
Abstract
Introduction:
Cardiopulmonary resuscitation is a primary method used in the treatment of sudden cardiac arrest. It is a crucial skill that a healthcare provider and a lay rescuer should acquire to improve the survival and the neurological outcome of out-of-hospital cardiac arrest. Several modules were used to teach cardiopulmonary resuscitation for the healthcare provider and lay rescuer, but no module been developed that could be utilised in both population. Thus, this study aims to investigate the effectiveness of modified cardiopulmonary resuscitation training to knowledge (K), attitude (A), and performance (P) between medical and non-medical university students.
Methods:
This research was a single experimental study involving a total number of 125 students: 58 for a medical group and 67 for a non-medical group. A modified basic life support module, based on American Heart Association guideline 2015 was delivered to both groups under the same study setting. Pre and post KA scores were assessed using Res-Q questionnaire. The performance was evaluated by resuscitation feedback machine. The KA scores were analysed using repeated measure analysis of variance, and performance was examined using Pearson chi-square.
Results:
The study showed 64.8% of the participants were able to perform high-quality chest compression. Despite significant differences of sociodemographic background, there was no significant difference on effective chest compression between two groups (p = 0.200). There were also significant improvements in KA scores in both groups after intervention (p < 0.001).
Conclusion:
The knowledge of cardiopulmonary resuscitation can be delivered to everyone as aspired by our stakeholder to have one qualified cardiopulmonary resuscitation provider in a family. This modified basic life support module is reliably applicable to both healthcare and lay rescuer cardiopulmonary resuscitation training. All rescuers will perform in a similar manner, and this will tremendously reduce the discrepancy in the cardiopulmonary resuscitation qualities. Ultimately, this will improve an out-of-hospital return of spontaneous circulation rate.
Keywords
Introduction
A cardiac arrest is an abrupt cessation of the normal blood circulation due to a failure of the heart to contract efficiently during systole. 1 The incidence of out-of-hospital cardiac arrest (OHCA) in the world is within 20 to 140/10,000 populations, and survival ranges vary from 2% to 11%. 2 Early bystander chest compressions determine brain perfusion in cardiac arrest victim. It is of paramount importance for providers to familiarise themselves with this technique. In Malaysia, the frequency of bystander cardiopulmonary resuscitation (CPR) is widely unknown. A study in Hospital Universiti Sains Malaysia (HUSM) revealed only 8.7% OHCA received bystander CPR as compared to 33.3% worldwide. 3 Those who received CPR training were more likely to provide chest compression as compared to the non-training person. 4 Current evidence shows that OHCA outcome was poor.5,6 However, with bystander CPR, it will improve the survival outcome. 7 Early initiation and efficient bystander CPR significantly enhanced the survival and the neurologic outcome of OHCA.8,9
Knowledge needs to be accompanied by a right attitude and practice to produce an effective CPR. A local study showed that knowing CPR did not determine willingness towards performing bystander CPR among final year medical and dental students in HUSM. 10 In a developing country like India, awareness of basic life support (BLS) among healthcare workers was deplorable which needed improvement. 11 Surprisingly, developed countries also face a similar problem. A study among junior doctors in medical schools of United Kingdom revealed a low level of competency in carrying out adequate resuscitation even though the participants received a life support training. 12 Another study in New Zealand community found that CPR knowledge was poor, but they were inspired to learn more about CPR. 13
Meanwhile, in an Asian population, a study among the public in Hong Kong noted that only 12.0% of the respondents had received CPR training. CPR knowledge was poor even among the previously trained group. 14 In Singapore, a majority of respondents agreed CPR skill should be acquired, but only 31.4% respondents undergone the training. When dealing with an emergency, most of the respondents are willing to use their life-saving skill on family members or friends. 15
Traditionally, the focus on BLS modules was only tailored to the specific group of participants. For example, (1) adult CPR was taught to internal medicine and geriatric home care staffs, (2) child CPR for health care in paediatric department, (3) infant CPR for neonatal ward staff, and (4) ‘chest compression-only CPR’ for lay rescuer. There were no standardised modules that could apply to all groups of participants. In term of a training period, BLS training for healthcare rescuer consumed longer time compared to training for lay rescuer. No standardised period of training advocated and it was based on local preferences and target participants. BLS module for healthcare rescuer covered basic anatomy and physiology of CPR apart from the practical aspect whereby lay rescuer focused on hands-on aspect only. In terms of practical training, healthcare providers were trained on step-by-step approach of CPR that included airway, breathing, compression, and defibrillation, whereas CPR training for lay rescuer focused on effective chest compression only. The content delivery in a traditional BLS course was more towards pedagogical approach (teacher-centred approach). This method involved formal and authoritative climate; teachers were in control of planning and formulation of objectives. The assessment and progress were measured by the teachers, and they were produced as a subject-centred delivery of information. This method is not usually conducive to increase self-directed learning as the students depend on the teacher for all learning cues. These factors create a significant discrepancy of knowledge and skill between various groups of CPR providers.
