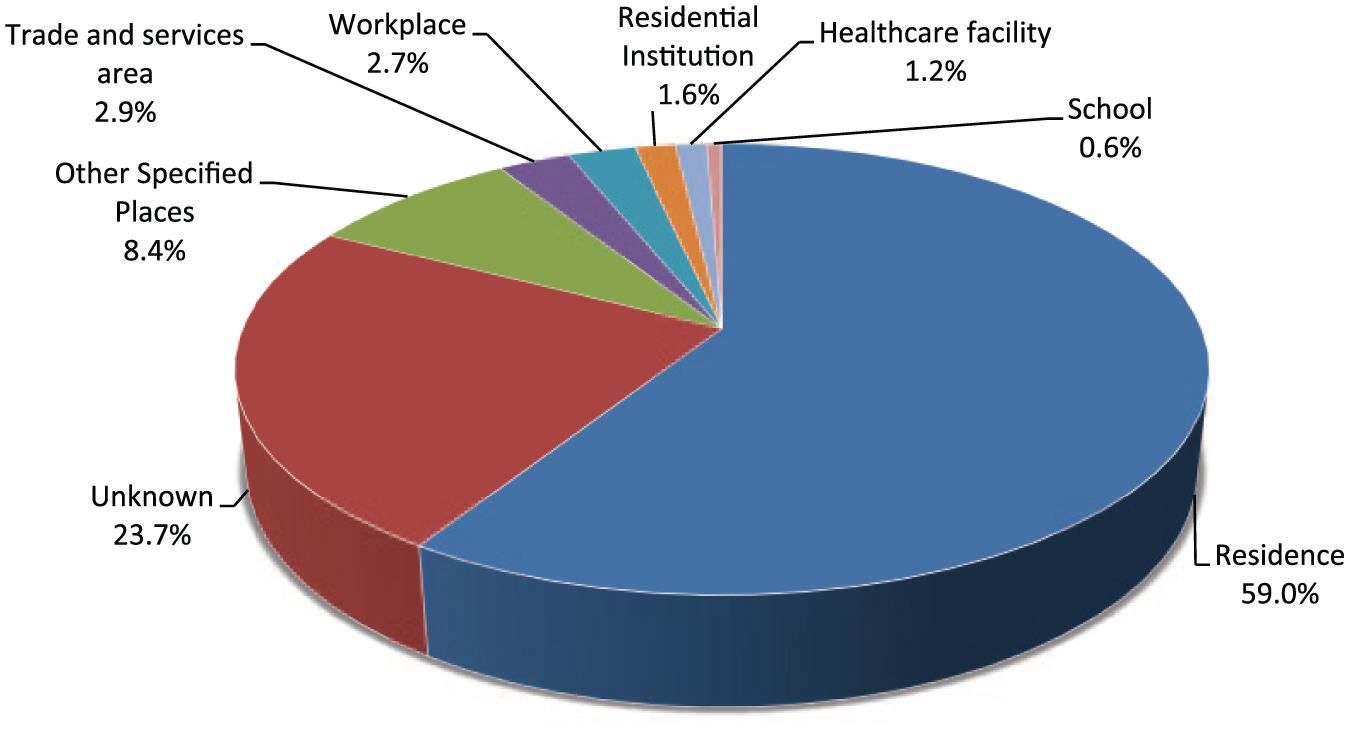
Place of exposure.
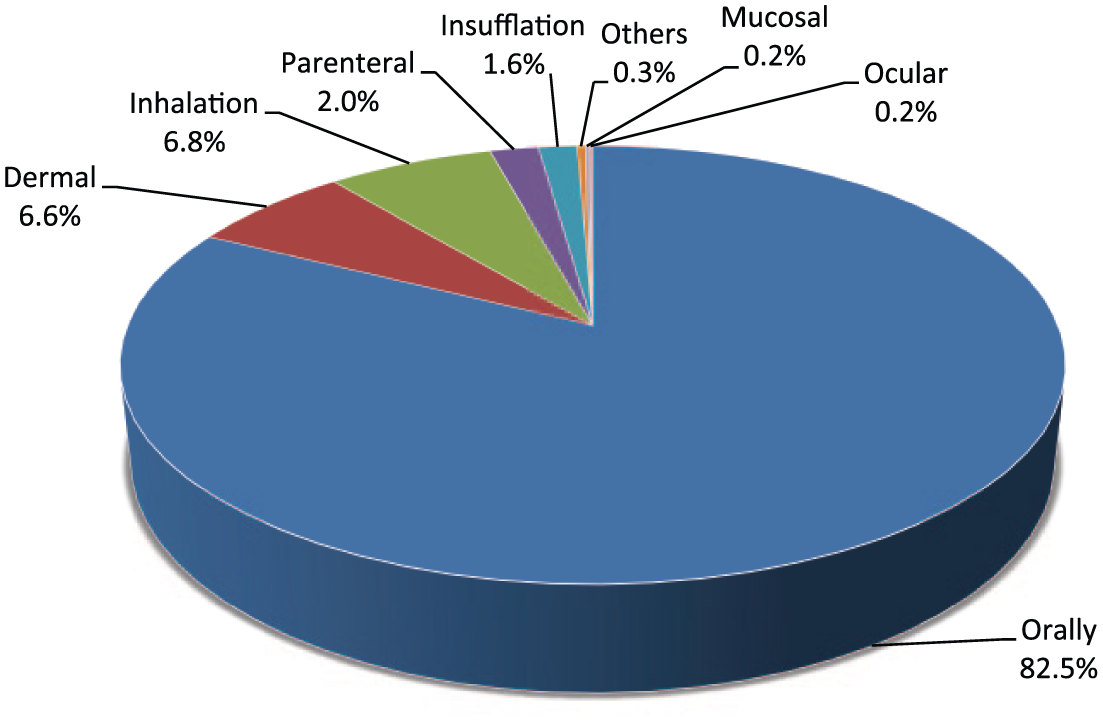
Route of exposure.
