
Abstract
Introduction:
Nocardiosis is a rare kind of opportunistic infections. Because of its insidious onset and atypical clinical manifestations, diagnosis and early treatment are often delayed.
Case presentation:
Here we present a 60-year-old Chinese female patient with systemic Nocardia infection, who had been diagnosed with idiopathic thrombocytopenic purpura previously and was misdiagnosed for up to 6 months prior to presenting at our hospital and ultimately achieved clinical cure.
Discussion:
The patient took prednisone because of ITP for several years which led to immunosuppression. Nocardia infection began from the skin rupture and then spread all over the body with multiple system involvement. The pus culture eventually found Nocardia. Sulphonamides have been the standard treatment for decades and there are several other options. Patients with severe Nocardia infection or immunosuppression are suggested a combined therapy.
Conclusion:
Nocardiosis is an infection that often resulted in delayed diagnosis because of lack of specificity of the clinical profile and the difficulty in culturing the bacteria. It should be included in the differential diagnosis of patients in which there are cutaneous, respiratory or neurological manifestations, especially in immunosuppressed individuals.
Introduction
Nocardia is a Gram-positive filamentous bacteria which grows aerobically. 1 It can be found in soil, air, water, decomposing vegetation and other organic matters and human contact, usually through contaminated soil, can cause infections by entering through the respiratory tract and skin wound. A considerable portion of the patients suffer from severe underlying disease, most commonly systemic lupus erythematosus (SLE) followed by nephrotic syndrome, organ transplantation, 2 tuberculosis, chronic lung disease, blood diseases, AIDS and so on. Clinically, nocardiosis can present as pulmonary infection in 70% of cases, followed by central nervous system (CNS) infection (the most common extrapulmonary manifestations), skin, 3 in addition to dissemination to other organs such as the liver, kidneys, muscles, tendons, bones, joints, eyes (keratitis), lymph nodes, thyroid, adrenals, pericardium, heart valves, mediastinum, peritoneum and even catheter-related infections.4,5 The key aspect of diagnosis is acquiring positive specimen culture or polymerase chain reaction (PCR) of 16SrRNA gene. 6
Here, we present a patient with idiopathic thrombocytopenic purpura (ITP), who was eventually diagnosed with systemic nocardiosis.
Case presentation
A 60-year-old Chinese female patient was admitted to the emergency department of our hospital 3 years ago because of high fever, severe jaundice and respiratory failure. She presented with a 6 months’ history of progressive skin infection on the lower extremities associated with late-onset intermittent fever, cough and shortness of breath in recent 40 days. 6 months ago, she repeatedly sought medical advice at local hospital. The initial diagnosis was “erysipelas”, unknown if confirmed via culture on account of the red nodules and swelling of right ankle. Her chest X-ray showed lesions which her doctors attributed to ordinary pneumonia. Penicillin was used intermittently during the first month. After a week or so when she got better, the local doctors changed penicillin for topical antibiotics. The lesions continued to recur. Her medical history included Graves’ disease, remote history of deep venous thrombosis and an 8-year history of ITP, which had been controlled for more than 1 year with daily continuous oral methylprednisolone (12 mg) and danazol (100 mg).
Upon admission to our ED, her blood pressure was 164/88 mmHg. Her pulse rate was 131 beats/min and the body temperature was 39.2°C. Physical exam was significant for scleral jaundice and scattered red nodules with ulcers on the the right thigh, right shoulder, right ankle and bilateral arms (Figure 1), from which purulent secretion could be expressed. Rales were heard almost throughout all lung fields and her heart rate was regular with no murmur. Abdominal examination was negative.
