
Abstract
Introduction
Salmonella is an enteroinvasive bacterium. Salmonella infections occur mainly via ingestion of contaminated food, most commonly being poultry products, eggs and egg products. It is one of the leading food-borne illnesses causing a considerable morbidity and mortality worldwide. 1 In general, Salmonella infection can be divided into five categories, including gastroenteritis, enteric fever, bacteraemia, localized infection and chronic carrier state. Gastrointestinal (GI) manifestations of nontyphoidal Salmonella infection include hepatomegaly, splenomegaly, cholecystitis, cholangitis, and splenic or hepatic abscesses, but these are overall uncommon.2,3 We report a rare GI complication of nontyphoidal Salmonella infection. A patient suffering from nontyphoidal Salmonella developed acute acalculous cholecystitis. Acute acalculous cholecystitis is frequently associated with gangrene and perforation. Prompt diagnosis and surgical intervention are essential to reduce complications and mortality.
Case
An elderly patient, who had history of ischaemic stroke, vascular dementia, hypertension and dyslipidaemia, was presented to our emergency department in April 2016 with symptoms of acute gastroenteritis for 1 day. This patient presented with fever, vomiting of undigested food twice and watery diarrhoea once. This patient was a nursing home resident, did not have history of recent travelling and there was no recent outbreak of gastroenteritis in the nursing home. At presentation, this patient was dehydrated with blood pressure of 139/89 mm Hg, pulse rate of 120 beats per minute and body temperature of 38.0°C. On physical examination, the abdomen was soft with active bowel sound. The initial complete blood picture showed white cell count (WCC) of 10.0 × 109/L (reference range: 3.7–9.2 × 109/L), normal haemoglobin and platelet levels. The initial biochemical markers showed normal creatinine level but hyponatraemia (sodium level: 128 mmol/L) and normal liver function. This patient was rehydrated with intravenous fluid replacement and admitted to the Emergency Medicine Ward (EMW) for further management. Ciprofloxacin was started empirically in view of severe symptoms of gastroenteritis. The patient’s condition improved and diarrhoea subsided with medical treatment. Stool culture had isolated Salmonella Group B. Polymerase chain reaction tests of stool for rotavirus, norovirus and Clostridium difficile toxin were all negative. However, the patient developed persistent fever. Ciprofloxacin was changed to Ceftriaxone. Septic workup showed negative blood and urine culture. Sputum culture grew commensals only. Abdomen remained soft and non-tender on physical examination. Blood tests which were repeated on day 7 showed deranged liver function (alkaline phosphatase 221 U/L (reference range: 30–120 U/L), alanine aminotransferase 87 U/L (reference range: <50 U/L), normal bilirubin level). WCC remained within normal range. Bedside ultrasonography (USG) showed high-riding liver and distended gall bladder with no definite gallstone detected. Sonographic Murphy’s sign was not able to be elicited as the gall bladder was covered by the rib cage. Urgent computed tomography (CT) scan of thorax, abdomen and pelvis was done to search for the septic source. CT scan showed thickened gallbladder wall with patchy areas of increased enhancement which was suggestive of acute cholecystitis (Figure 1). Tiny hyperdense foci were noticed at the gallbladder neck. Gallstones or sludge were suspected. The patient was then transferred to surgical unit, and urgent percutaneous cholecystostomy was performed. Antibiotic therapy was continued. Bile and blood culture did not isolate any organisms. The fever had subsided and liver function improved after the procedure. Percutaneous cholangiogram was performed about 4 weeks later and showed no free leakage. Tiny filling defects were noticed in gall bladder, they were likely to be sludge. PTC (Percutaneous Transhepatic Cholangiogram) drainage catheter was then removed.