A total of 5932 poisons were involved in the 3956 cases. About three quarters of the cases (72.5%) had exposed to a single poison, while the remaining (27.5%) cases had exposed to multiple poisons. Types of poison exposure are shown in Figure 5. Apart from ethanol which was commonly involved as a co-ingestant, the five commonest types of poison were benzodiazepine (384 cases), paracetamol (349 cases), zopiclone (288 cases), Chinese herbal medicine (CHM; 277 cases) and household products (266 cases).
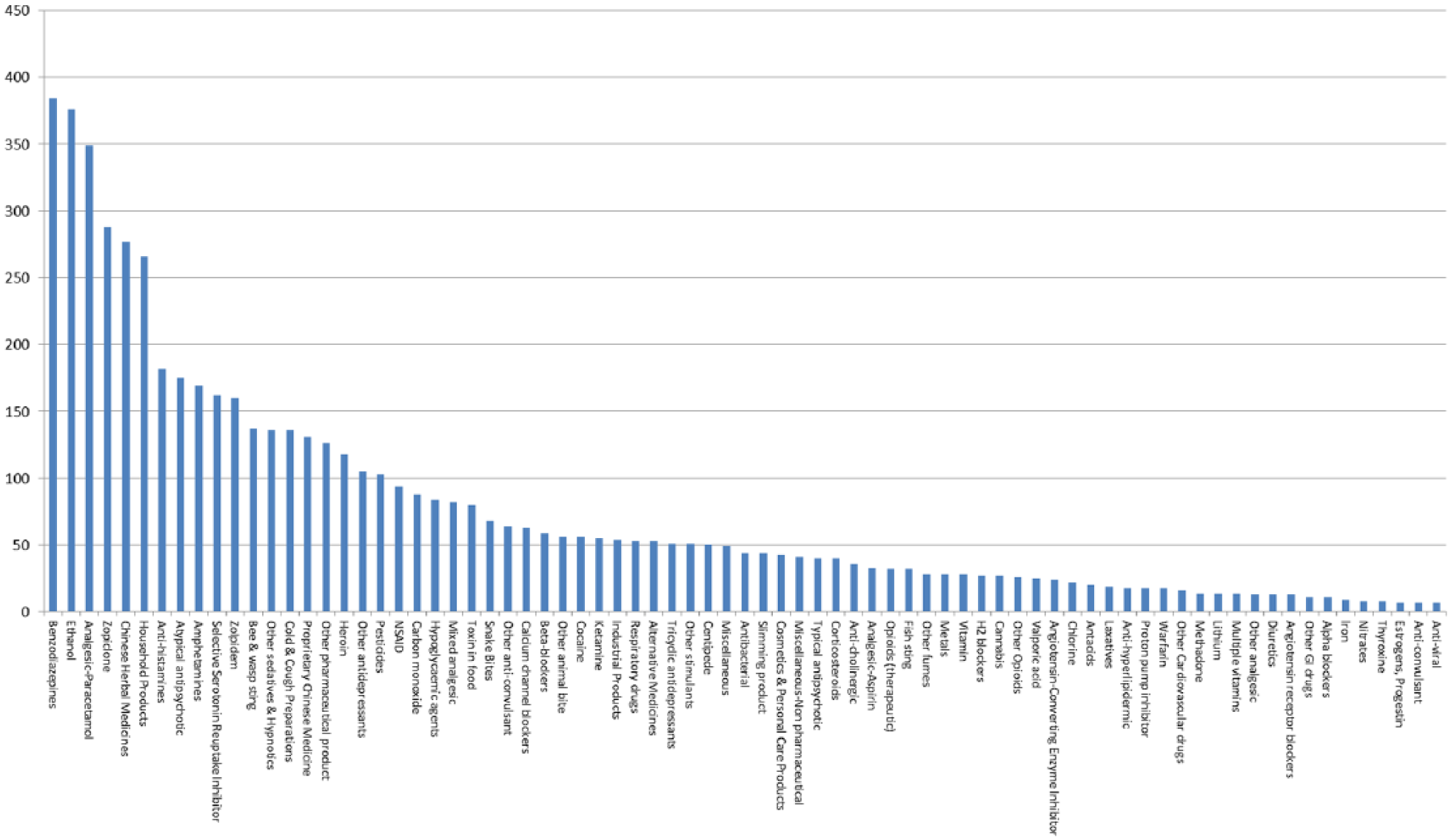
Types of poison exposure.
For the analysis on the management in terms of decontamination and antidote use, only the consultation cases were included. For the 2114 (100%) consultation cases, 368 (17.4%) patients underwent decontamination including 27 of them given multiple decontamination methods, the commonest method was single-dose activated charcoal (AC) (94.6%), followed by gastric lavage (7.6%) and multiple-dose AC (2.7%) as shown in Table 2. Regarding the antidote use, 280 (13.2%) patients were treated with antidotes and 39 of them were given more than one antidote. The five commonest antidotes used were N-acetylcysteine (NAC), benzodiazepines, snake antivenin, calcium and sodium bicarbonate as listed in Table 3.
Decontamination.