The bystander CPR awareness can be increased with comprehensive training as proved by an interventional study conducted in Hong Kong community. The self-assessed confidence score for bystander significantly rose after CPR training. 16 Quality improvement of bystander CPR will improve the prognosis of OHCA. Therefore, there is a need to develop a standardised and comprehensive module in CPR training to educate individuals in both medical and non-medical background. Thus, this study aimed to evaluate the effectiveness of modified BLS module on knowledge, attitude, and performance towards CPR between the medical and non-medical students in public university.
Methodology
Study setting and population
The single experimental study was conducted between a period of July 2016 and Jan 2017 at Universiti Sultan Zainal Abidin (UniSZA), Kuala Terengganu, Malaysia. Consented university students from 10 faculties in UniSZA were randomly enrolled in this study. Participants were divided into two groups: medical group and non-medical group based on their formal educational background. The simple sampling method used in recruiting non-medical participants, while all year 4 medical students from Medical Faculty were automatically enrolled in the medical group. Non-medical participants were selected from nine faculties with different levels of educational background and no formal medical education. Participants were randomly selected from a list provided by a faculty academic office. In the beginning, 100 non-medical students were invited to participate in this study, but only 67 participants consented to enrolment. The BLS course is considered as a part of curriculum activity for the participants. All medical participants were year 4 medical students, who undergone 2 years of basic medical training and 2 years of clinical practice. This course is compulsory for year 4 medical students in UniSZA medical faculty.
Study tools
A self-administered structured questionnaire (Res-Q) was distributed in this study to assess the knowledge and attitude of both groups. The Res-Q consisted of three sections: (1) sociodemography, (2) knowledge of CPR and sudden cardiac arrest (SCA), and (3) attitude towards CPR. The sociodemographic items such as race, age, gender, course, current semester, faculty, academic qualification, and previous CPR and SCA experience were asked in the first section. In knowledge section, 25 statements on knowledge, which related to heart disease, risk factors for cardiac arrest, and CPR, were included. The maximum score on the knowledge domain was 125. The third section was on the attitude which consisted of seven statements. The highest score on the attitude domain was 35. This questionnaire had undergone construct validity and reliability in the previous validation study. The Cronbach’s alpha used in assessing internal consistency of Res-Q ranges from 0.435 to 0.871. The intraclass correlation coefficient (ICC) was used to determine the reliability of the ‘test–retest’ Res-Q, and the result is excellent. The process of validation and reliability is acceptable in developing Res-Q. 17 Permission from the author was established before data collection.
This study used Resuscitation Feedback Device (Zoll AED Pro®) to assess the quality and effectiveness of performing chest compression. The data were reviewed by RescueNet Code Review software. The criteria of high-quality chest compressions are (1) compression depth of 5–6 cm, (2) compression rate of 100–120 min−1, and (3) compressions in the target (CIT) of 60% or more collected using the device. CIT is generated when both compressions rate and depth fall into the correct range at the same time per unit of time. It objectively reflects the percentage of effective chest compression obtained per total compression. To date, there is no published data on the acceptable level of CIT for effective chest compression. Compression fraction (CF) is a measurement of the proportion of total resuscitation time that compression is performed. The chest CF was set as high as possible, with a target of at least 60% per American Heart Association (AHA) 2015 guideline recommendations. 18 For the purpose of this study, we set the target of CIT at least 60% as same as AHA 2015 recommendations for CF. Effective, high-quality chest compression declared if all the criteria were fulfilled. Before data collection, the machine undergone calibration process to ensure the validity and reliability of results.
Intervention module
The BLS module used in this study was a modified version of current BLS training module. This two-day module consisted of (1) short didactic lecture, (2) instructor-narrated video shows, (3) instructed practical and simulated case training, and (4) printed module developed by this research team based on AHA guidelines 2015.
A 30-min simplified lecture was given by an Emergency Physicians that included the prevalence of SCA locally and globally, introduction to cardiac arrest, risk factors, clinical features and complication of cardiac arrest, basic anatomy and physiology of CPR, and steps in CPR for adult and paediatric population. Followed by a 30-min video presentation on measures in performing CPR. This video developed by this research team was based on AHA guideline 2015. The video was presented in Malay and narrated by life support instructors. The participants were randomly divided into small groups of three to four people per mannequin. The mannequin used for hands-on training and case simulation. The steps of performing CPR and technique of delivering chest compressions were highly standardised and based AHA guideline 2015. Each group was supervised by certified instructors who underwent 1 day of refresher CPR course for standardisation setting. All participants experienced 4 h of guided intensive practical training in CPR. The printed modules such as BLS reference book 19 and the pamphlet were distributed 1 week prior this study began. The pamphlet focuses on step-by-step guideline in performing high-quality CPR, and the book consisted of the information of cardiac arrest. The printed materials were in English or Malay.
Sampling method
The approval from Faculty of Medicine Review Board and Human Research Ethics Committee of UniSZA sought before the study was carried out. The purpose of the study was explained to the participants, and their consent was obtained. Pre-intervention sociodemographic, knowledge, and attitude data were collected using Res-Q. To enhance the validity and reliability of the result, all participants will receive a same BLS module in the same setting.
At the end of the module, all participants were undergone a 2-min performance assessment using Resuscitation Feedback Device and post-intervention data collected using the same questionnaire.