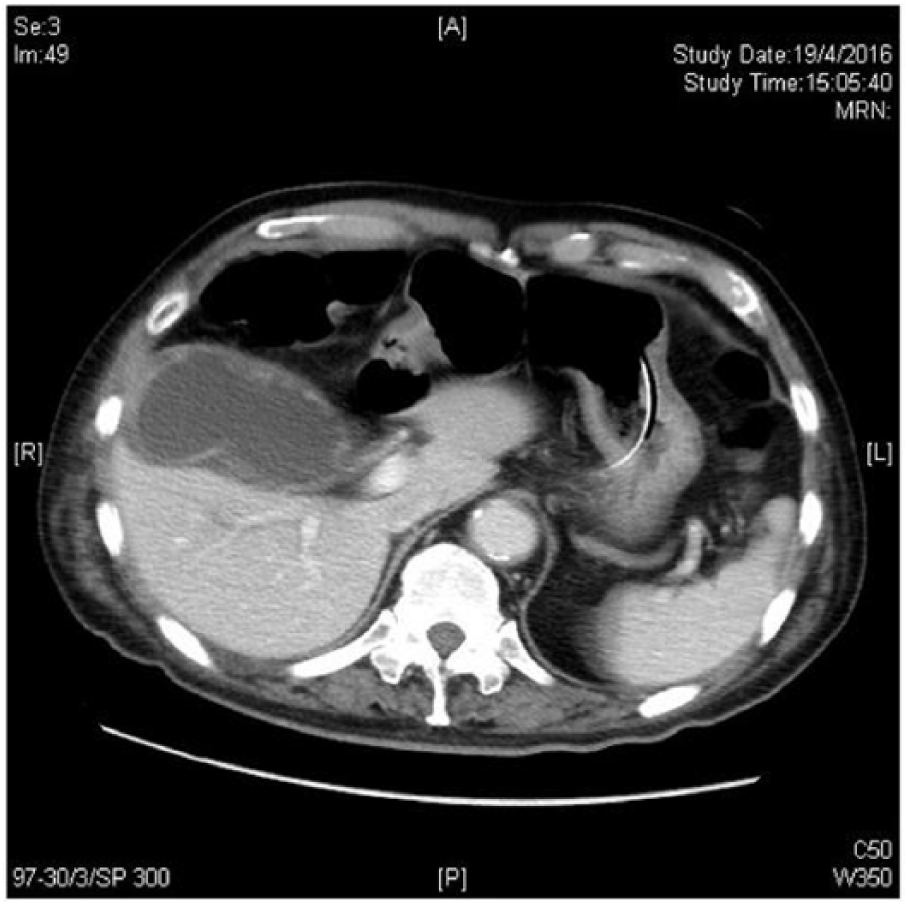
CT scan of the patient showing distended gall bladder with thickened gallbladder wall and patchy areas of increased enhancement.
Discussion
Salmonella are motile Gram-negative facultative anaerobic bacteria in the family of Enterobacteriaceae. The Salmonella genus consists of two species, S. enterica and S. bongori, with more than 2500 serotypes described in the genus, based on the difference in the somatic (O) and flagellar (H) antigen according to the Kauffman and White scheme. Most pathogenic strains causing illness in human belong to the S. enterica species. 3 Nontyphoidal Salmonella infection is caused by Salmonella species other than S. Typhi and S. Paratyphi. In Hong Kong, nontyphoidal Salmonella is the second most common bacterial food poisoning outbreak agent from 2009 to 2011. In 2010, the five most common species isolated locally were S. enteritidis (31.8%), S. typhimurium (16.1%), S. stanley (6.4%), S. derby (6.0%) and S. agona (2.5%). Clinical outcomes differ substantially by different serotypes; some serotypes such as S. dublin had a significantly higher rate of hospitalization, invasive infection and mortality compared to other serotypes. 4 Salmonella infection occurs mainly via ingestion of contaminated food products, most common being poultry, eggs and egg products. Salmonella infection may spread systemically via the blood stream resulting in invasive salmonellosis. Patients at extremes of ages with immunocompromised conditions, such as human immunodeficiency virus infection, diabetes mellitus, underlying malignancy and use of immunosuppressive medications, are at risk of invasive salmonellosis and complications from Salmonella infection. 5 Bacteraemia is one of the most common complications of Salmonella infection that occurs in 2% to 8% of patients with nontyphoidal Salmonella infection. 6 Salmonella has a tendency for wide dissemination in the body and causes focal metastatic infections by haematogenous seeding during the episode of bacteraemia which may result in meningitis, endocarditis, mycotic aneurysm, pneumonia, empyema, abscess formation, osteomyelitis and septic arthritis.
Although acute cholecystitis is a well-reported complication of typhoidal Salmonella infection, 7 GI complications from nontyphoidal Salmonella infection are uncommon.