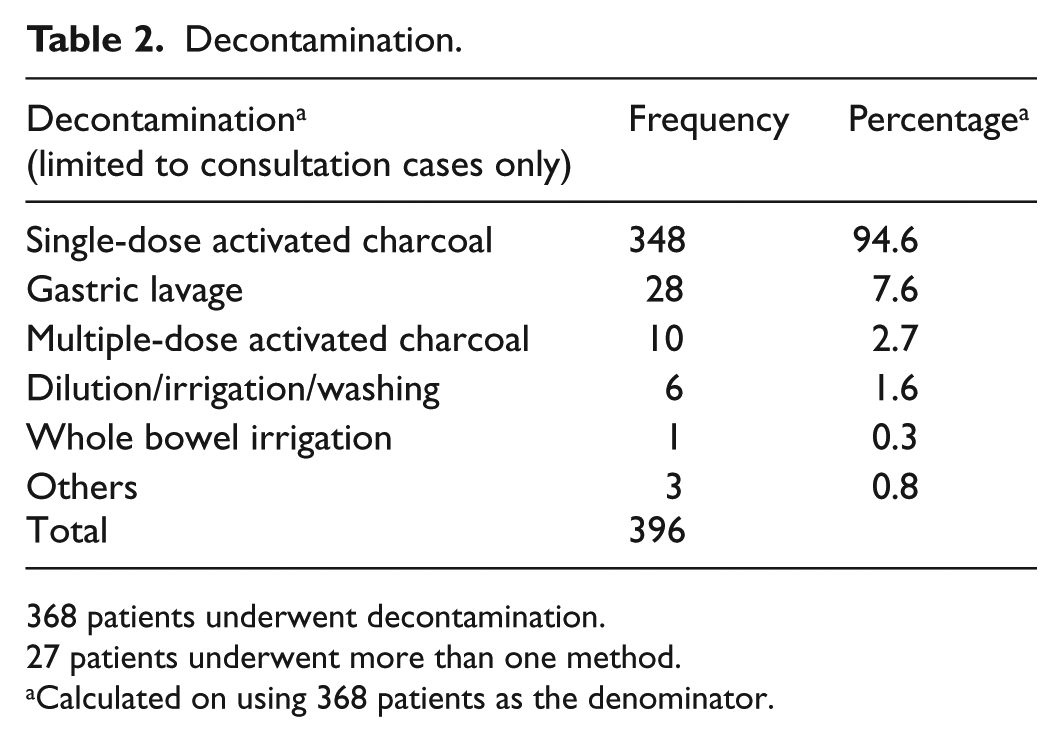
368 patients underwent decontamination.
27 patients underwent more than one method.
Calculated on using 368 patients as the denominator.
Antidotes.
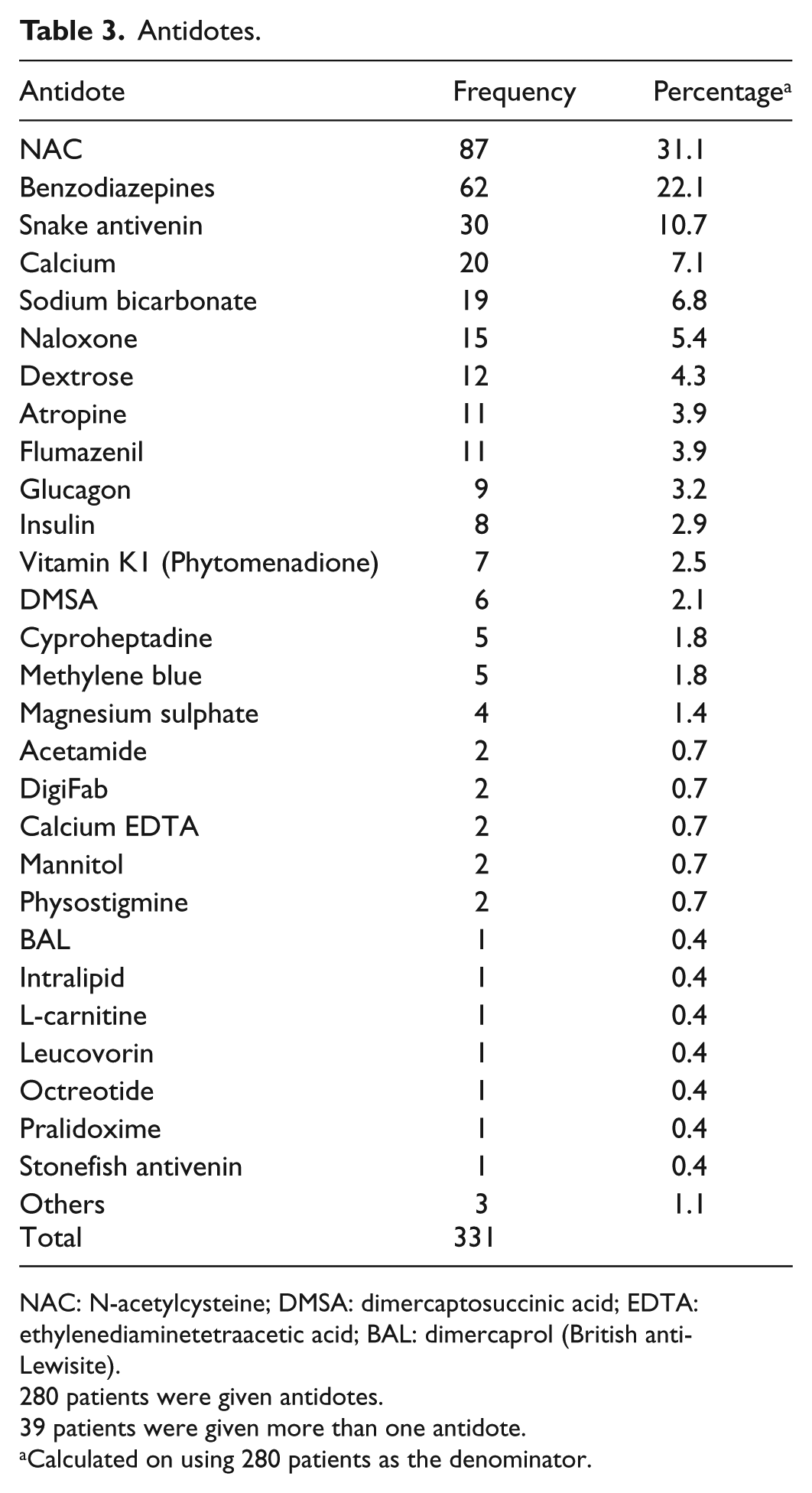
NAC: N-acetylcysteine; DMSA: dimercaptosuccinic acid; EDTA: ethylenediaminetetraacetic acid; BAL: dimercaprol (British anti-Lewisite).