Statistical analysis
Data were entered and analysed using Statistical Package for Social Science (SPSS), version 20. Descriptive statistics for all the variables were expressed as the mean and standard deviation (SD), meanwhile for categorical variables, they were expressed as frequency and percentage (%).
The dependent variables in this study were total knowledge and attitude scores with two levels of measurements, and an independent variable was the BLS module. Univariable analyses were performed to compare the baseline characteristics between medical and non-medical groups. Independent t-test was applied to determine the mean differences of variables between both groups. The repeated measures analysis of variance (RmANOVA) was used to evaluate the effectiveness of the intervention programme. A Pearson Chi-square test used to compare the effectiveness of chest compression in a medical and non-medical group. The level of significance was set at 0.05 with two-tailed fashion.
Results
Sociodemographic characteristics of the respondents for each group were shown in Table 1. For baseline characteristics, there were significant differences concerning age, academic qualification, previous CPR training, and experience with SCA (p < 0.001). Pre-intervention mean (SD) of total knowledge scores for medical and non-medical groups were 111.95 (12.83) and 84.47 (11.90), respectively. Meanwhile, the baseline mean (SD) total attitude scores were 28.39 (5.56) for a medical group and 26.25 (6.38) for the non-medical group.
Sociodemographic characteristics of respondents (n = 125).
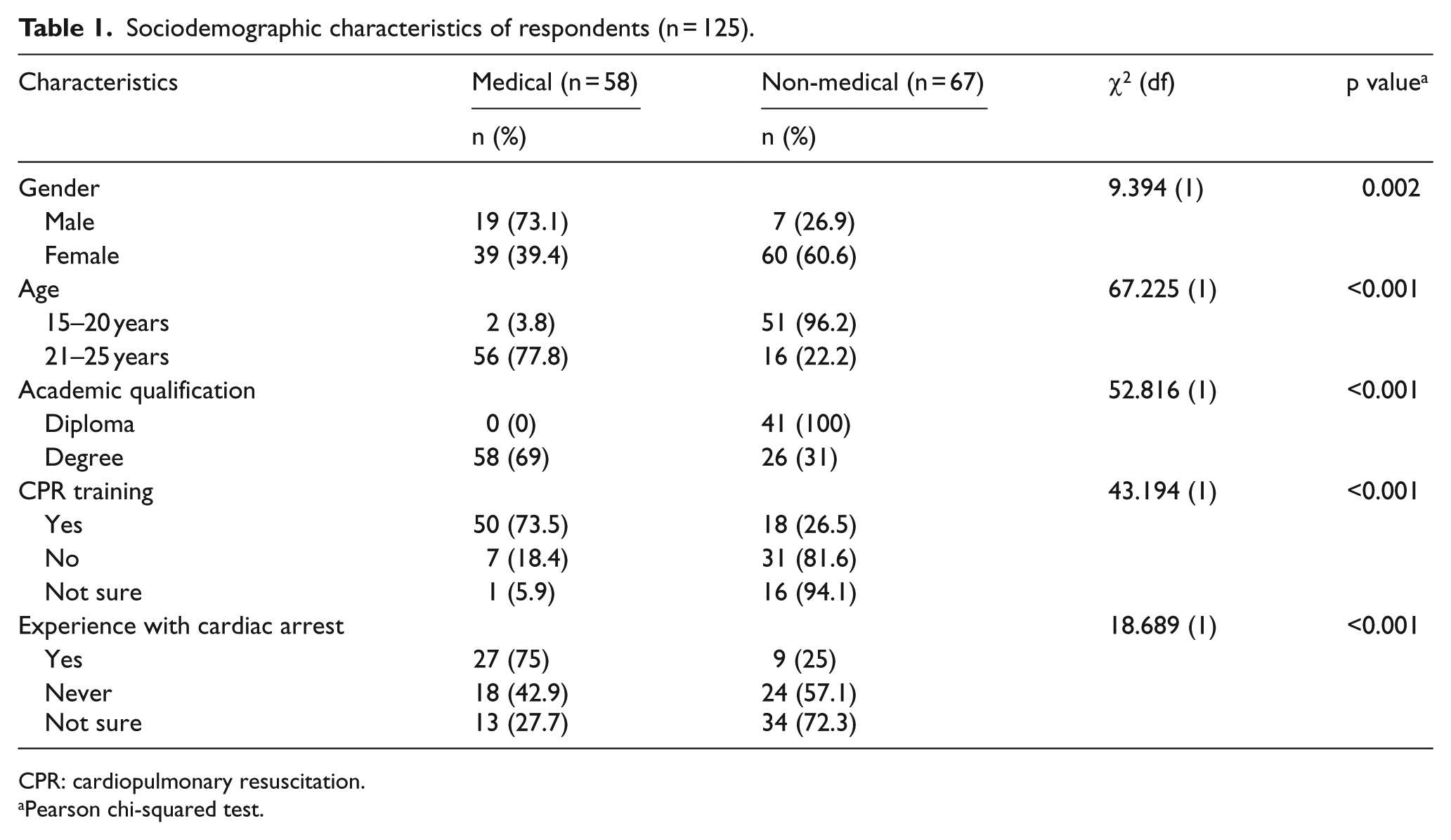
CPR: cardiopulmonary resuscitation.
