
Abstract
Objective:
To report and analyse the poisoning data of Hong Kong Poison Information Centre in 2016.
Methods:
In 2016, all poisoning cases received by Hong Kong Poison Information Centre were retrieved from its database (Poison Information and Clinical Management System) for analysis.
Results:
A total of 4096 poisoned cases were analysed. There were 1871 male patients (45.7%), 2203 female patients (53.8%) and 22 sex unspecified patients (0.5%). The majority of the cases (63.1%) were between 20 and 59 years old. Common causes for poisoning were suspected self-harm/suicidal attempt (36.3%), unintentional exposure (18.4%) and abusive use (13.1%). Excluding the common co-ingestant ethanol, the five commonest types of poisons were benzodiazepines, paracetamol, household products, zopiclone and Chinese herbal medicine. Most patients were managed with supportive measures, while 14.3% and 12.9% of them were treated by decontamination and antidotes, respectively. Majority of the cases had uneventful recovery; 1% resulted in death and 3.9% had major outcomes. Six interesting cases and three poisoning outbreaks were discussed.
Conclusion:
This 11th annual report provided the updated epidemiological information on poisoning pattern in Hong Kong and highlighted important changes in comparing with our previous reports.
Keywords
Introduction
The Hong Kong Poison Information Centre (HKPIC) was established in 2005. Currently, it provides 24 h phone consultation service to health care professionals in Hong Kong for poison information and clinical management advice on poisoning. It also provides onsite clinical toxicology service to poisoned patients in United Christian Hospital where it is located. HKPIC also collects important poisoning epidemiological data in Hong Kong from voluntary poisoning reporting in Hospital Authority (HA). It also continues to organize regular training activities such as monthly seminar, basic clinical toxicology course, certificate course and the 1-year quotable diploma course in clinical toxicology (Dip Clin Tox (HKCEM and HKPIC)) in conjunction with the Hong Kong College of Emergency Medicine (HKCEM), as well as training for overseas doctors. Clinical toxicology is a recognized medical speciality in Hong Kong since 2016. HKPIC is currently the accredited poison centre for the fellowship training of clinical toxicology under HKCEM. In the area of research, HKPIC published 6 articles in peer-reviewed journal in 2016, adding up to a total of 95 since its establishment. The mission of the HKPIC is to minimize the mortality and morbidity of poisoning by the provision of high-quality clinical toxicology service and to become one of the leading toxicology training centres in Asia-pacific region.
HKPIC has started to publish its annual reports since 2006. It continues to provide the updated information in poisoning epidemiology and its changing trend in Hong Kong. This 11th annual report of HKPIC covers the data in 2016, and as in the previous reports to focus on the latest poisoning pattern and highlight some important poisoning cases in Hong Kong.
Methods
The HKPIC received its poisoning cases from two major sources: consultation and reporting. Consultation is defined as poisoning case health care professional consulted us for the poison information and management advice while reporting is defined as the poisoning case reported in HA, majority by all accident and emergency department (AED). In 2016, all poisoning cases received by HKPIC were retrieved from its database (Poison Information and Clinical Management System (PICMS)) for analysis.
The data of each poisoning case was inputted into PICMS according to information obtained from the consulting health care professional, medial record, electronic patient record (ePR) of HA and other relevant sources. Data collected included patient demographic data, poison data (poison type and dose, route, time, place and reason of exposure), clinical data (clinical features, investigations results), management data (use of decontamination, antidotes and other specific treatment) and outcome data (disposal for AED patient, final outcome and its relationship to the poison exposure) for consultation cases, while only patient demographic data, poison data and outcome data were inputted for the reporting cases.
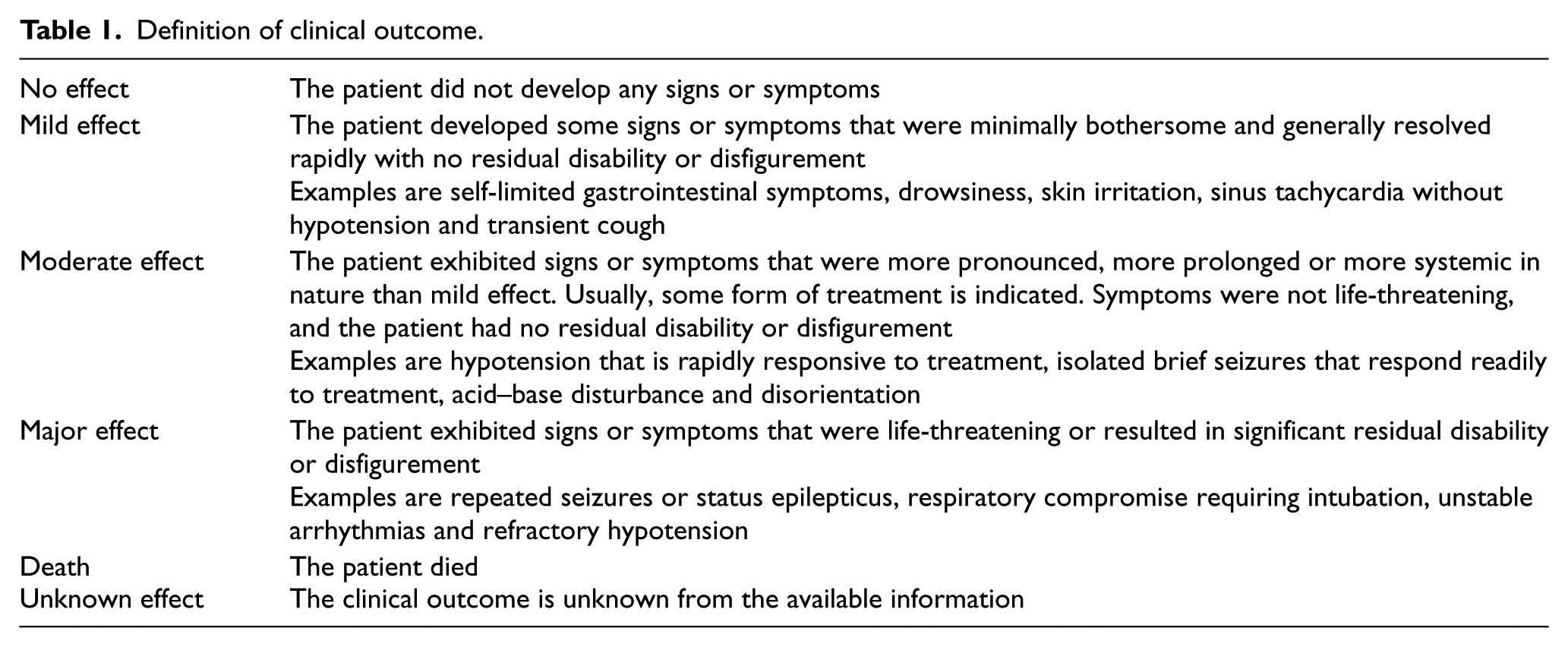
Senior doctors from the HKPIC would classify the outcome of the cases into five categories: no effect, mild effect, moderate effect, major effect or death with reference to the American Association of Poison Control Centers’ National Poison Data System 1 (Table 1). Besides, the relationship between the poison exposure and clinical outcome was graded as definite, probable, possible, not related or undetermined/not applicable according to the available information. All death or major effect cases were further reviewed by a second senior to ensure the grading is appropriate.