280 patients were given antidotes.
39 patients were given more than one antidote.
Calculated on using 280 patients as the denominator.
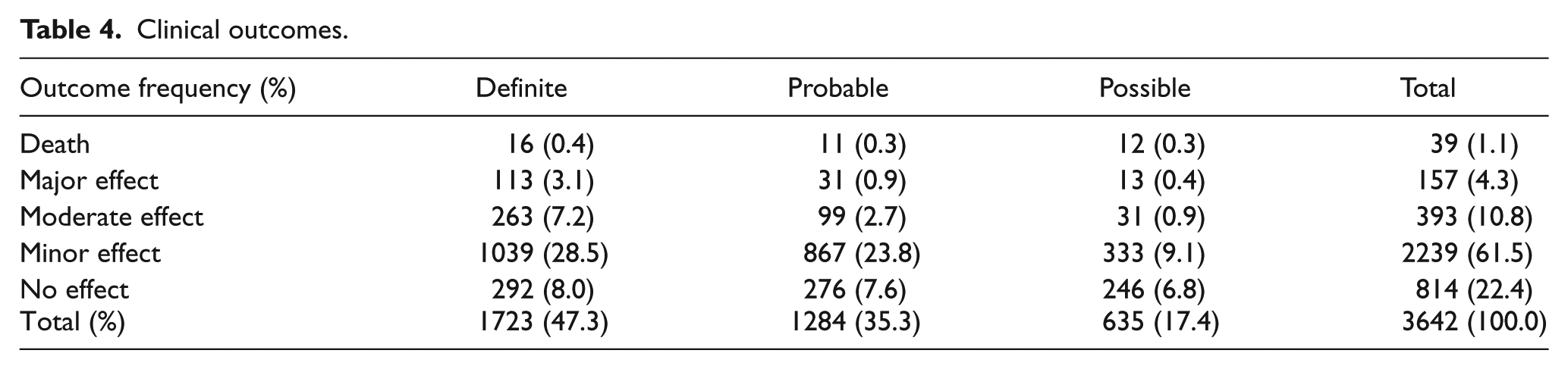
After excluding 314 cases in which the clinical outcomes were graded as not related to the poison exposure, or clinical outcome cannot be assessed from the available information, the remaining 3642 cases (100%) were analysed for the outcome. There were 39 deaths (1.1%), 157 cases of major effects (4.3%), 393 cases of moderate effects (10.8%), 2239 cases of mild effects (61.5%) and 814 cases of no effect (22.4%), as shown in Table 4. From another point of view, 47.3%, 35.3% and 17.4% of the outcomes were graded as definitely, probably and possibly related to the poison exposure, respectively.
Clinical outcomes.
In 2017, we have received 213 consultations on pre-hospital AC administration. Among these 251 patients, 123 (57.7%) patients were given AC by ambulance paramedics. The remaining 90 (42.3%) patients were either not indicated for AC administration, or judged to be not feasible for AC administration during the ambulance transfer.
Discussion
This 12th annual report of HKPIC analysed the data of 3956 poisoned cases in 2017 which represented the updated poisoning pattern in Hong Kong.
The poisoning reporting is not compulsory and it remains one of the intrinsic limitations in our poisoning data, which is common to other poisoning databases in developed countries. However, HKPIC recorded around 4000 cases yearly, the comparable figures of death and major outcomes over the past few years. We believe that we have captured the majority of poisoning cases for analysis.
The pattern of age and gender distribution and routes of exposure were grossly similar when compared with our previous reports and overseas data.1,2 However, we observe that there were 18.0% and 18.4% increases in the age groups of 13–19 years and older than 80 years, respectively, in 2017 compared with the data in 2016. Whether the increase in poisoned cases in these age groups is due to a true increased incidence or the increased utilisation of the reporting system needs further monitoring and future studies.
The three commonest reasons of exposure, namely, suspected self-harm, unintentional exposure and substance abuse, remained the same as the data of the previous year. The five commonest types of poison exposure were benzodiazepines, paracetamol, zopiclone, CHM and household products. According to the HKPIC data of years 2016 and 2017, benzodiazepines remained as the commonest poison.
Over the past 5 years (2013–2017), benzodiazepine and paracetamol exposure ranked either the first or second commonest poison and each was involved in an average of 9% of our poisoning cases. Benzodiazepine and zopiclone poisoning commonly occurs in intentional self-harm, as a sole poison or co-poison in multiple poison exposure. For CHM, the poisoning was frequently related to herb-induced liver injury and aconite poisoning from the data in 2017. Household products are commonly encountered in intentional overdose in adults as well as accidental exposure in children. Cleansing agents, antiseptics and bleaches were the three commonest poisons involved in household products.
In this year, the proportion of our consultation cases treated with decontamination (17.4%) is higher than the average of 15.5% in the previous 5 years and the proportion of 14.3% in 2016. Concerning the method of decontamination, the use of single-dose AC remained the commonest method as expected from our local experience and overseas poison centre data.1,2 The proportion of antidotes (13.2%) was about the same as the average of 14.1% in the previous 5 years. The reason why the proportion of decontamination increased abruptly in 2017 needs further monitoring.
Among all types of antidotes, NAC, benzodiazepines and snake antivenins were the three most commonly used antidotes. NAC has been the commonest antidote in all of our previous annual reports except in 2008. NAC was given in one-fourth of the paracetamol poisoning cases. It may also be used to treat other poisonings such as amatoxin and paraquat with limited evidence. Benzodiazepine and snake antivenin use accounted for one-third of the antidote use. Interestingly, the proportion of benzodiazepine use was remarkably increased from 12.8% in 2016 to 22.1% in 2017. Among those 62 cases treated with benzodiazepines, around three-fourth of the cases (72.6%) involved stimulant drugs and sedative agents as they commonly presented with agitation, confusion or seizures. Snake antivenins, calcium and sodium bicarbonate ranked the third, fourth and fifth most commonly used antidotes. The patterns of their use were similar and together accounted for about one-fourth (24.6%) of the cases treated by antidotes. Notably, there was the use of mannitol reported for two patients in 2017, due to an outbreak of ciguatoxin poisoning.