Pearson chi-squared test.
Knowledge and attitude
Within-group factor analysis (time effect)
RmANOVA within-subject design (time effect) was performed with adjusted confidence interval and based on Bonferroni correction. The result is shown in Table 2. There were significant differences of total knowledge and attitude score within a group based on time. The total knowledge score was F = 188.41 (p < 0.001); knowledge on cardiac arrest score was F = 101.29 (p < 0.001), knowledge on the risk of cardiac arrest score was F = 70.49 (p < 0.001), and knowledge on CPR was F = 163.27 (p < 0.001). Meanwhile, total attitude score was F = 40.86 (p = 0.01). Pairwise comparison of total knowledge and attitude score with confidence interval adjustment was performed. The result showed that there were significant differences in knowledge and attitude between a medical student and non-medical student groups.
Comparison of knowledge and attitude score of CPR within each group based on time (time effect) using repeated measures ANOVA.
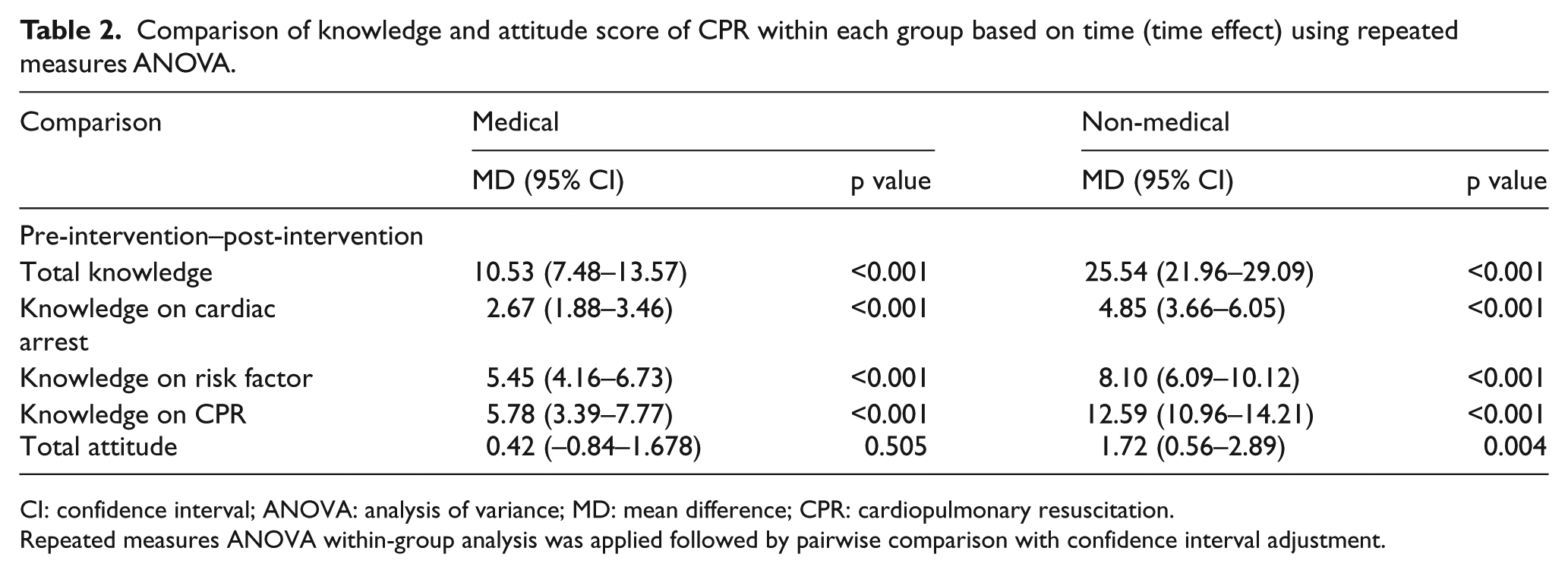
CI: confidence interval; ANOVA: analysis of variance; MD: mean difference; CPR: cardiopulmonary resuscitation.
Repeated measures ANOVA within-group analysis was applied followed by pairwise comparison with confidence interval adjustment.
As a conclusion, there was a significant difference in mean knowledge and attitude score within each group based on time.
Between-group factor analysis (group effect regardless of time)
Table 3 shows a comparison of mean knowledge and attitude scores on resuscitation between-group effects. From Test of Between-Subjects Effect, there were significant differences in mean total knowledge score (p < 0.001) and mean total attitude score (p = 0.014) regardless of time.
Comparison of knowledge and attitude score of CPR between two different groups (intervention effect regardless of time) using repeated measures ANOVA.