Definition of clinical outcome.
Results
After excluding duplicate and invalid cases, the PICMS generated 4096 (100%) valid cases, including 2183 (53.3%) consultation cases and 1913 (46.7%) reporting cases for analysis in the year 2016.
The age and gender distribution of the cases are shown in Figure 1. There were 1871 male patients (45.7%), 2203 female patients (53.8%) and 22 sex unspecified patients (0.5%). A female predominance was noted in majority of the age groups except for the children of age 0–12 years and for elderly from age 60 to 79. Concerning the age distribution, the middle-aged group (age, 30–39) was the commonest and the majority (63.1%) of them was between 20 and 59 years old. Around 10% of the cases were children from the age 0 to 5 years old.
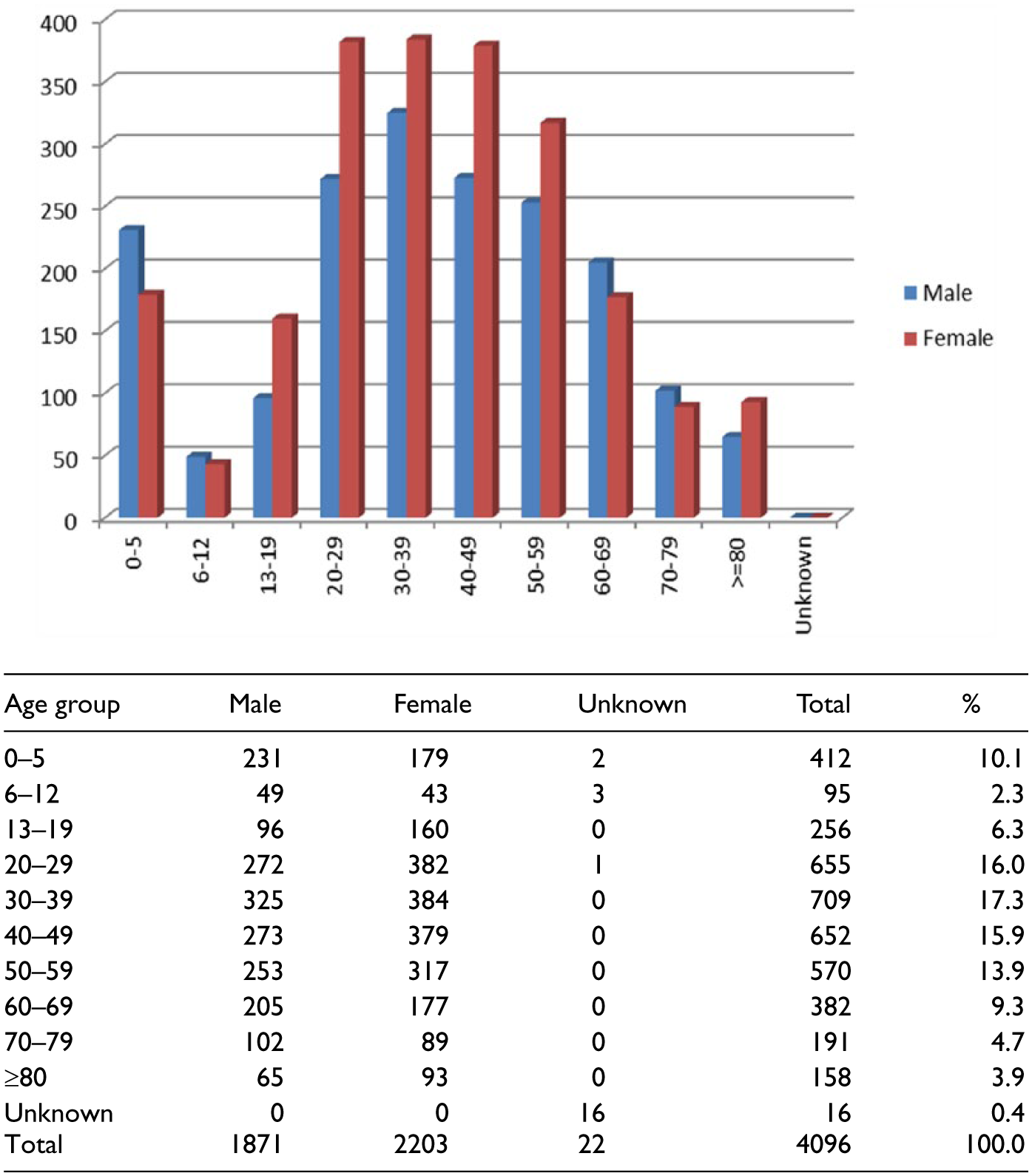
Age and gender distribution.
The reasons for poisoning are listed in Figure 2. The commonest cause was suspected self-harm/suicidal attempt which accounted for 36.3% of the cases. Poisoning due to unintentional exposure (18.4%) and abusive use (13.1%) had ranked the second and third commonest cause, respectively. Together with venomous bites and stings (10.1%) and adverse reactions secondary to herbal or proprietary Chinese medicine (7.7%), these five commonest reasons for poisoning contributed to the vast majority (85.6%) of the cases. As shown in Figures 3 and 4, commonest place of exposure was in the patient’s residential place (59.4%). The commonest route of poisoning was oral exposure (80.4%), followed by dermal exposure (8.4%) and inhalation (6.8%).
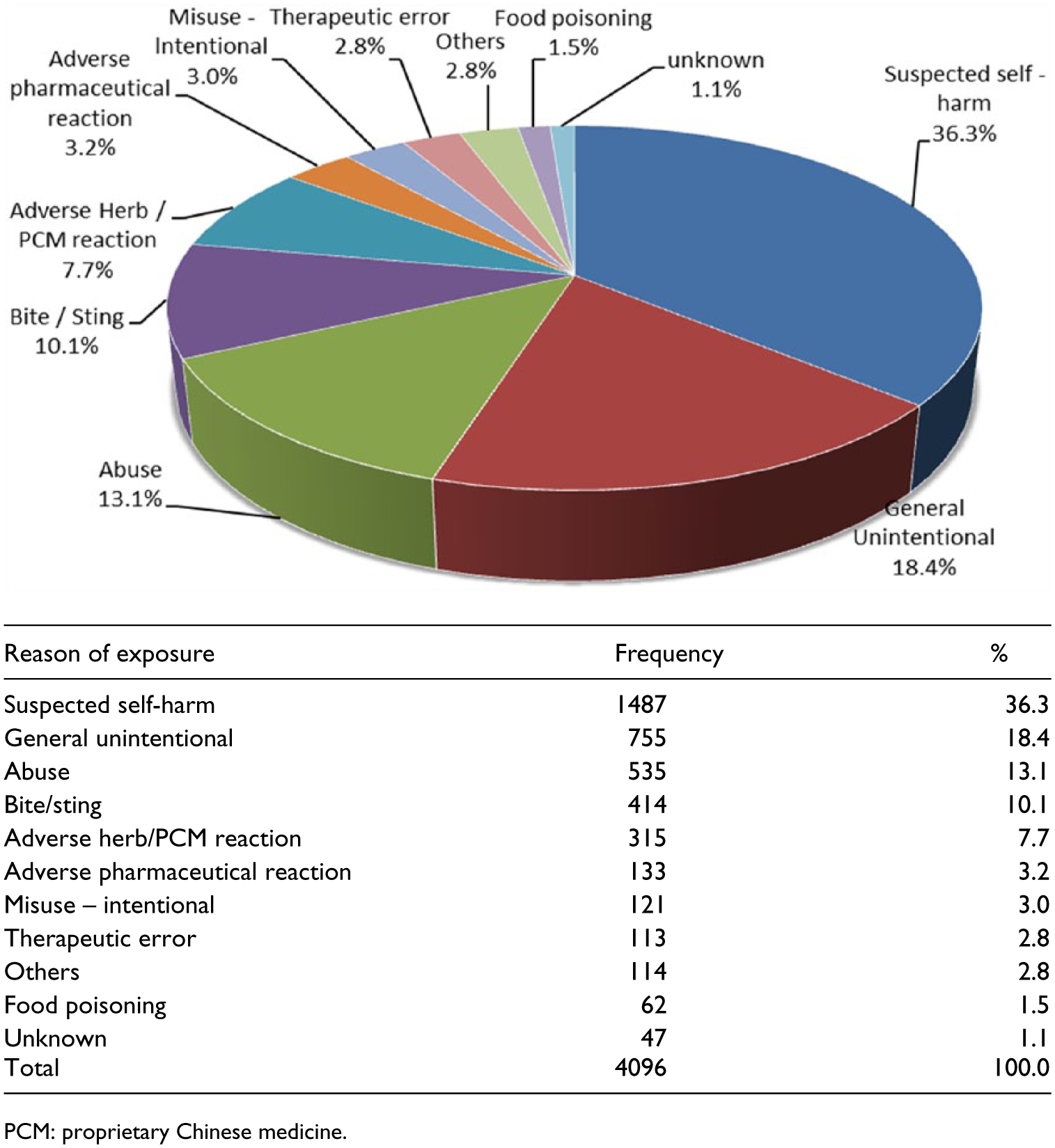
Reason of exposure.