Concerning the clinical outcome, the poisoning death rate in 2017 was 1.1%, which is similar to the average in the past 5 years (Table 5). The proportion of the major effect was 4.3% and remained comparable in recent years with an average of 4.4%. On the other hand, the majority of the cases (83.8%) were classified as no effect or mild effect, which again was similar to our data in recent years.
The HKPIC annual report’s important figures in the last 5 years.
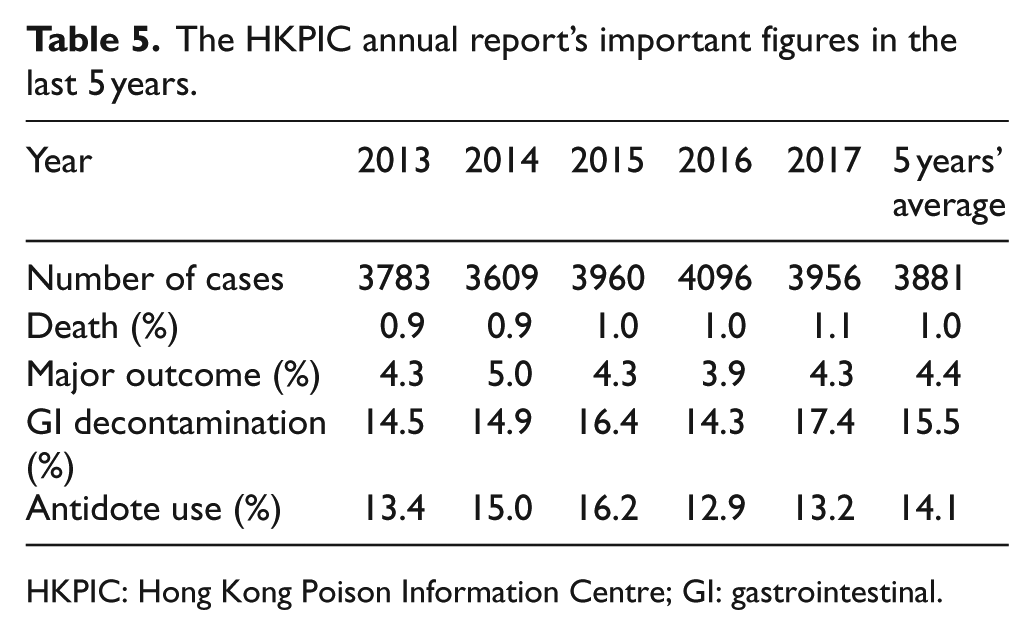
HKPIC: Hong Kong Poison Information Centre; GI: gastrointestinal.
There are limitations of this report as mentioned in our previous annual reports. First of all, reporting of poisoning cases in Hong Kong is on a voluntary basis. Second, the data obtained from the consulting medical professionals may not be comprehensive. However, as the most poisoning cases were managed in HA hospitals with the patient clinical records accessible by ePR, the accuracy and amount of information were expected to be much better than those of the data obtained from other poison centres which may not have direct access to the patient records in their managing hospitals. Third, in some of the cases with limited clinical information, it is difficult to make definite judgement on the causal relationship between the outcome and the poison exposure.
Conclusion
This 12th annual report provides the updated epidemiological information on poisoning in Hong Kong in 2017 and highlights some changes in the pattern of poisoning demography, decontamination and antidote use as compared with our previous reports. Concerning outcome, 1.1% and 4.3% of the cases resulted in death and major outcome, respectively. HKPIC will continue to monitor the poisoning pattern in Hong Kong to facilitate the formulation of strategies in poison control and prevention.
Interesting cases
Case 1
A schizophrenic patient in his 30s attempted suicide by ingesting a solution made from 15-g cantharides [斑蝥], which was bought through the Internet. He developed haematemesis, haematuria and dysuria and presented to an AED 2 hours after the ingestion. He was afebrile with a Glasgow Coma Scale (GCS) score of 15/15, a blood pressure level of 115/90 mmHg, a pulse rate of 127 bpm, a respiratory rate of 18 per minute and an SpO2 level of 100% on room air. Physical examination was unremarkable, and the chest X-ray and electrocardiography (ECG) were normal except sinus tachycardia of 117 bpm. HKPIC was consulted and the patient was assessed by a clinical toxicologist at the bedside. Cantharide poisoning was diagnosed and the reported ingested dose was considered to be fatal. Gastrointestinal decontamination was performed by nasogastric tube insertion (Ryle’s tube) and gentle gastric irrigation. He was managed with intravenous normal saline and transamine for the significant haematemesis and haematuria. He was then transferred to the operation theatre directly for oesophagogastroduodenoscopy (OGD) under general anaesthesia. OGD found Zargar grade IIA oesophagitis, Zargar grade I gastritis and duodenitis. He was admitted to intensive care unit (ICU) for monitoring and supportive care afterwards. He developed hypotension requiring high-dose inotropes for about 1 week, remained intubated for 10 days and complicated by liver and renal impairment, hospital-acquired pneumonia and rhabdomyolysis. He survived after 2 weeks of ICU stay. Follow-up OGD at about 1 month after ingestion showed residual mild gastritis only. He was transferred to a psychiatric hospital at about 5 weeks after the initial presentation. Cantharidin [斑蝥素], the toxic ingredient of cantharides, was detected in the patient’s urine, gastric aspirate and the cantharides herbal powder remnant. The case was reported to the Department of Health.