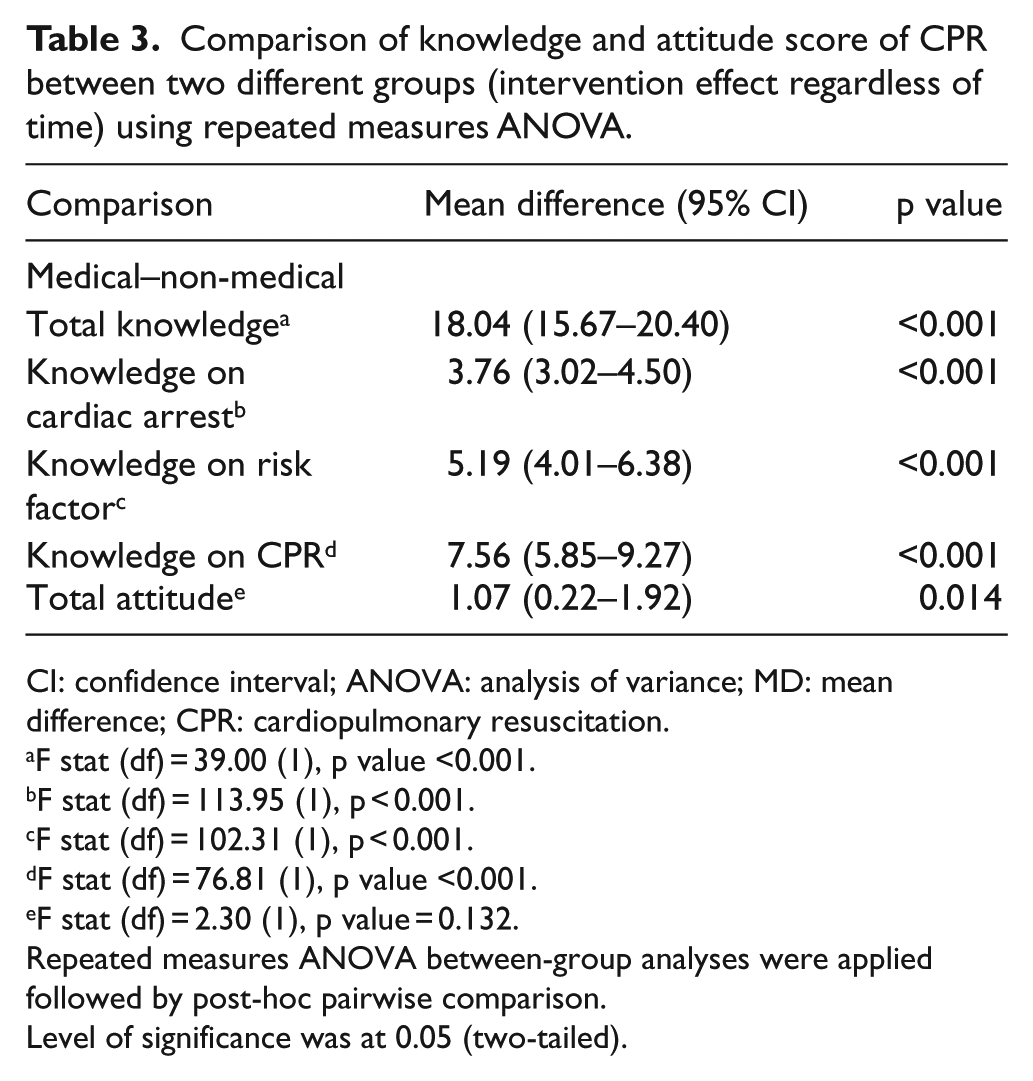
CI: confidence interval; ANOVA: analysis of variance; MD: mean difference; CPR: cardiopulmonary resuscitation.
F stat (df) = 39.00 (1), p value <0.001.
F stat (df) = 113.95 (1), p < 0.001.
F stat (df) = 102.31 (1), p < 0.001.
F stat (df) = 76.81 (1), p value <0.001.
F stat (df) = 2.30 (1), p value = 0.132.
Repeated measures ANOVA between-group analyses were applied followed by post-hoc pairwise comparison.
Level of significance was at 0.05 (two-tailed).
Within–between factor analyses (time–group interaction)
The comparison of knowledge and attitude scores on resuscitation among intervention and control groups based on time is shown in Table 4. There were significant differences in mean total knowledge score (F = 39.53, p < 0.001), mean knowledge on cardiac arrest (F = 8.57, p < 0.001), mean knowledge on risk factor of cardiac arrest (F = 23.61, p < 0.001), mean knowledge on CPR (F = 27.36, p < 0.001), and mean total attitude score (F = 6.24, p = 0.014) between two groups.
Comparison of knowledge and attitude of CPR between two different groups based on time using repeated measures ANOVA.