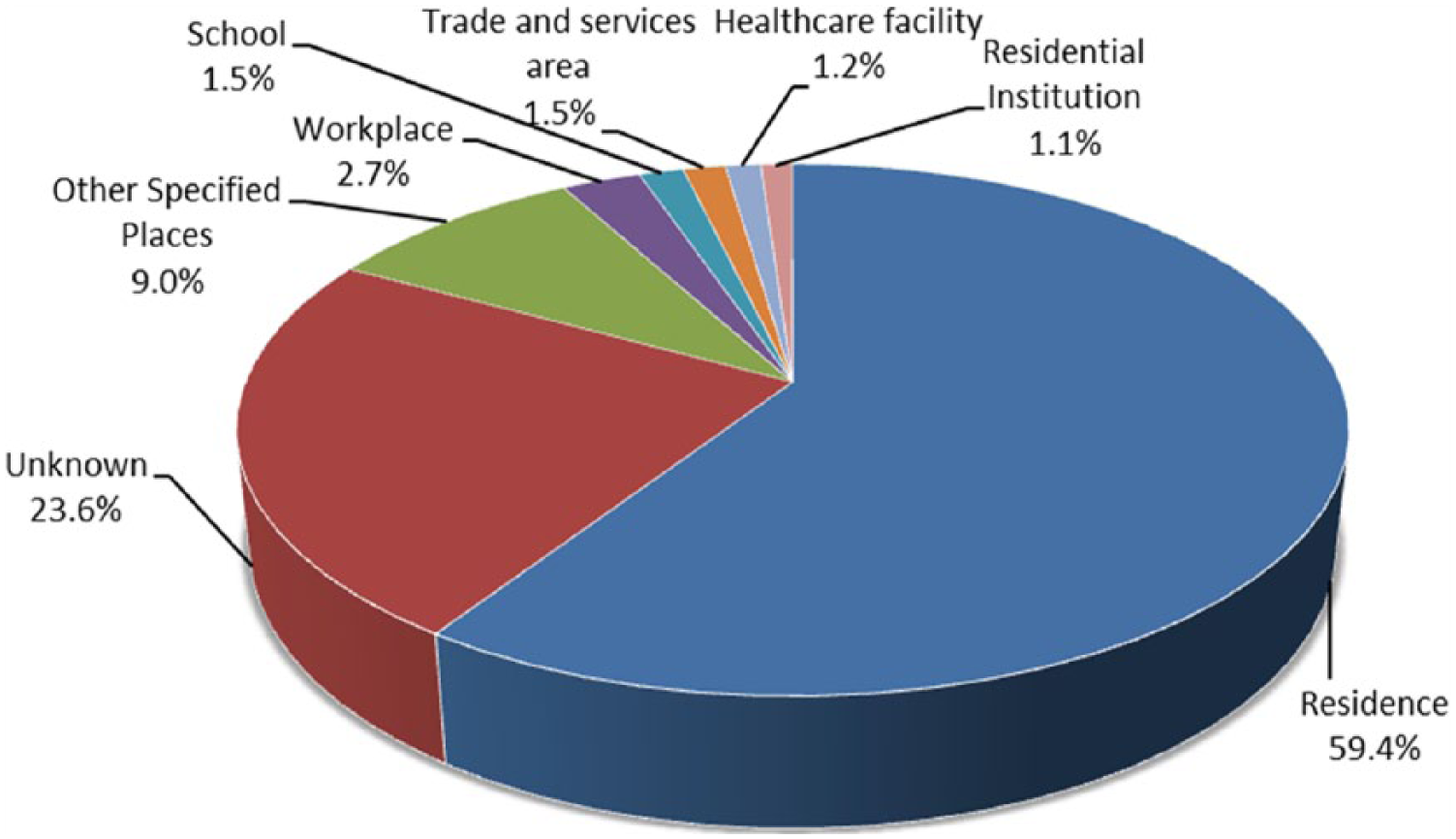
Place of exposure.