Cantharides, a dried and powdered blister beetle of the Mylabris genus, is a schedule I Chinese medicine in Hong Kong. It contains about 1%–1.2% cantharidin (3,6-epoxy-1,2-dimethylcyclohexane-1,2-dicarboxylic anhydride) as the toxic ingredient. The lethal dose of cantharidin in adults has been estimated to be 10–80 mg. 3 Its toxic mechanism is not well established. Most of its clinical effects are attributable to direct chemical irritation and possibly related to binding at the cellular level, where it has been found to be a potent inhibitor of type 1 and 2A protein phosphatases. Cantharidin was bound to albumin and undergoes excretion by glomerular filtration, causing glomerular damage and acute tubular necrosis, as well as blister formation in the lower urinary tract. 4 Symptoms of cantharidin intoxication typically begin within 1–2 h of ingestion. Initially, physical complaints include burning and blistering of the mouth, tongue and oropharynx, dysphagia, abdominal pain, vomiting and haematemesis. Urinary symptoms including dysuria, urinary frequency and haematuria and, less commonly, coagulopathy, seizure and flaccid paralysis have been reported. 5 Death commonly results from acute kidney injury, cardiovascular collapses and multi-organ failure. Management is mainly supportive treatment, with rational decision on gastrointestinal decontamination. There is no specific antidote, and enhanced elimination of cantharidin is generally not recommended.
This patient ingested 15-g cantharides with an estimated cantharidin content of 150–180 mg, which is well above the reported lethal dose. Multi-specialties’ high-quality care, including gentle gastric irrigation (by nasogastric tube) in removing the unabsorbed cantharidin at the AED, contributed to his survival. Besides, it is worthwhile noting that it is possible to obtain such a highly toxic Chinese medicine from the Internet sources.
Case 2
A 17-month-old toddler, born in Hong Kong, was found to have lead poisoning during the investigation of an outbreak from the use of ‘Chinese herbal medicine (CHM) powder’ in Shenzhen 3 months before. She was hyperactive and irritable after using the ‘CHM powder’. Blood lead level (BLL) at that time was 56.9 mcg/dL. Three courses of intravenous chelation therapy with calcium disodium edetate were given before she came back to Hong Kong.
Upon evaluation, the patient was asymptomatic with no active complaints. The BLL repeated was 34 mcg/dL. Complete blood picture and renal function test were normal. X-ray of the knee showed ‘lead lines’ in the metaphyseal regions of the lower femur and upper tibia (see Figure 6). Oral Succimer (dimercaptosuccinic acid (DMSA)) was given, with her BLL being monitored, which was around 20 mcg/dL in a year after she came back to Hong Kong.
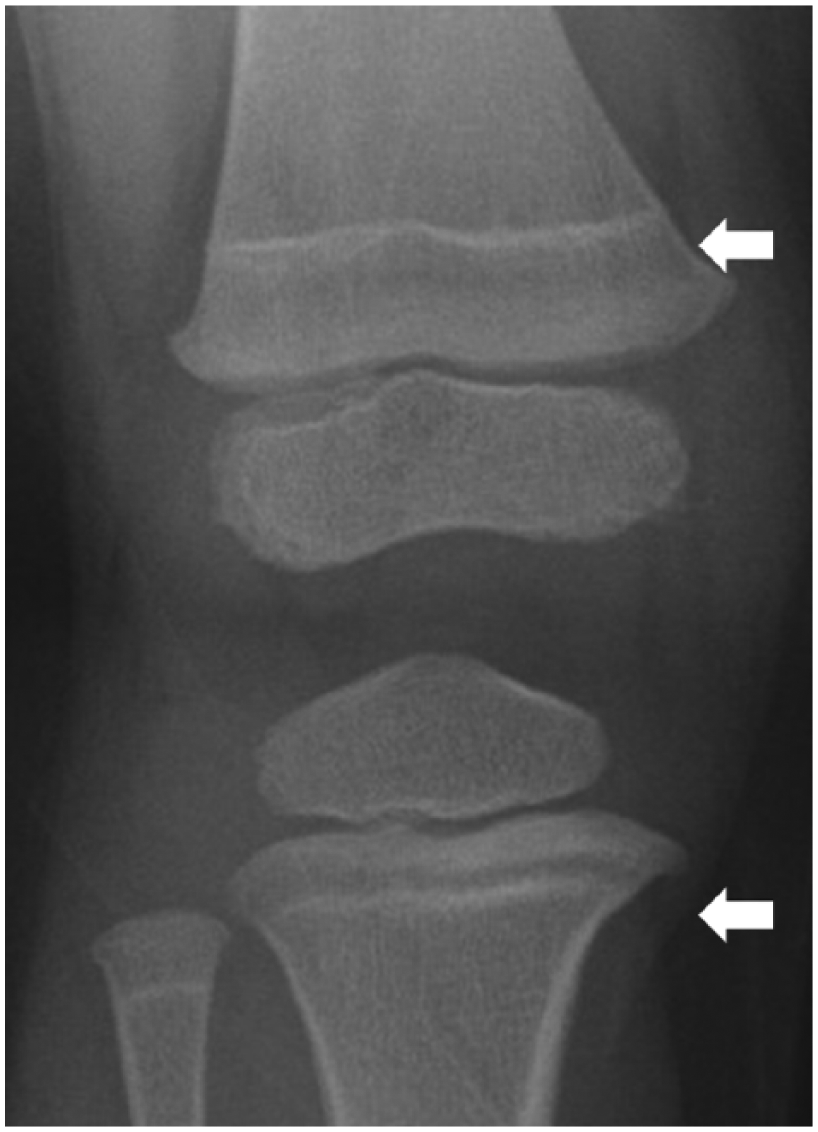
X-ray of the patient showing ‘lead lines’ (bands of increased metaphyseal density on radiographs of long bones in young children).