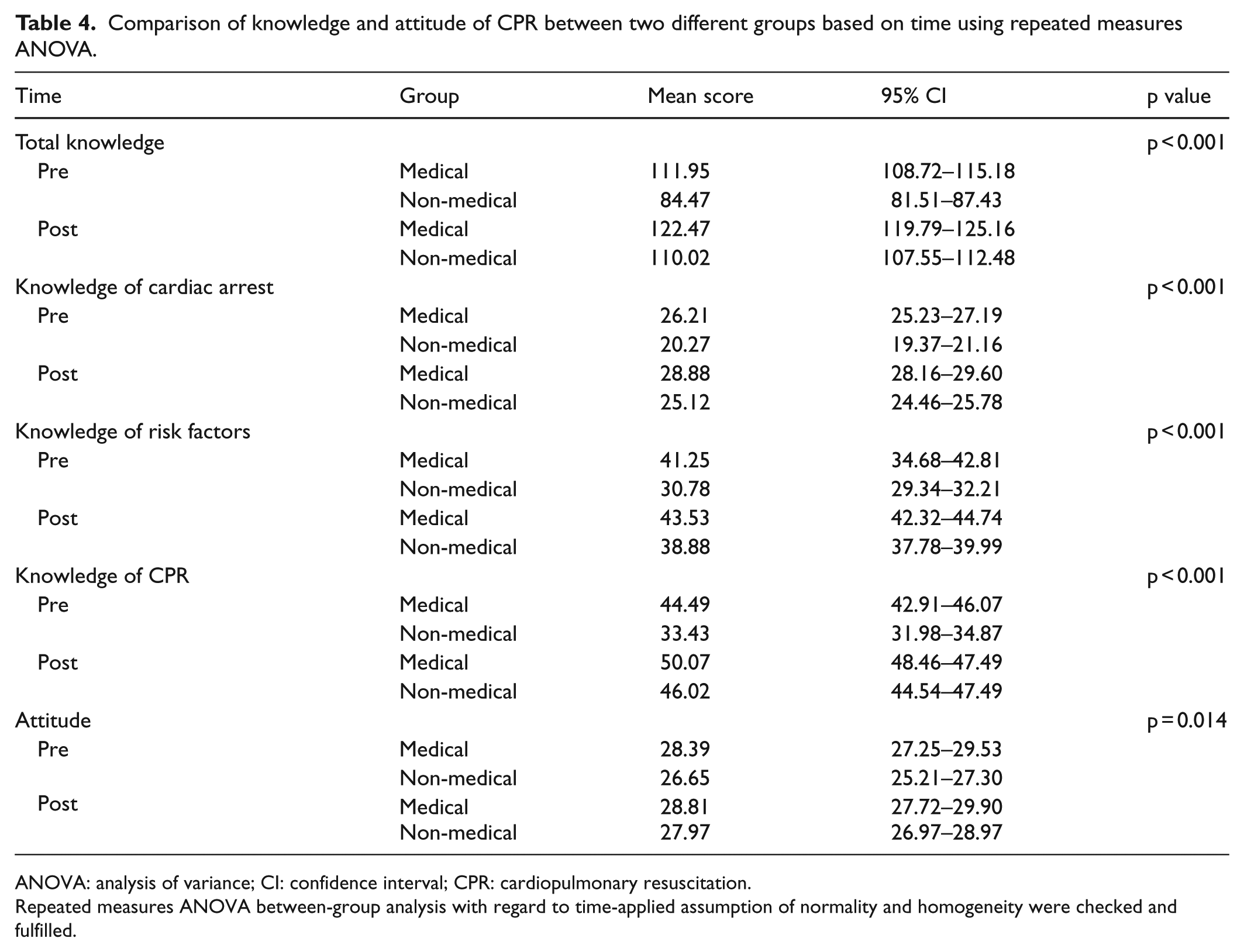
ANOVA: analysis of variance; CI: confidence interval; CPR: cardiopulmonary resuscitation.
Repeated measures ANOVA between-group analysis with regard to time-applied assumption of normality and homogeneity were checked and fulfilled.
Performance
The effectiveness of performing chest compression
This study revealed that 64.8% of the participants were able to achieve high-quality, effective chest compression: 32.8% from a medical group and 32% from a non-medical group. A non-significant interaction was found (χ2(1) = 1.646, p = 0.200) on effectiveness of performing CPR among medical group (32.8%) and non-medical group (32%). There were also no significant difference in adequacy of compression depth (χ2(1) = 2.247, p = 0.325), compression rate (χ2(1) = 3.041, p = 0.218), and CIT (χ2(1) = 1.158, p = 0.282) between medical and non-medical groups (Table 5).
Distribution of practice (effectiveness in chest compression) among medical and non-medical groups during intervention.