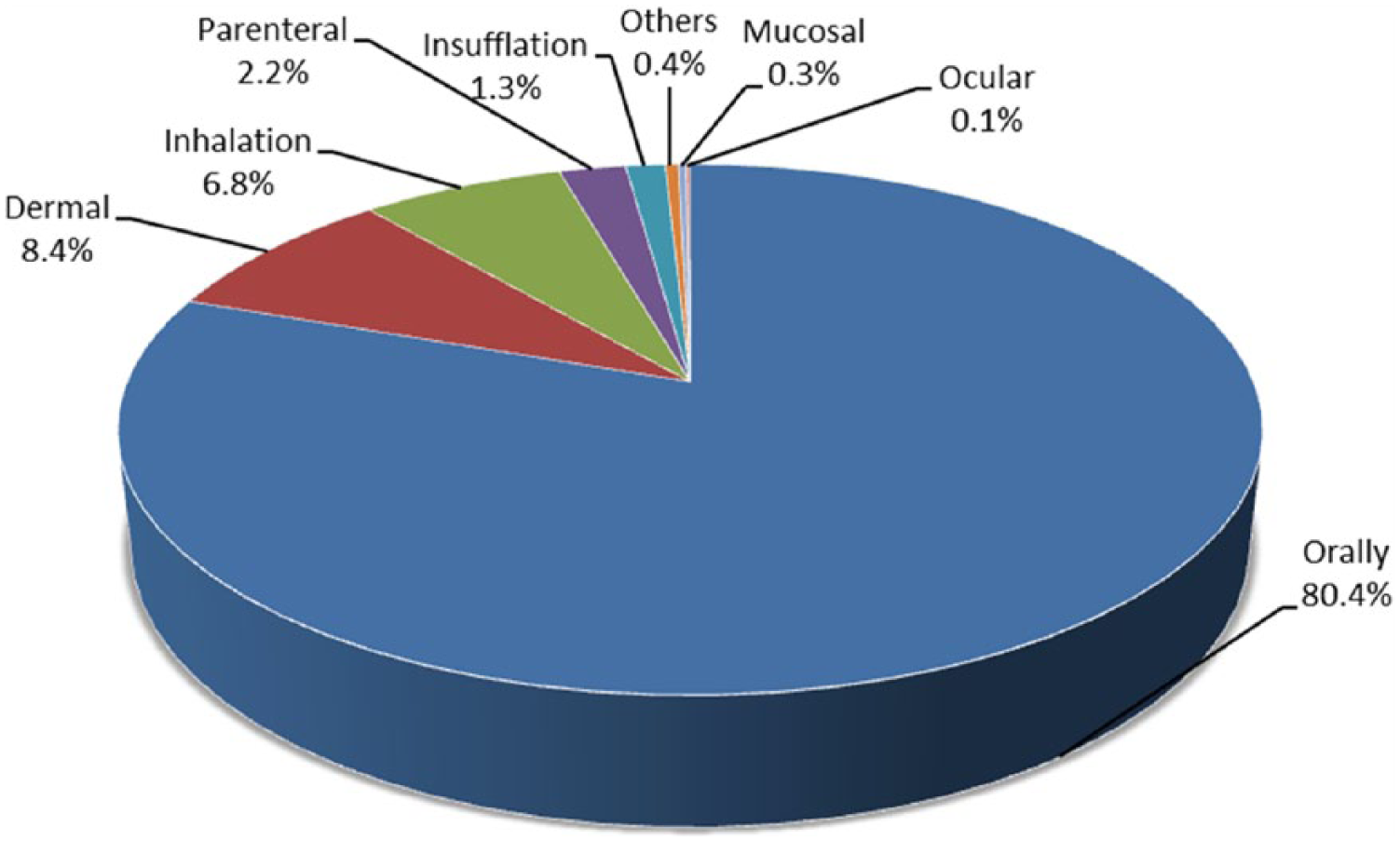
Route of exposure.
A total of 6055 poison exposures were recorded in the 4096 cases. About three-quarters of the cases (73.2%) had exposed to a single poison while the remaining (26.8%) of the cases had exposed to multiple poisons. Types of poison exposed are shown in Figure 5. Apart from ethanol which was commonly involved as co-ingestant, the five commonest types of poisons were benzodiazepine (361 cases), paracetamol (334 cases), household products (322 cases), zopiclone (272 cases) and Chinese herbal medicine (260 cases).
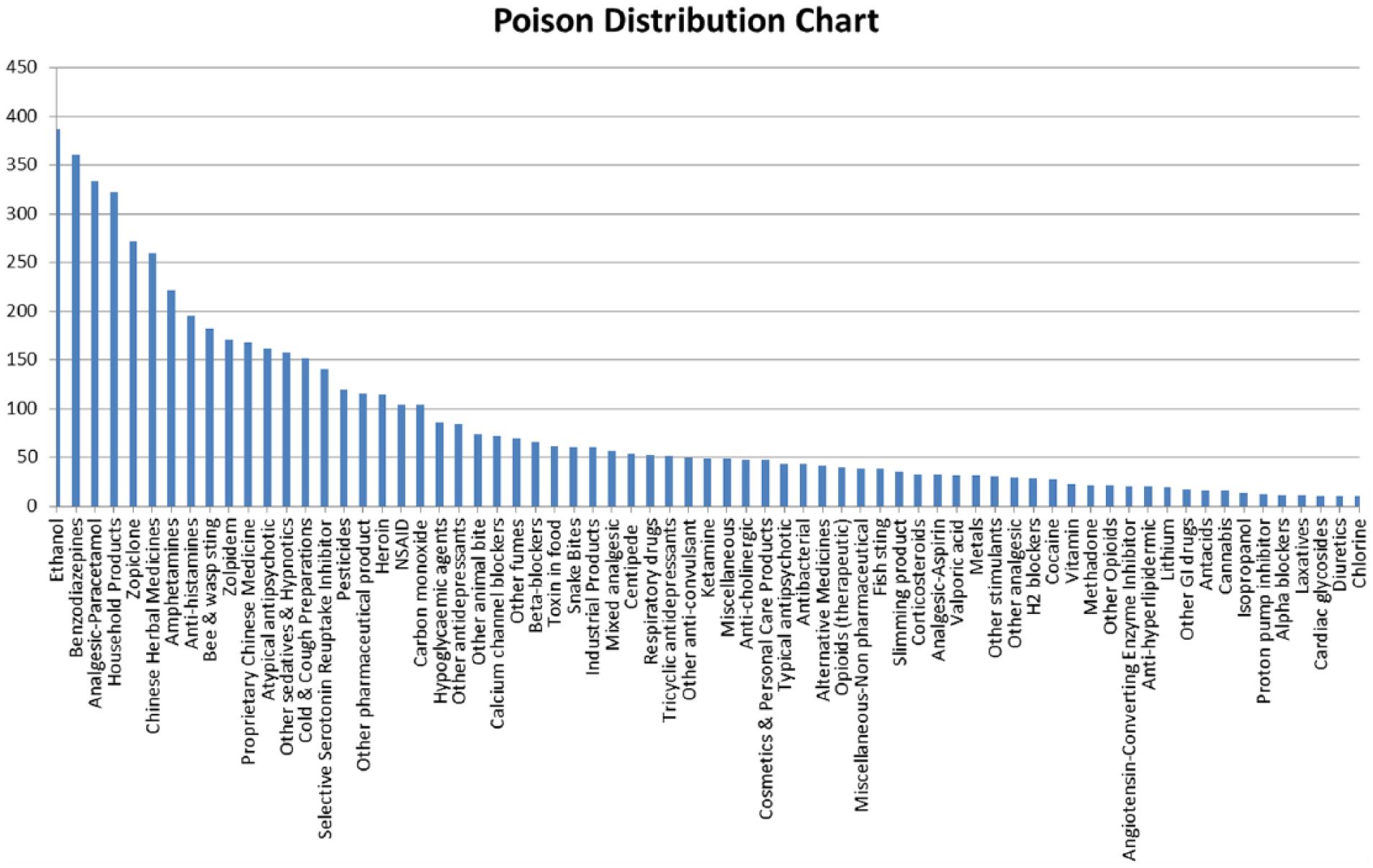
Type of poison exposed.
For the analysis on the management concerning decontamination and antidotes use, only the consultation cases were included. For the 2183 (100%) consultation cases, 312 (14.3%) patients underwent decontamination and 27 of them were given multiple decontamination methods, the commonest method was single-dose activated charcoal (AC; 80.9%), followed by gastric lavage (7.0%) and multiple doses of AC (6.2%) as shown in Table 2. Regarding the antidotes use, 281 (12.9%) patients were treated with antidotes and 39 of them were given more than one antidote. The five commonest used antidotes were N-acetylcysteine (NAC), naloxone, benzodiazepines, antivenom and calcium as listed in Table 3.
