
Abstract
Bites by venomous snakes can cause fatal systemic and coagulation disorders. Rare complications, such as compartment syndrome and hemoperitoneum, may also require surgical intervention. Here, we describe our experience with an unusual case of snakebite-induced delayed splenic rupture. A 54-y-old male with no specific medical history visited a local hospital for a bite by an unidentified snake. He had been bitten on the left thumb and was administered antivenom. He was discharged from the local hospital after 3 d when his symptoms had improved. However, he revisited our emergency medical center 2 d later, reporting dizziness with diaphoresis. Focused abdominal ultrasonography and computed tomography revealed large amounts of intraperitoneal fluid collection and hemoperitoneum with splenic rupture, respectively. The patient underwent immediate blood transfusion and received antivenom treatment in our emergency department and, subsequently, emergency splenectomy. Histopathologic findings at the time of surgery revealed multifocal lacerations on the external surface of the spleen, with fresh hemorrhage. He recovered 7 d after surgery without any complication.
Introduction
According to the World Health Organization, 200 of about 600 viper species are of medical concern. 1 In Korea, 14 types of snakes have been reported, including 5 species of viper: Gloydius brevicaudus, Gloydius ussuriensis, Gloydius saxatilis, Gloydius blomhoffii, and Rhabdophis tigrinus. 2 The World Health Organization reported that 4.5 to 5.4 million snakebites and 81,000 to 138,000 deaths occur annually. 1 Venom is not injected in about 10 to 15% of venomous snakebites, and symptoms are usually local. 3 In Africa, some snakes, such as spitting cobras, have a dry bite rate of 50%. 4 Conservative management is recommended as an initial treatment for snakebite victims.
Antivenoms specifically bind to venoms or the molecular targets of venoms and block their activities and thus may be considered treatment options. 2 In Korea, antivenom is used to prevent the spread of local tissue damage and to reduce hematologic abnormalities and systemic toxicity. Antivenom should be administered within 3 h of a bite if hematologic abnormalities and systemic toxicity are observed or if local edema progresses to affect more than half of an affected limb—necrosis or compartment syndrome may develop at bite sites. 5 However, few detailed studies have been conducted on optimal dosages or methods of antivenom administration. 6
Local symptoms are slow to improve after antivenom administration. In Korea, therapeutic effects on coagulopathy usually begin to appear within 1 h of administration, and the effects of antivenom subside within 12 to 30 h. Prothrombin time (PT) recovers within 6 to 24 h and fibrinogen within 20 to 48 h. 2
Rare complications requiring surgical intervention, such as compartment syndrome and hemoperitoneum, can also occur. 7 Here, we describe our experience of an unusual case of delayed splenic rupture after a venomous snakebite; rupture occurred after local complications had improved.
Case Report
A 54-y-old male with no specific medical history who was a social drinker (1–2 times per week) visited a local hospital after being bitten on his left thumb by a snake of unknown species. He received 1 vial of antivenom (Kovax freeze-dried Agkistrodon [Korean mamushi] antivenom 6000 units/vial; Korea Vaccine Co., Ltd, Ansan-si, Gyeonggi-do, Korea) and was discharged from the local hospital 3 d later after his symptoms had improved. However, 2 d later, he visited our emergency medical center reporting dizziness, diaphoresis, nausea, vomiting, and subtle abdominal pain. He had no recent specific trauma history.
At second presentation, swelling at the bite site was somewhat improved (Figure 1). Local pain was not observed, and his vital signs were as follows: blood pressure, 126/95 mm Hg; heart rate, 90 beats·min-1; respiratory rate, 20 breaths·min-1; and body temperature, 34.2°C. Initial laboratory tests showed hemoglobin 10.2 g·dL-1, white blood cells 16700 cells·μL-1, platelets 95000 cells·μL-1, creatinine 1.78 mg·dL-1, aspartate transaminase 46 U·L-1, and alanine transaminase 29 U·L-1. However, his PT was 25 s (normal 11–13), his activated partial thromboplastin time was 170 s (normal 24–31), and his fibrinogen level was less than 30 mg·dL-1 (normal 205–429 mg·dL-1). His PT international normalized ratio was 2.19 (normal 0.92–1.13) but fell to 1.20 after antivenom injection.