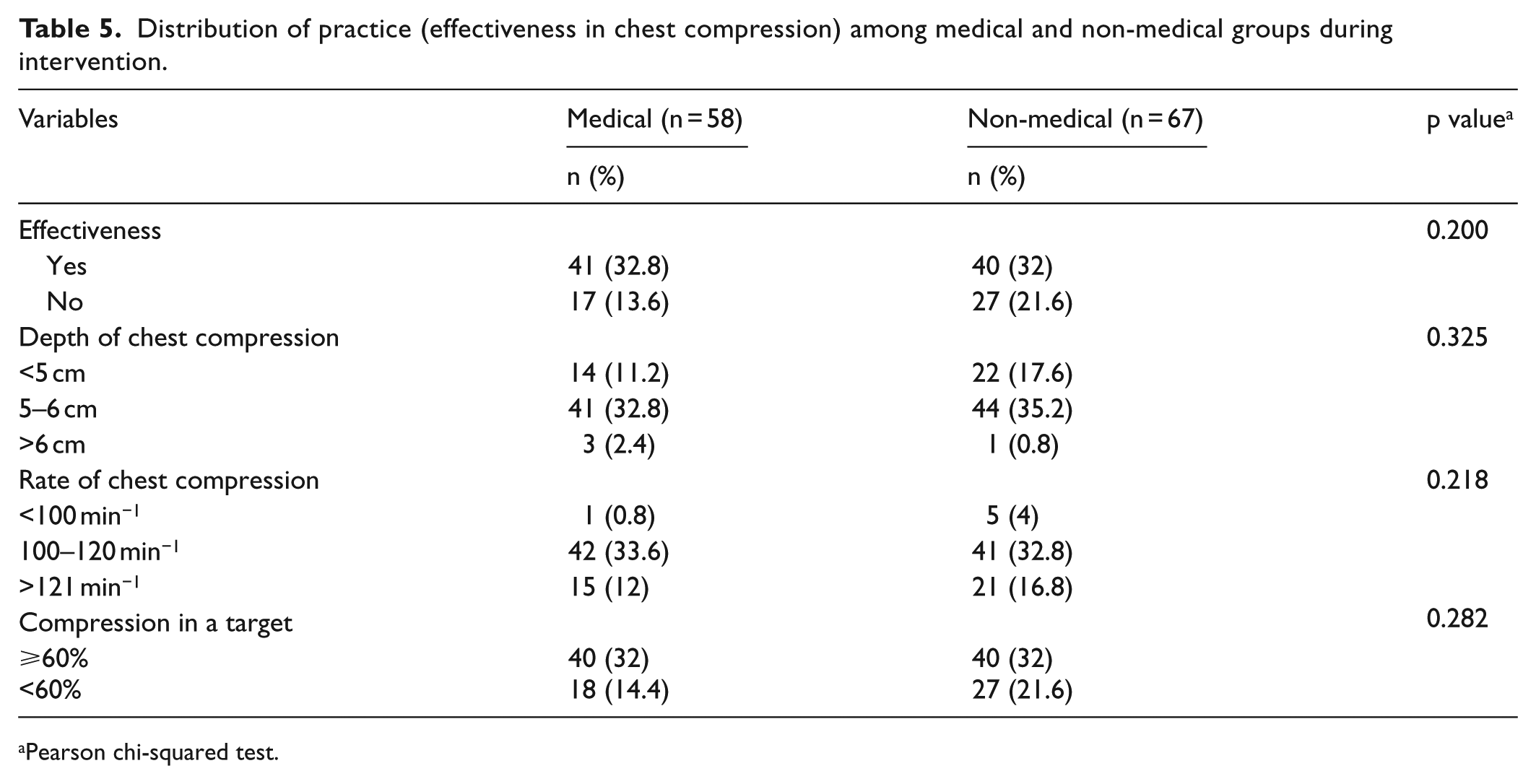
Pearson chi-squared test.
Discussions
Appropriate implementation of the chain of survival by the lay rescuer would increase a chance of survival victim who sustains OHCA. The first three chains which include immediate recognition of cardiac arrest and activation of the emergency response system, good quality of CPR and early defibrillation should be well digested and mastered by the lay rescuer who encounters victim with SCA. It is crucial to focus on optimising the quality of CPR among lay rescuer to maximise the return of spontaneous circulation (ROSC) rate from OHCA. 9 The traditional approach to CPR training failed to recognise the target participant, training setting, and how the training delivered. To date, no single CPR module is comprehensive, and an ideal community approach will consolidate all these modules. 20
In this study, we have set our target to compare the effectiveness of modified BLS module on knowledge, attitude, and performance (KAP) towards CPR among medical students who represented as healthcare rescuer and non-medical who represented as a lay rescuer.
This modified BLS module integrates an andragogy classroom approach (student-centred approach) with modern technology. The andragogy approach is an adult learning method. The learners are more independent with a climate of mutual respects and collaboration, evaluation and progress measured by mutual discussion between student and teacher, a problem-solving method as a medium to deliver the information and extremely conducive to increase self- directed learning. 21 It utilised 10 learning techniques proposed by Agarwal et al. 22 This learning technique was used to improve the success across a wide variety of domains. The techniques are (1) elaborative interrogation, (2) self-explanation, (3) summarisation, (4) highlighting, (5) keyword mnemonic, (6) imagery of text, (7) rereading, (8) practical testing, (9) distributed practice, and (10) interleaved practice. The modified BLS module also used modern equipment such as CPR feedback and an audio-visual input such as video-based CPR. This additional mode of teaching deliveries can increase the depth of understanding, improve the technical competencies and the knowledge retention.23–29
The sociodemographic analysis showed that these two groups were significantly different in terms of age, educational background, and experience in CPR. Reasonably, the medical group would have an enormous gap in KAP compared to the non-medical group. This study showed that 64.8% of the participants were able to perform a high-quality and effective chest compression. In this study, we set a standard of effective chest compression criteria as recommended by AHA guideline 2015. Interestingly, there was no significant difference in the quality of chest compression between these two groups (p = 0.269).
This modified BLS module was able to significantly increase the knowledge and attitude scores of the respondents from both groups with regard to time as shown in RmANOVA. There were differences in the mean knowledge and attitude score between these groups in pre- and post-intervention. The knowledge and attitude scores were higher in a medical group, but interestingly, this study found that non-medical group showed the greater increment of post-intervention knowledge and attitude score compared to the medical group.