Decontamination.
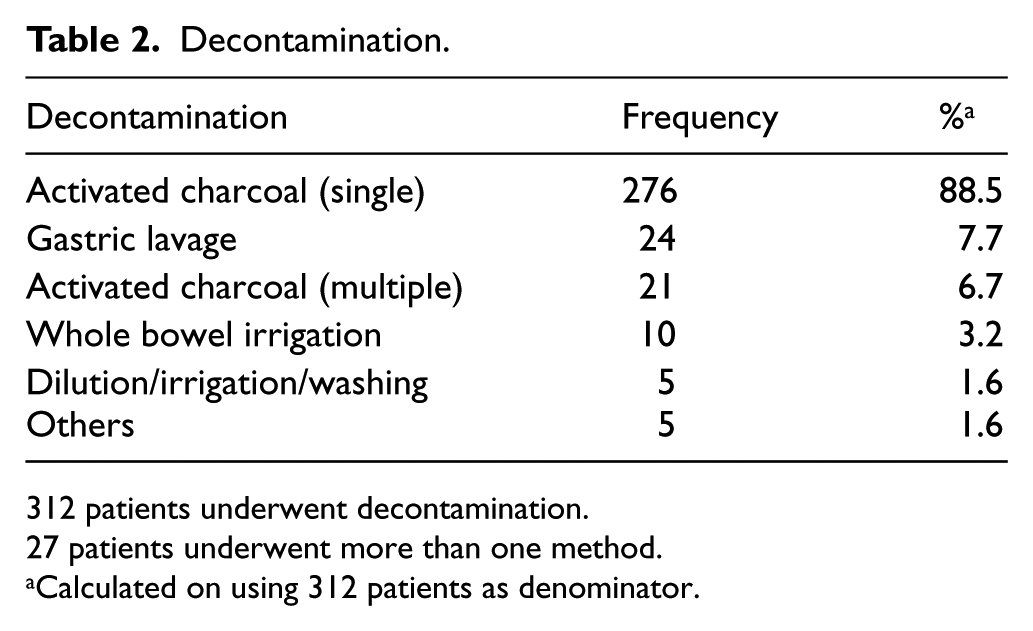
312 patients underwent decontamination.
27 patients underwent more than one method.
Calculated on using 312 patients as denominator.
Antidote.
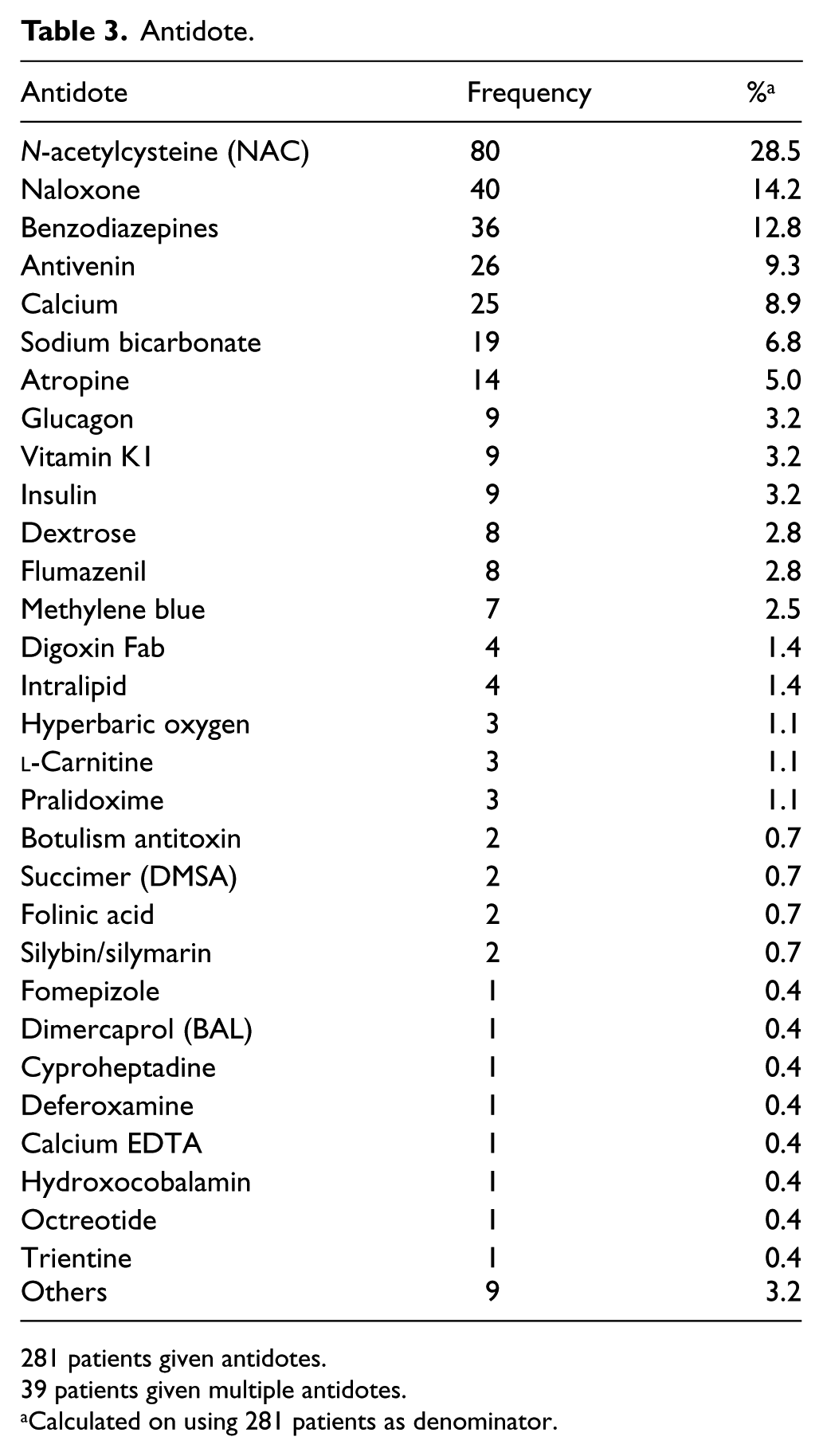
281 patients given antidotes.
39 patients given multiple antidotes.
Calculated on using 281 patients as denominator.