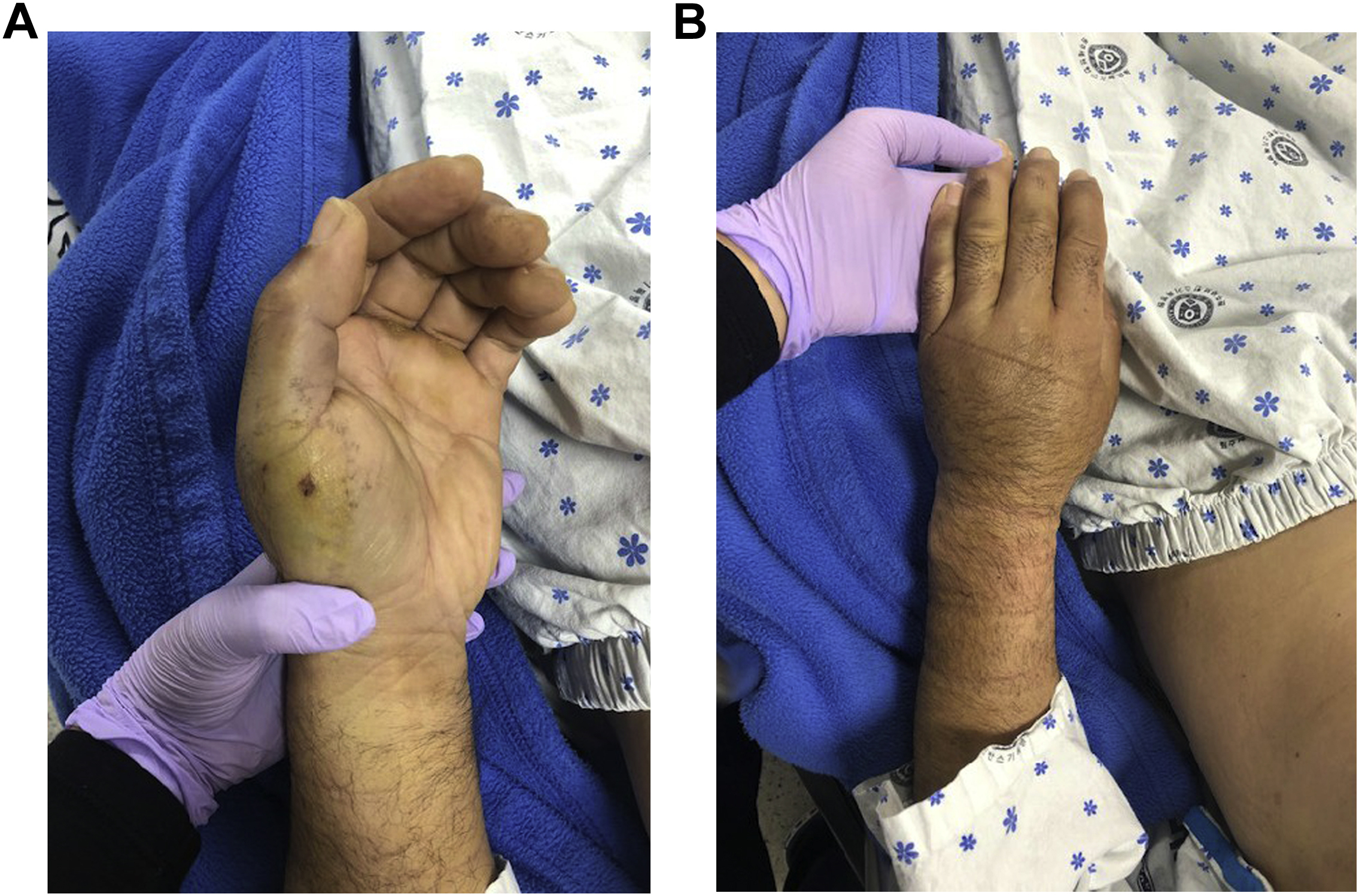
Photographs of the damaged hand. Palm of hand (A), Dorsum of hand (B).