The role of CPR course is pivotal to increase the awareness towards CPR in the community. The programme is essential for providing an individual with useful information, skills, and motivation required in dealing with the life-threatening situation. Conducting the programme especially in the university is a necessary step in promoting early intervention in cardiac arrest to the younger generation and contributing to the overall improvement of SCA prognosis. Younger population is more accessible, keen, and capable of learning newer skills and is more willing to perform CPR. 30 In addition, training the students could ultimately translate to a broader spread of knowledge about CPR in the whole population. 31
In Malaysia, there were studies of KAP on CPR in various levels of the community. A prospective intervention multicentre controlled trial study found that level of knowledge and attitudes of secondary school children were acceptable before the intervention. Furthermore, a brief CPR training programme improved their standard of knowledge and attitudes significantly as compared to those who had never trained. 32 A local survey study found that junior doctor had adequate knowledge and attitude towards CPR but lacked confidence in performing CPR when it came to an actual case. 33
The cross-sectional study among college students in Thailand found that level of knowledge and attitudes were significantly increased after CPR training. 34 Another study conducted in Japan showed that simplified CPR training programme for non-medical staff of university hospital improved the quality and attitude towards CPR and usage of an automated external defibrillator (AED). 35 A series of studies revealed brief episode CPR training with an instructor-led training and CPR feedback improved CPR skill retention and effectiveness in both healthcare and lay rescuer.23,24 These findings were consistent with the Cochrane database of systematic reviews which found that competent evidence supporting the use of CPR feedback devices during CPR training could improve skill acquisition and retention. 25
A local study was conducted to evaluate the effectiveness and retention of learning AED usage in non-critical care nurses. They found that new self-instructed video was as good as traditional classroom instruction in providing the knowledge, competency, and confidence in performing AED defibrillation. 26 Recently, new approaches were designed to increase the effectiveness of CPR training. One of the proposed methods was online CPR training. This approach was supported by a randomised control trial study that found video-based CPR course to yield higher retention and better skill than classroom course. 27 Video-based CPR course was also found to be effective in older adults 28 and high-school students. 29
Different methods of education levels have been done in previous studies. Each had its weaknesses and strengths, so did in the module used in this study. Even though it was adequate in improving knowledge, attitude score, and performance in two study groups, the module has not been tested elsewhere previously. It also has not been tested for retention. Due to time limitation, evaluation of the effectiveness of each component of the package (lecture, video presentations, and printed materials) was not done. Besides, the intervention was delivered only once and in short period to improve the knowledge, attitude, and performance of the respondents. Developing competent lay rescuer seems to take much longer time and constant reminder and reinforcements. Despite all the weaknesses, the findings in this study did provide useful baseline information for future intervention programme.
Conclusion
A high-quality chest compression was successfully obtained by both medical and non-medical groups after a modified BLS module. Knowledge and attitude were also improved significantly. It showed that with a comprehensive module and adequate training, a rescuer could perform an effective chest compression regardless of their medical background. Further research is necessary to evaluate the retention and skill-lab-based performance to actual performance when encounters with a real cardiac arrest event. Nevertheless, this module is reliably appropriate for healthcare rescuer and lay rescuer. It will reduce the knowledge and competency gap between these two groups. They will communicate and perform in the same manner, and it will facilitate the continuation and transfer of care. It also can reduce the misunderstanding and misconception of CPR among non-medical personnel. Ultimately, this will benefit the community by creating a safer environment since the lay rescuer can perform CPR as effective as healthcare rescuer.
Limitations
This study had several significant limitations. First, we omitted provider fatigue as a factor for poor CPR as our participants were a youngster and claimed not to have any medical illness. Second, the consented non-medical participants were intrinsically more likely to have a positive attitude and higher ability to learn CPR. Third, we did not measure the hands-off time as in previous studies. The analysis confined to periods during the active chest compressions phase only. The current evidence mentioned about minimising interruption to ensure a high-quality CPR and time consumed during hands-off positively associated with increased mortality. Our study aim was to compare the quality of chest compression delivered rather than the amount of time performing CPR.
Footnotes
Acknowledgements
The authors wish to express their gratitude to the experts, facilitators from UniSZA Resuscitation Training Committee and Terengganu Resuscitation society, enumerators, and Zoll Malaysia for their contribution to this study. All authors participated sufficiently in the work and agree to take public responsibility for appropriate portions of the contents.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors whose names are listed immediately below certify that they have no affiliations with or involvement in any organisation or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received university grant (UniSZA/2015/GOT/02) from Universiti Sultan Zainal Abidin.
Availability of data and materials
All data were primary and could be provided if required.
Informed consent
Personal, demographic details and pre- and post-intervention data of the participants were collected and recorded after getting informed consent.
Ethical approval
Research conducted at the Faculty of Medicine, UniSZA in this study was approved by the UniSZA Human Ethics Research Committee (UHREC; Ref. No: UHREC/2016/3/012) and Universiti Sultan Zainal Abidin (UniSZA; Kuala Terengganu, Malaysia) on 21 June 2016. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the UHREC.