Adulteration of CHM has been reported to be a cause of lead poisoning in Hong Kong. 6 Anaemia, the central nervous system effects like hyperirritable behaviour, intermittent lethargy and gastrointestinal symptoms like vomiting, abdominal colic and anorexia may be observed in children with the BLLs of 45–69 mcg/dL. 7 Impaired cognition, reduced intelligence quotient, short stature and so on may also be associated with a lower BLL. 8 Source identification and removal from exposure is the most important step. Chelation therapy is recommended for children with BLL of more than 45 mcg/dL. 9 The management of asymptomatic children with a BLL of 20–44 mcg/dL is controversial. Potential indications for chelation treatment in this group include BLL at the higher end of the range, persistently raised BLLs despite environmental control, younger children or clinical or biochemical hints of lead toxicity. 10
Case 3
A 19-month-old toddler, with normal G6PD status, was found holding a bag of her parental grandmother’s Pyridium® 100 mg. Totally six tablets were missing. The maximum dose of exposure was estimated to be 63 mg/kg (body weight – 9.5 kg). She developed unprovoked vomiting of partially digested tablets 20 min later, and she was noted to have yellow sclera as well. She was admitted to a paediatric ward and became irritable, with SpO2 being dropped to 85% on room air which improved to 92% on high-flow oxygen via a non-rebreathing mask. Her methaemoglobin (MetHb) level was 18.8% on co-oximetry, and blood gas showed mildly compensated metabolic acidosis with a lactate level of 4.7 mmol/L. She was transferred to paediatric ICU and intravenous methylene blue (MB) 1 mg/kg was given for her methaemoglobinaemia. She was noted to have desaturation after MB administration (from 95% to 90%) and non-invasive ventilation was given for her ‘persistent desaturation’ although her blood gas showed a PaO2 level of 58.5 kPa. Her methaemoglobin level subsequently dropped to 2.6%.
She also developed acute haemolysis with haemoglobin (Hb) drop from 12.9 to 9.7 g/dL and total bilirubin level raised from 21 to 51 µmol/L (unconjugated bilirubin level 46 µmol/L) in the first day. She remained clinically well afterwards and was transferred back to a general ward on day 3 and discharged home on day 4.
Pyridium (phenazopyridine) is an azo dye used as a urinary analgesic. Methaemoglobinaemia and cyanosis are the most common manifestations of phenazopyridine intoxication in children, and ingestion of 1–2 tablets may result in clinical cyanosis requiring MB treatment. 11 Other toxicities including haemolysis, acute renal failure, commonly secondary to haemolytic anaemia, rhabdomyolysis, jaundice and raised liver enzymes have been reported. Yellowing of sclera can be a result of red-orange discolouration after drug use (as in our case at the first presentation), or due to raised bilirubin level secondary to haemolytic anaemia as in day 1 in our case. Treatment is mainly supportive with MB for methaemoglobinaemia. After MB treatment, peripheral pulse oximeter would give a falsely low oxygen saturation reading as MB absorbs most of the 660-nm light emission from the pulse oximeter, in which case blood gas should show a normal PaO2. In case of doubt, arterial blood gas should be checked. 12
Case 4
A 1-year-old baby, with a history of chronic constipation, suffered from fever and influenza-like symptoms for a week, as well as constipation for 4 days. She was noticed to have lethargy and muscle spasm shortly before admission. Upon admission, she further deteriorated to the comatose state with a GCS score of 3/15, a pulse rate of 160 bpm, 99% oxygen saturation and a temperature of 38°C. Physical examination revealed dehydrated state, clear lungs to auscultation, non-tender abdomen and generalised muscle spasm despite the presence of spontaneous movements. Endotracheal intubation was performed for ventilatory support in comatose state. Blood tests revealed 6.76 mmol/L phosphate, 0.96 mmol/L total calcium, 0.47 mmol/L ionised calcium, 150 mmol/L sodium, 2.2 mmol/L potassium, 0.63 mmol/L magnesium, 101 mmol/L chloride, pH 7.31, 14 mmol/L bicarbonate, 50 µmol/L creatinine and 5.2 mmol/L glucose. Computed tomography of the brain was unremarkable. Electroencephalogram (EEG) did not detect epileptiform discharge. Further history was taken that she had been given a half tube of a rectal enema solution (133 mL per tube) twice uneventfully according to the prescription dose in the past. However, a three-fourth tube of the enema solution was administered this time, around 1 h before generalised muscle spasm was observed. Her impaired conscious level and muscle spasm fully recovered after the correction of severe hypocalcaemia and other electrolyte imbalances within 48 h. She was discharged on day 6 without long-term sequelae.
Each 133-mL bottle of the involved enema solution contains 19 g of monobasic sodium phosphate and 7 g of dibasic sodium phosphate. It functions as an osmotic laxative used for the treatment of constipation. It has been reported to induce significant toxicity or even fatality in susceptible groups including children, the elderly and patients with renal failure and impaired gut motility.13,14 Systemic toxicity may occur as early as 15 min after the administration of a single dose. The electrolyte disturbances related to toxicity are hyperphosphataemia, hypocalcaemia, hypernatremia, hypomagnesaemia and metabolic acidosis. The clinical features of electrolyte disturbances are dizziness, tachypnoea, convulsions, tetany, coma, tachycardia or bradycardia, hypotension and QT prolongation secondary to hypocalcaemia or hypokalaemia.14,15 The management is mainly supportive measures to ensure adequate hydration and to correct electrolyte disturbances, especially hypocalcaemia. Haemodialysis or haemofiltration may be considered in severe conditions. According to this case and case reports from the literature, sodium phosphate–based rectal enema solution should be used with caution, especially in susceptible patients of developing toxicity from sodium phosphate.
Cases 5–8
Four young adults, all in their 20s, presented with convulsion and hyperthermia while participating in an outdoor electronic music festival on 16 September 2017. The first case presented to AED at about 3 pm, with convulsion for 5 min and a body temperature of 42.9°C. The patient was intubated and put on CritiCool® system for rapid cooling in AED. The body temperature was brought down to 37.6°C within 40 min. The patient developed multi-organ failure and required extracorporeal membrane oxygenation (ECMO) support and renal replacement therapy (RRT) in intensive care unit (ICU). The patient survived after 7 weeks of ICU stay and months of rehabilitation.