One hour after he visited, the patient reported more intense abdominal pain, and repeat laboratory testing revealed a hemoglobin level of 6.5 g·dL-1. Focused abdominal ultrasonography confirmed intraperitoneal fluid collection in Morison’s pouch, the splenorenal recess, and perivesical space (Figure 2), and abdominal computed tomography visualized a large hemoperitoneum with splenic rupture (Figure 3). The patient then deteriorated, and his blood pressure fell to 85/37 mm Hg. Accordingly, he was administered 2 units of packed red blood cells, 2 units of fresh frozen plasma, and 1 vial of antivenom in our emergency department and immediately underwent emergency splenectomy. Histopathologic findings at the time of surgery revealed multifocal lacerations on the external surface of the spleen with fresh hemorrhage. Seven days after laparotomy, he was discharged without any complications.
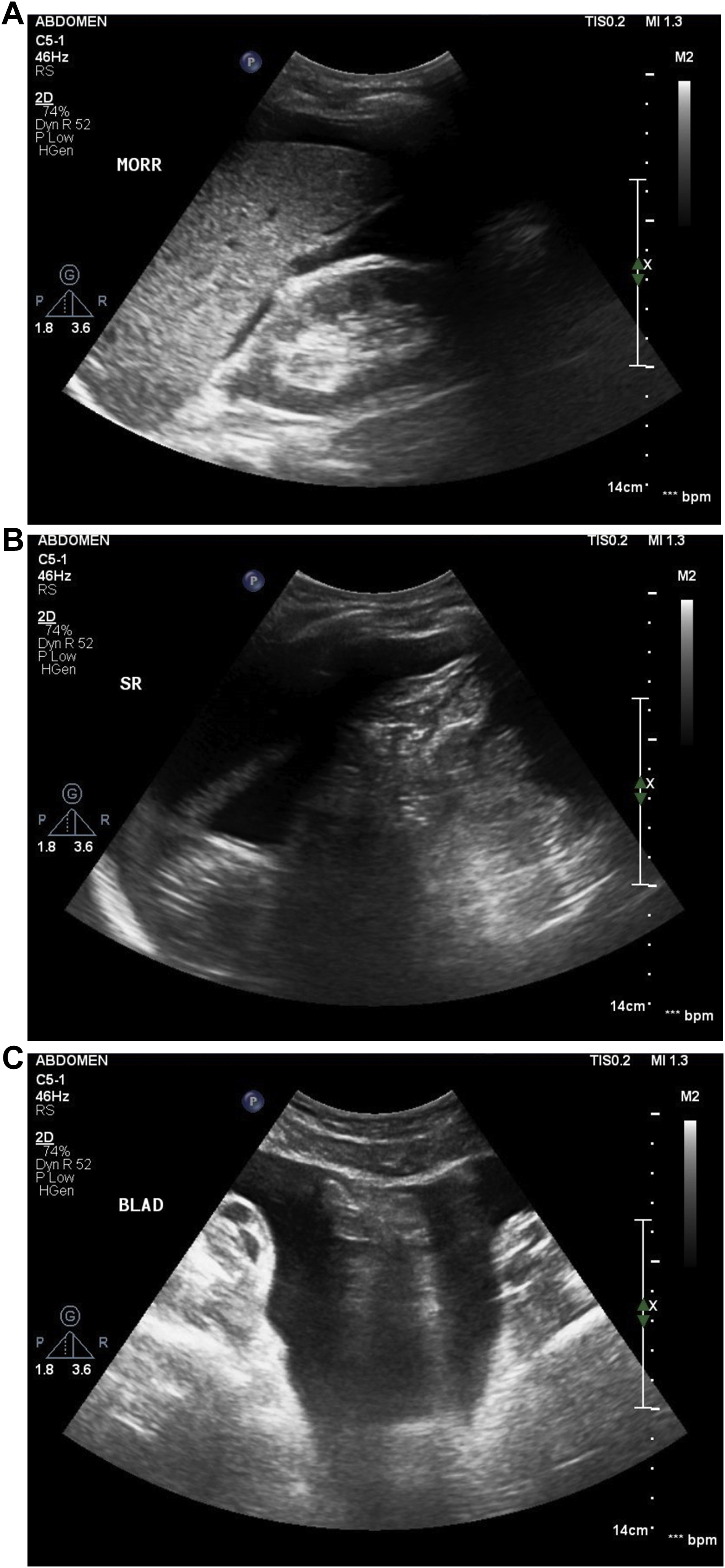
Focused abdominal ultrasonographic images obtained in the emergency department showing a large amount of fluid collection in Morison’s pouch (A), the splenorenal recess (B), and the peri-bladder space (C).