Acute acalculous cholecystitis, a condition of an acute necroinflammatory disease of the gall bladder in the absence of gallstones, is typically seen in the critically ill patients and is associated with high morbidity and mortality rates. 8 It is recognized as a complication of serious medical and surgical conditions and is well reported to occur in patients after major surgery and patients with multiple trauma or burn injury. 9 Acute acalculous cholecystitis also develops in patients with sepsis and various bacterial infection conditions, including leptospirosis, 10 brucellosis, 11 typhoidal Salmonella, 12 and other diarrhoeal diseases, such as cholera 13 and Campylobacter enteritis. 14 However, acute acalculous cholecystitis caused by nontyphoidal Salmonella infection is rare, with a reported incidence of 0.6%. 15
The pathogenesis of acute acalculous cholecystitis is thought to be related to bile stasis and gallbladder ischaemia, resulting in a local inflammatory response in the gallbladder wall, concentration of bile salts, gallbladder distension and eventually necrosis of the gallbladder tissue. Once gallbladder ischaemia is established, secondary infection of the ischaemic tissue by enteric pathogens, including Escherichia coli, Enterococcus, Klebsiella, Pseudomonas, Proteus species and Bacteroides, occurs. Perforation develops in severe cases. 16 Rapid diagnosis and prompt surgical intervention are essential because gallbladder ischaemia progresses to gangrene and perforation very rapidly. 17
Acute acalculous cholecystitis often poses major diagnostic challenges as the clinical presentation is often subtle. In obtunded patients, the appearance of unexplained fever, leucocytosis or vague abdominal discomfort may be the only sign of acute acalculous cholecystitis. In some cases, jaundice or presence of right upper quadrant mass may occur. Jaundice typically results from sepsis-related cholestasis or partial biliary obstruction induced by inflammation extending into the common bile duct. It may also occur as a result of extrinsic compression of the common bile duct by a phlegmon (Mirizzi-type syndrome). 18 Laboratory test abnormalities may include leucocytosis or abnormal liver tests, but they are non-specific. 19 Since the presentation is often insidious and subtle, gallbladder necrosis, gangrene and perforation are frequently present at the time of diagnosis, manifesting as sepsis, shock and peritonitis.
Diagnostic imaging for acute acalculous cholecystitis includes USG and CT scan. USG is accurate to diagnose acute acalculous cholecystitis, and thickening of the gallbladder wall is the most sensitive diagnostic feature. Gallbladder wall thickness greater than or equal to 3.5 mm is diagnostic of acute acalculous cholecystitis with reported sensitivity and specificity of 80% and 98.5%, respectively. 20 Other USG findings of acute acalculous cholecystitis include absence of gallstones, presence of pericholecystic fluid or intramural gas and gallbladder distension of more than 5 cm in transverse diameter. 21 In addition, USG could also help to detect gallstones and measure the bile duct diameter. The diagnostic features of acute acalculous cholecystitis by CT scan are similar as USG. However, CT scan is particularly useful in patients with Salmonella infection with bacteraemia since endovascular complications such as mycotic aneurysm, which may not be apparent in USG, can also be detected by CT scan.
Treatments for acalculous cholecystitis include prompt initiation of antibiotics, cholecystostomy and cholecystectomy. Percutaneous cholecystostomy is the preferred option for critically ill patients with high perioperative risks. Most of the patients have clinical improvement within 48 h after the procedure.22,23
Failure to improve, as defined by persistent fever, ongoing sepsis or new evidence of multi-organ dysfunctions, may be due to gangrenous cholecystitis, catheter dislodgement, bile leakage resulting in peritonitis or an incorrect diagnosis of acalculous cholecystitis. Patient who fails to improve after drainage should consider complications from acalculous cholecystitis, including gangrenous cholecystitis, gallbladder wall necrosis with perforation or bile leakage, and emergency cholecystectomy is required. On the other hand, once the episode of acalculous cholecystitis has resolved, cholecystectomy is generally not required if the underlying problem is no longer present.
Conclusion
In summary, Salmonella infection is a common cause of food-borne illnesses in Hong Kong and can lead to various complications. Acute acalculous cholecystitis is a rare, but potentially lethal, complication of Salmonella infection. The clinical presentation of acute acalculous cholecystitis is often subtle; therefore, a high degree of suspicion should be maintained in managing patients with Salmonella infection and ongoing sepsis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All patients’ identifications were removed before storage. The master dataset was kept by the investigators in computer, and password was required to open the file. Access to the data would be limited to the investigators and clinical research ethics committees of Kowloon West Cluster, Hong Kong Hospital Authority. Please contact principal investigator if further information of the data is required.
Informed consent
The author was unable to obtain informed consent from the patient directly due to patient’s mental condition, verbal consent had been obtained from patient’s spouse and the paper will be published anonymously.
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.