The second case was brought to an AED at about 9 pm on the same day. On arrival, the patient was comatose after reported convulsion, with a body temperature of 42°C, a blood pressure of 52/28 mmHg and a pulse of 166 bpm. The patient developed ventricular fibrillation and cardiac arrest a few minutes later. After an hour of active resuscitation, death was certified for this patient in AED. The third case arrived at the same AED while the second case was resuscitating. The patient convulsed for 2 min and the body temperature was 42°C. The patient was intubated and put on CritiCool system for rapid cooling in AED. The body temperature was brought down to 40.2°C in 35 min. This patient developed less severe multi-organ failure compared with the first case, requiring RRT and 10 days of ICU stay. The fourth case presented to AED around midnight, with convulsion for 30 min and a body temperature of 41.9°C. The patient was intubated and put on conventional external cooling measures (i.e. applying ice packs, water spraying and fanning) in AED. The body temperature was brought down to 39°C in 1 h. This patient survived after 4 days of ICU stay.
Methylenedioxymethamphetamine (MDMA) was detected in the urine samples of all cases. Use of Ecstasy (street name of MDMA) during the music festival was reported by the patients or their friends. MDMA is an amphetamine-like stimulant with potent serotoninergic effect. The resurgence of MDMA-related death was reported in Europe and the United States in recent years. Deaths have been reported after single MDMA pill use. Patients with severe MDMA toxicity may present with hyperthermia, convulsion, intracranial haemorrhage, dysrhythmias, rhabdomyolysis, disseminated intravascular coagulation and hyponatraemia. Management is mainly supportive with rapid cooling measures to lower the core temperature in patients with hyperthermia. Serotonin syndrome was observed in all survival cases in this cluster and cyproheptadine, an anti-serotoninergic drug, was used during initial management.
Cases 9–13
Five cases of aconite poisoning after treatment from five different Hospital Authority Tripartite Chinese Medicine Centres for Training and Research (HACMCTR) happened over a 4-month period from the end of 2016 to January 2017. All of them were dispensed with normal doses of processed Radix Aconiti Lateralis (製附子). Three of the patients had mild symptoms with perioral and limb numbness only, while the other two developed bradycardia and hypotension requiring ICU care. All patients recovered after treatment. The Department of Health (DH) and HA were alarmed of the clustering. The batch of herb was promptly recalled from all HACMCTR and no more case of aconite poisoning after treatment from HACMCTR was recorded in 2017.
Processed Radix Aconiti Lateralis is a Chinese herb made from highly toxic aconite rootstocks with a recommended dose of less than 15 g by the Chinese Pharmacopoeia. Pre-boiling of the herb for 1–2 h is required to detoxify the toxic alkaloids before consumption. Symptoms usually occur within 30 min to 4 h after taking the decoction that manifest as gastrointestinal upset, perioral and limb numbness, weakness, bradycardia with different levels of heart blockage, hypotension and ventricular arrhythmia. It is the commonest acute herb poisoning in Hong Kong and is potentially lethal. Depending on the clinical situation, intravenous fluid, inotropes, atropine and antiarrhythmic agents may be required for treatment.
A cluster of deschloro-N-ethylnorketamine poisoning
Since October 2017, HKPIC has recorded more than 15 cases of deschloro-N-ethylnorketamine (2-oxo-PCE; also deschloro-N-ethylketamine) poisoning. They presented separately to various AEDs in Hong Kong. They were sent to AEDs because of varying degrees of altered mental status from drowsiness to agitated delirium of prolonged duration. Most patients reported an unfamiliar experience (e.g. intense rush sensation) after using the substances that were sold as ketamine. Typical clinical presentations of ketamine insufflation, such as the presence of white powder in nostrils, and collateral history of ketamine usage were noted. Hypertension, tachycardia and fever were also observed in some patients. They were all treated with supportive measures. In some cases, physical restraint and repeated doses of intravenous sedation were required. Bedside urine immunoassay tests for ketamine were performed in some of these cases and were found to be negative. Laboratory analysis of the urine specimens of all these cases detected the presence of 2-oxo-PCE. 16
2-oxo-PCE, a psychoactive substance, has emerged clinically in Hong Kong since October 2017. Toxicological information of 2-oxo-PCE is limited in the literature. The chemical structure of 2-oxo-PCE is closely related to ketamine, and it was used as a ketamine substitute. Like other phencyclidine derivatives, it produces the dissociative effects through N-methyl-D-aspartate (NMDA) receptor antagonism. Toxicity was similar to that of ketamine but considerably more potent, resulting in the higher incidence of intoxication and emergence delirium. Patients with 2-oxo-PCE intoxication may present with clinical features resembling stimulant toxicity, including agitation, confusion, seizures, loss of consciousness, hypertension, tachycardia, fever, rhabdomyolysis and transient ischaemic attacks. Furthermore, chronic toxicity of 2-oxo-PCE, as noted in ketamine abuser, remains unknown at this moment. Bedside urine immunoassays for ketamine were negative in cases with solely 2-oxo-PCE exposure. Laboratory analysis of the urine specimens of the suspected cases would be helpful in detecting the presence of 2-oxo-PCE.
Based on the experience from this cluster, if patients purported ketamine use and presented with ketamine-like toxidrome, more agitated delirium and features of stimulant toxicity, together with negative bedside urine immunoassay for ketamine, the 2-oxo-PCE exposure should be considered.
Footnotes
Acknowledgements
We certify that we have each made substantial contribution so as to qualify for authorship and that we have approved the contents.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Since this is an annual report with no patient contact and intervention involved, written informed consent was considered not necessary by our centre and no patient identifiable data have been included in the manuscript. Our previous annual reports were also published in this journal without informed consent.
Ethical approval
Our centre considered ethical approval not necessary as the study involved no patient identifier and intervention. Information used in this study was considered as part of the usual clinical data obtained by our institute and was passed to the researchers in a fully anonymised format. Our previous annual reports were also published in this journal without the need for ethical approval.
Human rights
Patient’s right was not infringed in this study.