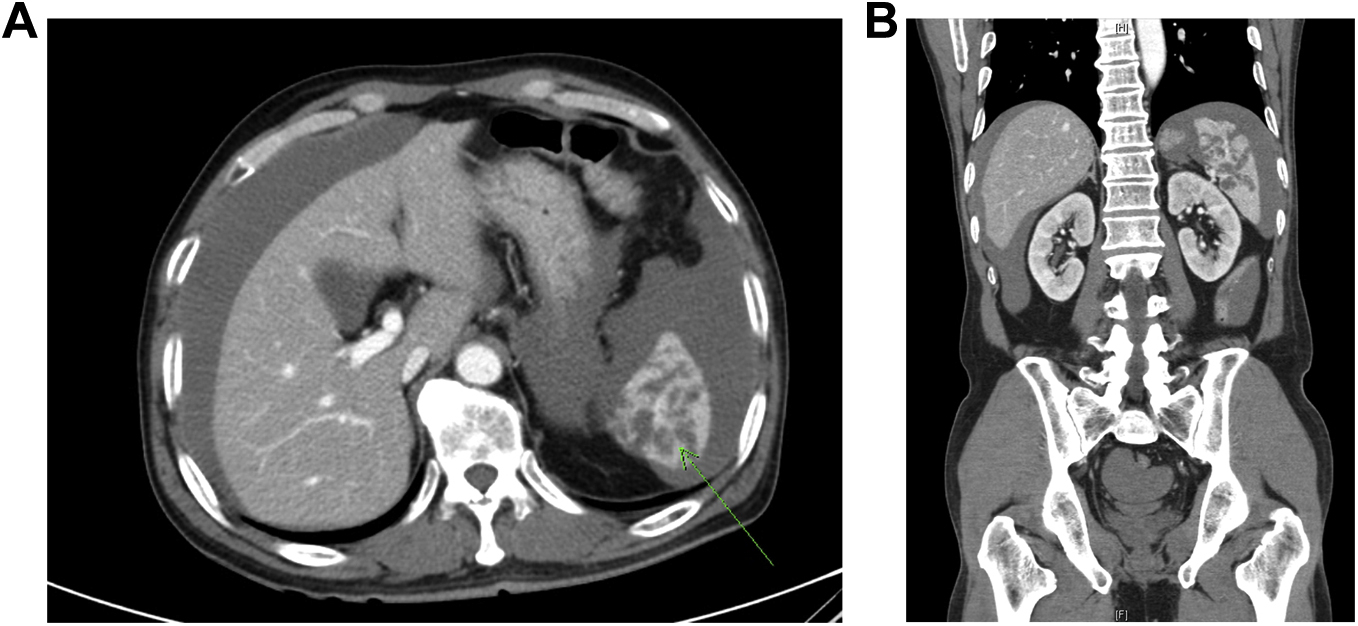
Abdominal computed tomography findings suggested splenic injury (A) with intraperitoneal hemorrhage (B).