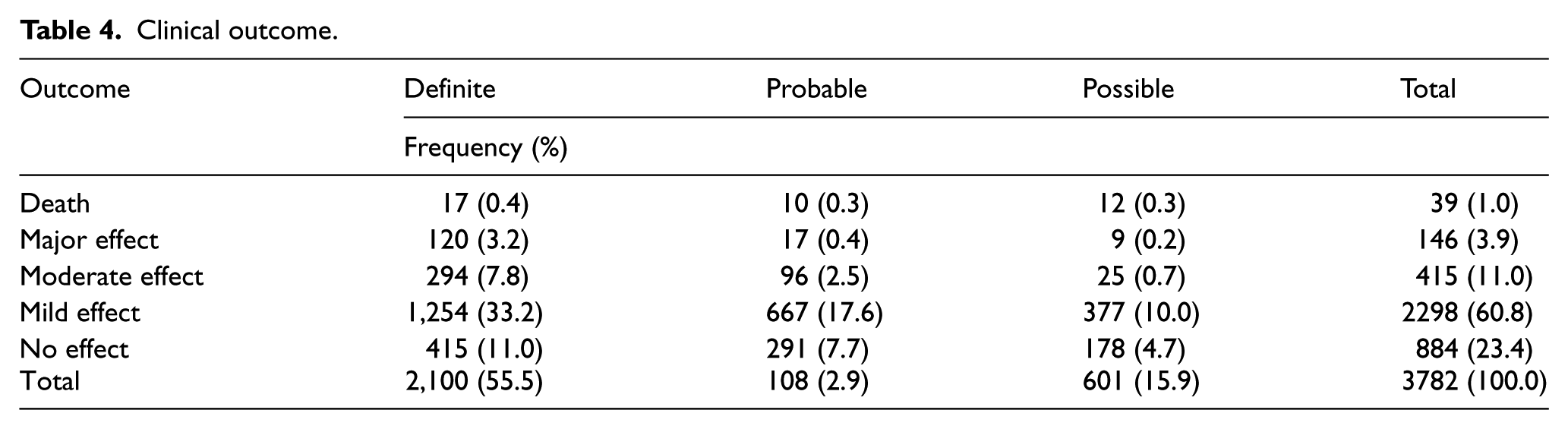
After excluding 314 cases in which the clinical outcomes were graded as not related to the poison exposure or clinical outcome cannot be assessed from the available information, the remaining 3782 cases (100%) were analysed for the outcome. There were 39 deaths (1.0%), 146 cases of major effects (3.9%), 415 cases of moderate effects (11.0%), 2298 cases of mild effects (60.7%) and 884 cases of no effect (23.4%), as shown in Table 4. From another point of view, 55.5%, 28.6% and 15.9% of the outcomes were graded as definitely, probably and possibly related to the poison exposure, respectively.
Clinical outcome.
In 2016, we have received 251 consultations on pre-hospital AC administration. Among these 251 patients, 152 (60.6%) patients were given AC by ambulance paramedics. The remaining 99 (39.4%) patients were either not indicated for AC administration or AC administration was judged to be not feasible during the ambulance transfer.
Discussion
This 11th annual report of HKPIC analysed the data of more than 4000 poisoned cases in 2016 which represented the updated poisoning pattern in Hong Kong.
HKPIC recorded 4096 cases in 2016 which increased 3.4% compared with that in the previous year. The increase in number of poisoning cases was primarily from our reporting service while the cases in the consultation remained similar. 2 Whether the increase in the reporting cases is due to the increased utilization of reporting system or a true increased incidence of the poisoning cases in Hong Kong needs further monitoring.
Poisoning reporting is not compulsory and remains as one of the intrinsic limitations in our data that is common to the poisoning databases in most developed countries. Nevertheless, we still record over 4000 cases in this report, and we believe that we have captured the majority of poisoning cases for analysis.
The age and gender distribution and routes of exposure were comparable with our previous reports and overseas data.1,2 The three commonest reasons of exposure, namely suspected self-harm, unintentional exposure and substance abuse, remained the same as in previous year. Five commonest types of poison exposed were benzodiazepines, paracetamol, household products, zopiclone and Chinese herbal medicine. In this year, benzodiazepines outnumbered the others and became the commonest exposed poison.
Over the past 5 years (2012–2016), benzodiazepine and paracetamol exposure ranked both first and second commonest poison and each was involved in an average of 9% of our poisoning cases. Benzodiazepine and zopiclone poisoning commonly occur in intentional self-harm and abusive substances poisoning, as a sole poison or co-poison in multiple poisons exposure. Household products are commonly encountered in intentional overdose in adults as well as accidental exposure in children. Antiseptics, bleaches and cleansing agents were three commonest poisons involved in household products. For Chinese herbal medicine, the commonest acute poisoning remained as aconite poisoning from the data in 2016.
In this year, the proportion of our consultation cases treated with decontamination (14.3%) and antidotes (12.9%) were both lower than the average of 14.7% and 13.4%, respectively, in the previous 5 years. Concerning the method of decontamination, the use of single-dose AC remained the commonest method as expected from our local experience and overseas poison centre data.1,2 Before 2016, there was a continuous increasing trend in the proportion of poisoning cases being treated with antidotes over the past few years, reaching a peak at 16.2% in 2015. The reason for the observed decrease in the decontamination and antidotes rate needs further monitoring.
NAC, naloxone and benzodiazepines were the commonest used antidotes. NAC was given in one-fourth of paracetamol poisoning cases. It may also be used to treat other poisonings such as amatoxin and paraquat with limited evidence. Naloxone, benzodiazepine and antivenin use were similar and together accounted for about 30% of the antidote use. Calcium ranked fifth mostly used antidote. Interestingly, the use of calcium increased abruptly from 3.5% in 2015 to 8.9% in 2016 that was higher than the average of 5.9% in the last 5 years. A possible explanation for this change can be the increasing awareness of calcium as the established antidote for calcium channel blocker–induced hypotension or other poison such as hydrofluoric acid. Notably, there was a use of botulism antitoxin for two patients in 2016, due to an outbreak of iatrogenic botulism as discussed in interesting cases section below.
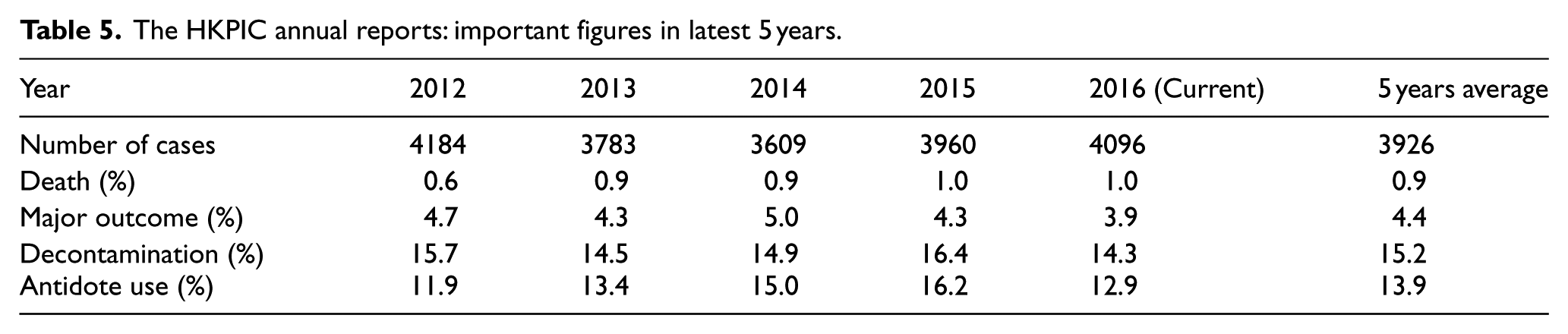
Concerning the clinical outcome, the poisoning death rate in 2016 was 1.0%, which is similar to the average in the past 5 years (Table 5). The proportion of major effect was 3.9% and remained comparable in recent years with an average of 4.3%. On the other hand, majority of cases (84.1%) were classified as no effect or mild effect, which again was similar to our data in the recent years.
The HKPIC annual reports: important figures in latest 5 years.
