
Abstract
Introduction:
Cupping therapy has been widely performed in oriental countries and considered a safety alternative to relieve pain. Here, we report a rare complication from abdominal cupping. Case presentation: A 49-year-old man presented with a 2-day history of left upper quadrant abdominal pain after cupping therapy 3 days earlier. His abdomen was soft but appeared a localized rebounding tenderness. Contrast-enhanced computed tomography of the abdomen showed intraperitoneal hemorrhage originated from the left upper quadrant of the omentum.
Discussion:
Several mechanisms are proposed for the development of intraperitoneal hemorrhage after cupping therapy, including the tensile stress generated by cupping that facilitates the disruption of omentum vessels, strong negative pressure generated by cupping that suppresses blood supply to the cup-applied sites causing adjacent tissue ischemia, and subsequent vascular extravasation. Treatment for intraperitoneal hemorrhage depends on clinical conditions. Stable patients can be managed conservatively, whereas surgery is reserved for those with continuous bleeding and hypovolemic shock.
Conclusion:
Cupping therapy complicated with omentum bleeding can present insidiously until peritoneal irritation developed by intraperitoneal hemorrhage. A comprehensive history taking and a high degree of vigilance are crucial to diagnose early patients with this rare complication.
Case
A 49-year-old otherwise healthy male presented to the emergency department with 2-day history of left upper quadrant abdominal pain, which was characterized as a dull, severe, and persistent aching, with a gradual increase in intensity. The pain was not associated with meal and not accompanied with nausea and diarrhea. On arrival, the patient was afebrile. Vital signs were unremarkable. His abdomen was soft but showed a rebounding tenderness over the left upper quadrant. In addition, there were circular bruises measuring 5 cm in diameter over the upper back and left upper quadrant. Laboratory tests showed hemoglobin of 12.9 g/dL and were insignificant for the other tests. The patient denied any history of medication use and trauma event, yet he recalled receiving cupping therapy 3 days earlier because of muscle strain of his back. Point-of-care ultrasound showed minimal intra-abdominal fluid accumulation over Morrison’s pouch and splenorenal fossa. Contrast-enhanced computed tomography of the abdomen revealed one heterogeneous hematoma measuring 4.0 × 2.5 × 2.3 cm3 over the left upper abdomen with accumulation of bloody ascites (Figure 1). Given the nature of ongoing pain and potentially continuous intra-abdominal bleeding (hemoglobin downed to 11.4 g/dL 8 h later), diagnostic laparoscopy was performed. The results revealed bloody clots and mild oozing over the left upper portion of the greater omentum, which confirmed the diagnosis of the greater omentum tear with hemoperitoneum. The patient received debridement with the placement of Sil-Med drain and was discharged uneventfully 1 week later.
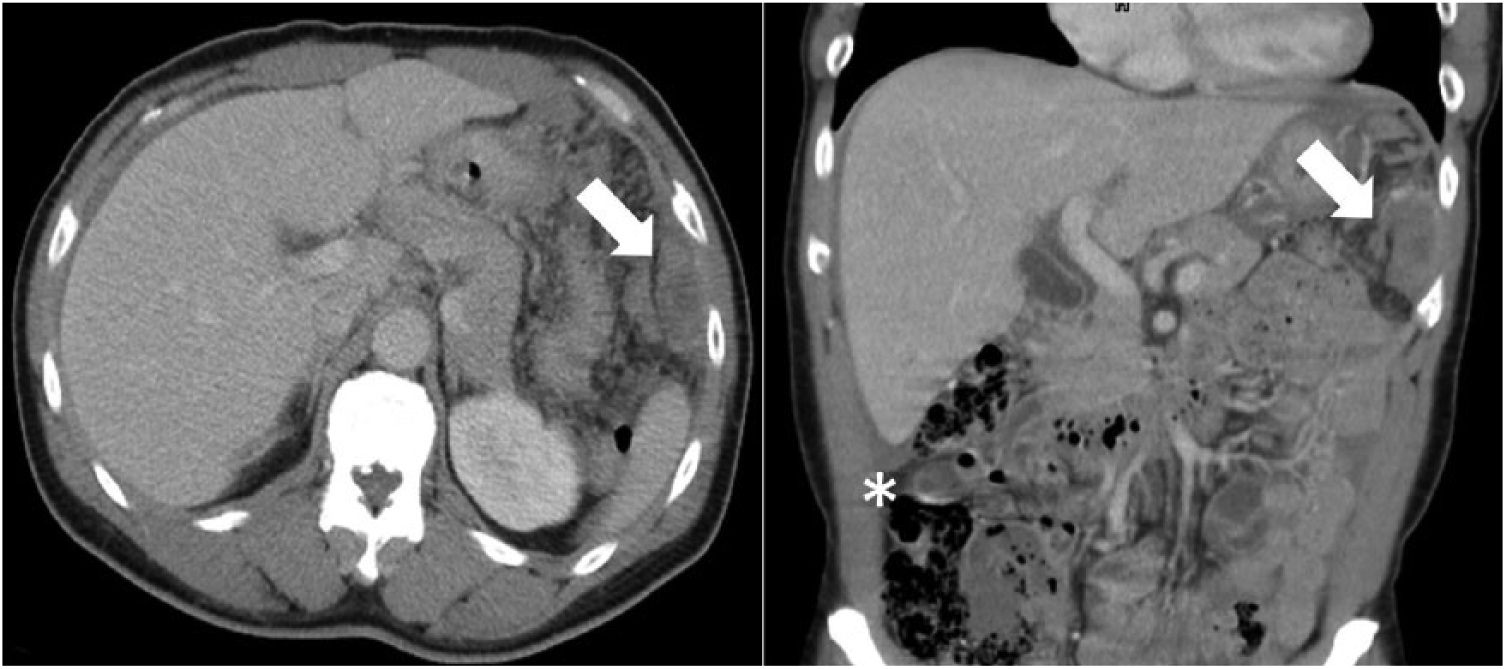
Contrast-enhanced computed tomography of the abdomen showed a heterogeneous mass measuring about 4.0 × 2.5 × 2.3 cm3 without contrast enhancement (arrowhead) over the left anterolateral upper abdominal wall and ascites (asterisk) in the intraperitoneal cavity.
Discussion