Discussion
In general, snakebite cases exhibit 1 or more indications of a bite, such as skin penetration or scratches. Local symptoms vary, occurring within 1 h or more than 8 h. 8 These symptoms include edema, erythema, hemorrhage, and pain, which develops in more than 90% of cases immediately after a bite. Early systemic symptoms include nausea, vomiting, numbness around the mouth, numbness in the fingertips or toes, muscle tremors, lethargy, and general weakness. Blood clotting disorders are evidenced by elevated PT international normalized ratio and PT/activated partial thromboplastin time levels, hypofibrinogenemia, elevated fibrinogen degradation production, and decreased platelet counts.2,9 Phospholipase A2, serine protease, metalloprotease, L-aminoacid oxidase, phosphoesterase, distinegrin, and C-type lectin protein are components of snake venom and may have anticoagulant or antithrombotic effects by acting on blood coagulation factors, platelet receptors, perivascular matrix, and vascular endothelial layers. In addition, the anticoagulant, coagulant, antithrombotic, or thrombotic effects of snake venoms damage blood vessel walls and prevent platelet aggregation and thus increase capillary permeability and cause bleeding.10,11 These effects are probably the main cause of snakebite-induced hemoperitoneum.
The spleen is a delicate organ and contains many blood vessels. Most splenic ruptures are caused by trauma or occur secondary to tumors, infections, and invasive diseases. However, in patients with impaired coagulation, splenic rupture can occur even after minor damage. 12 Various reports from India and Africa have noted coagulation disorders (eg, intraperitoneal bleeding, hemothorax, and internal bleeding) caused by snakebites. 13 -15 In 2016, the World Health Organization recommended repeat antivenom administration at the initial dose if the following conditions are met: 1) blood remains uncoagulable 6 h after initial antivenom administration; 2) profuse bleeding persists (antivenom should be readministered within 1 to 2 h); or 3) signs of neurotoxicity or cardiovascular compromise deteriorate. 16 The side effects of antivenoms include itching, hives, dry cough, fever, nausea, vomiting, abdominal pain, diarrhea, tachycardia, hypotension, organ contraction, and angioedema. However, the Kovax freeze-dried Agkistrodon antivenom used in Korea has few side effects related to coagulopathy. 2 It was on this basis that the second dose of antivenom was administered to our patient.
Three cases of abdominal hemorrhage after snakebites have been reported in South Korea. The individuals concerned usually displayed local symptoms and were rapidly diagnosed. A 2014 case report described snake venom–induced splenic rupture caused by direct vascular endothelial injury and disseminated intravascular coagulation. The patient presented with severe localized swelling and abdominal pain, and hemoperitoneum was found after 4 d. 17 In South Korea, a patient who presented with abdominal pain 1 d after a snakebite was diagnosed as having spleen rupture. 18 A patient with only local edema and pain after a snakebite was diagnosed with hepatic necrosis and rupture 4 d later. 19 In 2019, we also reviewed a case of atraumatic spleen rupture caused by venom-induced coagulopathy 3 d after a snakebite. 20
Although our patient was not an alcohol abuser and had no underlying disease, idiopathic splenic rupture occurred. Unlike some previous reports on snakebites, the described case is unusual because rupture was caused by delayed systemic reaction after local symptoms had improved. Kovax freeze-dried Agkistrodon antivenom was developed in horses against Agkistrodon halys in China. 2 This antivenom used in Korea is not manufactured to specifically target the venoms of snakes indigenous to Korea, and the effectiveness of antivenom is doubted because the targeted venom is extracted from Chinese vipers.
This case study demonstrates that despite improvements in local symptoms after a snakebite, splenic rupture may occur up to 1 wk later, which cautions that follow-up evaluation may be required even after antivenom treatment.
Footnotes
Acknowledgements
Author Contributions: Acquisition of data and drafting of the manuscript (TYK); analysis of data (YIR); critical revision of the manuscript (KCC, SOH); drafting of the manuscript and critical revision of the manuscript (WJJ). All authors approved the final version of the manuscript.
Financial/Material Support: None.
Disclosures: None.