There are limitations of this report as mentioned in our previous annual reports. First of all, reporting of poisoning cases in Hong Kong is on voluntary basis. Second, data obtained from the consulting medical professions may not be comprehensive. However, as most poisoning cases were managed in HA hospitals with the patient clinical records accessible by ePR, the accuracy and amount of information was expected to be much better than data obtained from other poison centres which may not have direct access to the patient records in their managing hospitals. Third, in some of the cases with limited clinical information, it is difficult to make definite judgement on the causal relationship between the outcome and the poison exposure.
Conclusion
This 11th annual report provides the updated epidemiological information on poisoning in Hong Kong in 2016 and highlights some changes in comparing with our previous reports. The pattern of the poisoning is similar over the past years. Concerning outcome, 1.0% and 3.9% of the cases resulted in death and major outcome, respectively. HKPIC will continue to monitor the poisoning pattern in Hong Kong to facilitate the formulation of strategies in poison control and prevention.
Interesting cases
Case 1
A mentally subnormal patient in their twenties was admitted after drinking 500 mL of an alcohol-based handrub, which was labelled to contain 75% isopropyl alcohol. The patient was in coma and hypotensive requiring intubation and inotropic support. Serum methanol screening was positive, and the serum methanol level was subsequently confirmed to be 72 mmol/L while isopropyl alcohol level was 55.9 mmol/L. The patient was treated with intravenous ethanol and continuous veno-venous haemofiltration (CVVH). Chemical analysis of the handrub detected 22% methanol, 36% isopropyl alcohol and 3.5% ethanol. The unexpected finding of the high concentration of methanol in this handrub was reported to the Department of Health (DH) for further investigation.
The World Health Organization 3 recommended either 80% ethanol or 75% isopropyl alcohol as the main ingredients of alcohol-based handrub. In ethanol and isopropyl alcohol poisoning, inebriation, hypotension, hypoglycaemia (for ethanol poisoning) and ketosis without acidosis (for isopropyl alcohol poisoning) may also occur. Treatment is mainly supportive. Rarely, haemodialysis may be required in life-threatening poisoning such as intractable hypotension. Methanol poisoning, on the other hand, can lead to severe metabolic acidosis, blindness, cerebral necrosis with or without haemorrhage that typically involves the putamen and death. The ‘block and wash’ approach by intravenous ethanol or fomepizole that blocks the metabolic conversion of methanol to formate and enhanced elimination by haemodialysis or haemofiltration is the mainstay of treatment in methanol poisoning.
This case alarmingly revealed that undeclared methanol can be found in alcohol-based handrub in Hong Kong. In fact, two deaths caused by ingestion of hand sanitizer containing undeclared methanol have been reported in Canada in 2013. 4 Urgent testing for blood methanol may be indicated in selected patients who have taken alcohol-based handrub. The use of methanol-containing handrub also has health concern as visual damage have been reported after long-term dermal and inhalational exposure to methanol.
Case 2
A patient in their 60s from South Asia with history of diabetes mellitus (DM), renal impairment and hypothyroidism presented with abdominal pain, vomiting, diarrhoea and anaemia with haemoglobin level of 6.8 g/dL. They initially denied herbal medicine intake. Blood transfusion and extensive workup that included bone marrow examination, oesophagogastroduodenoscopy and colonoscopy had been performed for the patient. Blood lead level (BLL) was checked as the blood film showed heavy basophilic stippling. The patient was later readmitted for delirium and an episode of generalized convulsion. The BLL coincidentally came back to be 150.7 µg/dL. It emerged that the patient had been taking Ayurvedic medicine consisting of ‘herbal’ powder and pills obtained from India for her DM. Lead encephalopathy was diagnosed and chelation therapy was started with intramuscular dimercaprol (BAL) and intravenous calcium disodium ethylenediaminetetraacetic acid (Ca EDTA), followed by a course of oral succimer (DMSA). The patient’s general condition improved and the follow-up BLL at about 2 weeks and 1 month later dropped to 60 and 21 µg/dL, respectively. The ‘herbal’ powder was analysed to have a high lead concentration of 108,389 ppm (parts per million).
Acute lead encephalopathy is the most severe clinical form of lead poisoning. Before the advent of chelation, 65% of severe cases terminated fatally. 5 Obtundation, headache, seizure, confusion, cerebral oedema, papilloedema and death may occur in adult while apathy, vomiting, ataxia, incoordination, seizures, coma and cranial nerve palsy may occur in children. 6 In chronic poisoning, anaemia, peripheral neuropathy and abdominal pain are reported. Prompt administration of appropriate chelation, removal of the source and supportive measures are essential in treating patients with lead encephalopathy.
Ayurvedic medicine is used worldwide by the Indians and other South Asian diaspora. Lead, mercury, arsenic and other metals may be found in Ayurvedic medicine products. 7 Lead poisoning should be considered in patients who have used these products.
Case 3
A patient in their 50s man developed gastroenteritic symptoms 12 h after consumption of several wild mushrooms which were self-picked in Tai Mo Shan. The mushrooms were whitish in colour, with a sack-like covering at the base (Figure 6). The patient presented to AED at about 19 h post-ingestion with repeated vomiting, profuse watery diarrhoea and abdominal pain. HKPIC was consulted and amatoxin mushroom poisoning was suspected based on the clinical presentation. The patient was admitted to the intensive care unit (ICU) for management. Supportive treatment, silibinin, high-dose penicillin G, NAC, multiple dose AC and charcoal haemoperfusion were initiated. Urgent urine analysis performed by Hospital Authority Toxicology Reference Laboratory (HA TRL) was tested positive for alpha-amanitin. Subsequently, the mushroom sample was identified to be Amanita exitialis by expert mycologist. The patient’s liver function started to derange at 36 h post-ingestion, with alanine aminotransferase peaked at day 4. Deranged renal function was also apparent. The patient finally recovered without liver transplant and was discharged after 12 days of hospitalization. This was the fifth recorded case of Amanita poisoning after consuming wild mushroom collected within the territory of Hong Kong. 8

The mushroom was identified to be Amanita exitialis.
Case 4
A patient in their 30s was bitten by a spider in a swimming pool. She presented to an AED with local pain and swelling developed within 1 h after the bite. The patient’s vital signs were normal and other physical examination was unremarkable. The patients was treated with anti-histamine and antibiotic with rapid symptomatic improvement and was subsequently discharged a few hours later. Pictures of the spider were examined by biologists and culprit was judged to be a wolf spider.
There are more than 2300 species of wolf spiders in the biological family Lycosidae distributed worldwide. 9 Wolf spiders are commonly in brown or grey colours with a body size ranging from 15 to 30 mm. 10 They do not make web but hunt on ground like a wolf and hence the name. They are attracted to water and can swim for a short distance. A significant proportion of wolf spider bites happened while the victim was swimming or cleaning a pool. Despite being venomous, their bites are generally not life-threatening. Envenomation usually results in intense local pain, swelling, redness, itchiness and minor systemic upset include nausea, headache and malaise. Skin ulceration occurs rarely. Treatments are general wound care and symptomatic. Most bites should recover within 1–2 days. In Hong Kong, there are at least 36 native species of spiders and none possesses significant toxicity to human. 11
Case 5
A patient in their 30s found drowsy and confused was sent to hospital. On arrival to the AED, the patient was disorientated, with Glasgow Coma Scale of 9–10/15, blood pressure of 174/93 mmHg, pulse rate of 91 bpm and SpO2 of 96% on room air. The patient had poor respiratory effort that did not respond to 0.8 mg naloxone nor did their conscious state. The patient was treated with non-invasive-assisted ventilation initially but required endotracheal intubation and mechanical ventilation several hours later because of respiratory failure. The patient’s condition improved at 48 h after admission and was extubated. The patient admitted his suicidal attempt by overdosing himself with the dangerous drug carfentanyl that was bought over the Internet. The patient claimed that they had only used half of the total amount of 0.25 mg being bought. Subsequent testing on their urine sample by the HA TRL confirmed the presence of carfentanyl and its metabolite.