Cupping therapy is a traditional treatment that has been widely performed in Asian countries to relieve pain. Although cupping therapy was considered a safety alternative, there have been a few reports on its complications, such as bullae, keloids, 1 vasovagal syncope, panniculitis, 2 and even hemorrhagic stroke. 3 Here, we report a case of intraperitoneal hemorrhage after cupping therapy. To our knowledge, this is the first report of intraperitoneal hemorrhage complicated by cupping therapy.
Intraperitoneal hemorrhage could be attributed to any intra-abdominal solid organ disorders (liver, spleen, pancreas, kidney, intestine, omentum, gynecological organs, tumors, etc.), vascular disorders (aneurysm, varices), or coagulation disorders. The present case has no history of medical disease, trauma, or use of coagulant, except cupping therapy applied to his back and flanks 5 days prior to the emergency department visit. Cupping therapy refers to a cup that is attached to the skin surface to cause congestion through negative pressure created by heat. After cupping, blood stasis or bruise over the suction sites is frequently seen. Blunt and Lee 3 had reported that the tensile stress generated by cupping therapy might facilitate the development of vessel dissection in the presence of an intimal tear. In our case, the tensile stress from cupping therapy could possibly tear the vessels within the omentum and subsequently lead to hemoperitoneum. Another probable mechanism is that the strong negative pressure generated by cupping suppresses the blood supply to the omentum under the cup-applied site and causes adjacent tissue ischemia. The damaged omental tissue might further potentiate vascular extravasation after reperfusion.
Stable patients with intraperitoneal hemorrhage can be managed conservatively. Percutaneous transcatheter embolization therapy is considered for those who have active extravasation of blood detected on computed tomography in stable hemodynamics. Exploratory laparotomy is reserved for those who are hemodynamically unstable, uncertainty, and for clinically deteriorating conditions following conservative diagnostic management. 4 Kleinsasser had reported that the mortality of intraperitoneal hemorrhage was 8.6% if the bleeder could be identified and ligated. In contrast, the mortality could reach as high as 56% if a bleeding site could not be detected. 5 Nevertheless, in approximately 30% of the intraperitoneal hemorrhage the bleeding source could not be identified even after surgery. 6 Diagnostic laparoscopy has a strength of providing tissue diagnosis, avoiding unnecessary surgery, avoiding unnecessary delay in diagnosis and treatment, and shortening the operative and hospitalization period. However, it provides only an alternative not a substitute for traditional diagnostic procedures and will never lessen the importance of conventional laparotomy. 7
Cupping therapy complicated with omentum bleeding can present insidiously until peritoneal irritation developed by intraperitoneal hemorrhage. Physicians may be unfamiliar with cupping therapy and rarely observed this serious complication resulted from cupping maneuvers. A comprehensive history taking and a high level of vigilance are crucial to diagnose early patients with this rare cupping-related complication.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of National Defense (MAB-105-088).
Availability of data and materials
All data were obtained retrospectively from chart review.
Ethical approval
The study was approved under TSGH IRB No. T-22029.
Informed consent
Written informed consent was obtained from the patient for research publication.
Human rights
The report was written after TSGH IRB approval and was without any identifiable personal information.