Carfentanyl is an extremely potent synthetic opioid with an analgesic potency estimated 10,000 times more than morphine. 12 It was used as an animal tranquillizer, typically being put inside firing darts for the sedation of big mammals like elephant. It has invaded the street drug market in North America as an undeclared substitute for other illicit opioids. An alarming outbreak of carfentanyl deaths since 2016 continues into 2017 and has been spreading to other parts of the world. In addition to carfentanyl, fentanyl and several other related substances are also increasingly found in street heroin and oxycodone. Conventional treatment for heroin overdose that typically use 0.4 mg or less naloxone plus a short period of supportive care is unlikely to be useful for the overdoses by drugs in the fentanyl family. A more aggressive regime starting with 2–5 mg naloxone bolus followed by infusion may be tried in patients with suspected overdose by fentanyl derivatives.
Case 6
A patient in their twenties presented with subacute onset of psychotic features temporally related to the use of a slimming product bought from overseas. Drug-induced psychosis was initially suspected. HA TRL analysed a sample with the same brand purchased in Hong Kong and detected an undeclared chemical, 2-diphenylmethylpyrrolidine (deoxy-D2PM). 13 The finding was reported to the DH and the product was recalled. 14
Desoxy-D2PM is a psychoactive substance, structurally similar to diphenylprolinol (D2PM) and desoxypipradrol (2-DPMP). It is sold as a designer drug and has been used in the manufacture of so-called legal highs. Reported features after its use include decreased appetite, agitation, hallucinations, mydriasis, hypertension and tachycardia. For D2PM and 2-DPMP, a review article indicates they have sympathomimetic properties similar to that of cocaine and, in addition, prolonged neuropsychiatric symptoms. 15
The patient was subsequently diagnosed to have limbic encephalitis, paraneoplastic syndrome and ovarian teratoma; after further investigations, it was judged that the deoxy-D2PM exposure was unlikely related to her clinical presentation. However, this case illustrated the collaboration of frontline clinicians, HKPIC, HA TRL and DH that bring about early detection against emerging poisons and swift poison control.
Outbreak 1
A total of 11 women presented with descending weakness to the AED of seven acute hospitals from May to August in 2016. They had received botulinum toxin injection to their faces, necks, calves or arms for beauty purpose in the mainland China at different occasions. The injections were not given by doctors, and all the procedures were not conducted in medical facilities. The patients developed progressive weakness in their head and neck region outside the injection sites within a few days. Typical symptoms included drooping eyelids, blurred vision, diplopia, facial weakness, difficult to keep their heads up, dysphonia and liquid food dysphagia. The more severe ones developed significant weakness in their limbs, difficulty breathing as well as generalized unwell feeling being described as flu-like. Clinically, they suffered from the toxic effect of botulinum toxin and were diagnosed iatrogenic botulism. A few of them who presented early among the cohort had underwent investigations for Guillain–Barre syndrome or myasthenia gravis. Electrodiagnostic studies on the condition can be non-specific. The diagnosis of iatrogenic botulism was made in one patient only when she disclosed the history of injection after she had been treated for myasthenia gravis for 6 months. Three patients who presented within the first week post-injection with significant weakness that impaired their swallowing, breathing and walking were treated with anti-botulinum antitoxin. After the antitoxin treatment, cessation of weakness progression was observed, but no objective power improvement could be documented in contrary to a report. 16 One patient developed serum sickness manifested as high fever and rash 1 week after the antitoxin treatment.
This outbreak of iatrogenic botulism also happened in Beijing, Shanghai, Shenzhen and other Chinese cities. 17 Sub-pharmaceutical graded black-market botulinum toxin with unstable toxin concentration was believed to be the cause. Poor injection technique might have also contributed to this epidemic. Botulinum toxin, although commonly used for cosmetic purpose, is factually the most toxic substance known to mankind. It can be lethal in the order of nanogram dose. Meticulous dilution and quality control are required in the manufacture of pharmaceutical-grade botulinum toxin. Black-market botulinum toxin carries a high risk of overdose in addition to obvious hygienic risk. Public should be warned against illicit botulinum toxin injection. Doctors should consider iatrogenic botulism as a differential diagnosis for acute onset descending weakness.
Outbreak 2
HKPIC provided consultation to AED on the case of an adolescent presented with headache, dizziness, nausea and shortness of breath shortly after exposure to an unknown smelly gas in classroom with windows opened. About 20 classmates in the same classroom were affected and attended the same AED. All patients had stable vital signs and improvement in symptoms after leaving the site. Hospital Authority Major Incident Control Centre (MICC) was activated by the incident. Police and Fire Service Department were involved. Two schools were evacuated in this incident, and a total of 70 patients were taken to three hospitals in Kowloon. 18 All cases received assessment and a brief observation in AEDs and were discharged with medical advice. Subsequently it was confirmed that the gas came from a chemical spill from a shipping container in nearby barge. The chemical was tetrahydrothiophene, which is used as on odorant. It is an organosulphur compound with intense smell. Accidental inhalational exposure can cause mild respiratory tract irritation. Management is mainly supportive and symptomatic.
Outbreak 3
In November 2016, HKPIC recorded a cluster of six cases of carbon monoxide (CO) poisoning happened in an indoor restaurant serving charcoal hotpot. They presented to three different hospitals and their ages ranged from 22 to 53 years old. Their symptoms appeared during the meal and persisted after leaving the venue. They complained of dizziness, headache, vomiting, palpitation and shortness of breath. Three of them suffered from transient loss of consciousness on scene, and one of them had urinary incontinence associated with her syncope. On presentation, they were all alert with stable vital signs and normal peripheral oxygen saturation. Some of them presented late, and with non-specific symptoms, the carboxyhaemoglobin (COHb) levels were measured as late as 5 h after the meal. Their COHb level ranged from 5.4% to 24.2% and they were all diagnosed as CO poisoning. Five patients were treated with normobaric oxygen therapy, while one patient received three sessions of hyperbaric oxygen therapy and were all discharged apparently well. At about 3 months post-incident, one patient was noted to have mild expressive dysphasia while one patient had memory deterioration on follow-up. This incident was immediately reported to the DH and Food and Environmental Hygiene Department for investigation.
CO is an odourless and colourless poisonous gas. Patients usually do not notice the poisoning themselves until it is too late. Clinically, most signs and symptoms of CO poisoning are non-specific. The existence of an indoor combustion source should be actively sought and COHb levels should be liberally tested in patients, particularly those with spatial clustering who presented with acute onset non-specific symptoms. Hotpot using charcoal burning in indoor environment may cause CO poisoning. This incident illustrated the risk of such dining practice. Health education and control measures should be taken to prevent this type of incident from recurring.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.