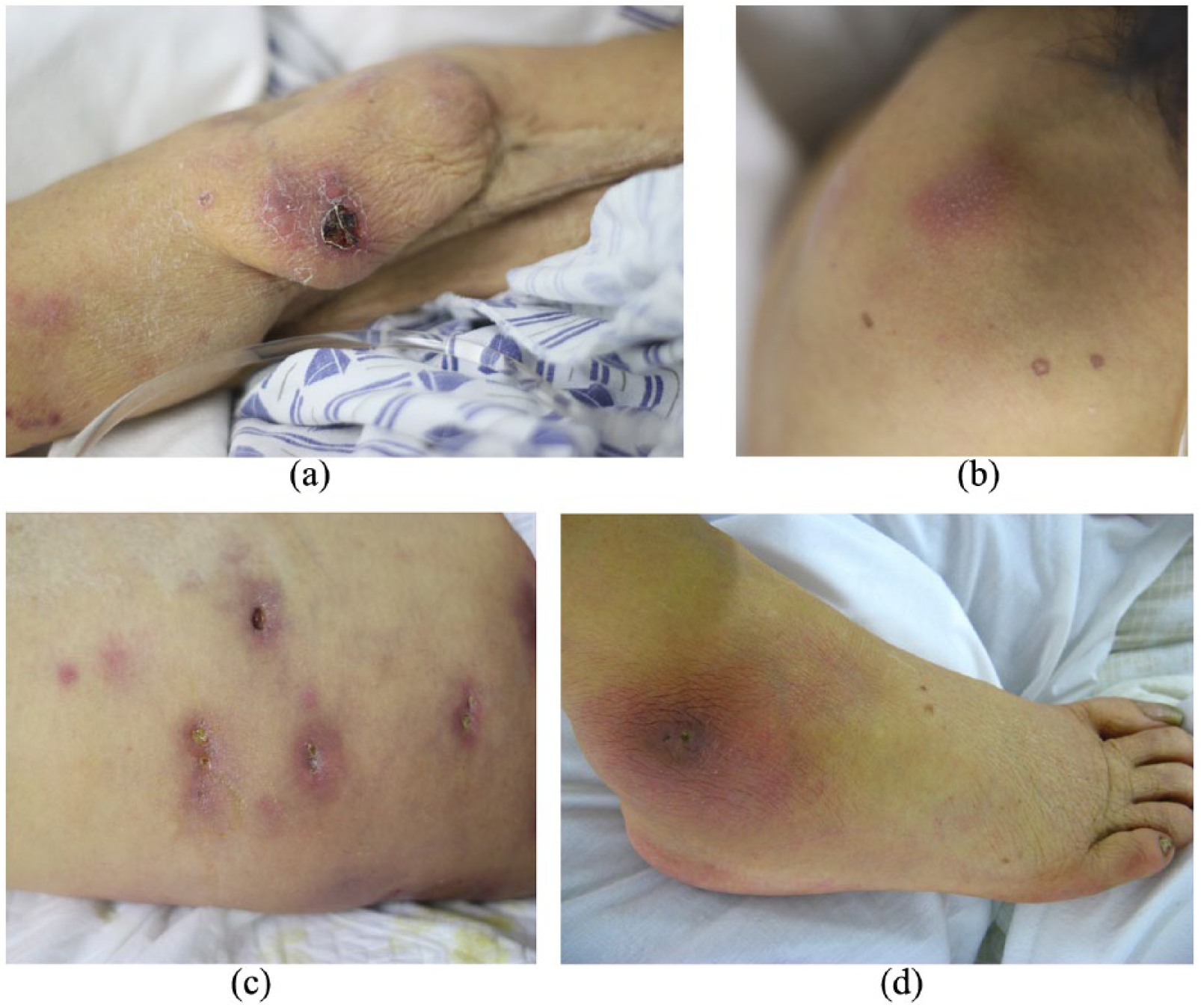
Skin lesions of (a) right arm, (b) right shoulder, (c) right thigh and (d) right ankle.
Her white blood cell count was 19.53 × 109/L, of which neutrophil was 96.7%. Platelet count was 219 × 109/L. Abnormal liver function, especially significantly increased bilirubin, was noticed (alanine transaminase (ALT) 72 U/L, aspartate aminotransferase (AST) 134 U/L, total bilirubin (TBIL) 150.8 µmol/L). Chest X-ray and computed tomography (CT) scan revealed multiple high-density nodules of varying sizes disseminated throughout both lungs, accompanied by opacity in most lesions.
We had analysed the reason of hyperbilirubinemia. Alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT) and direct bilirubin were all elevated. First, we had performed abdominal ultrasound and abdominal CT scan to rule out biliary obstruction and liver abscess. Second, we checked the hepatitis antibodies, which were all negative. Third, she did not have anaemia and there was no evidence for haemolysis. Then we thought it was drug-related bile stasis in hepatocyte, the most common reasons of which were ischaemia and drugs. We believed that hyperbilirubinemia was related to long-term use of androgen, which was terminated immediately and several hepatoprotective drugs including ademetionine and polyene phosphatidylcholine were used. Subsequently, her TBIL decreased from 150.8 to 89 µmol/L.
Purulent fluid was cultured from multiple skin nodules, which were found to have Staphylococcus hominis and Candida albicans. Later, the blood culture also confirmed Staphylococcus hominis bacteraemia, secondary to skin infection, which explained the sudden onset of fever. Because the G test was negative, Candida albicans was considered to be colonization or specimen contamination. Skin biopsy was performed in dermatology clinic and the pathologic diagnosis was panniculitis though, unfortunately, no tissue culture performed. Panniculitis with systemic disease can be caused by connective tissue disorders, lymphoproliferative disease, sarcoidosis or just skin infection. She presented with lesions involving multiple systems. Therefore, infectious, autoimmune, neoplastic diseases should be ruled out one after another. Other laboratory test results including G/GM test, T-spot, autoimmune antibodies and tumour markers were normal and the serology for human immunodeficiency virus was negative. Because of poor condition of the patient, CT-guided lung biopsy was not performed.
Her body temperature was still above 39°C with frequently occurring shiver. We started treatment as soon as the patient arrived. We were reminded of a previous patient who had nocardiosis because of leukaemia and chemotherapy. Their clinical course and CT manifestations were very similar. Because of the high probability of nocardiosis, we chose trimethoprim–sulfamethoxazole (TMP-SMX) and ceftriaxone as the initial antibiotic therapy immediately.
As a matter of fact, there was also a tender subcutaneous mass that did not attract our attention at the beginning. It had the dimensions of 7 × 8 cm2 with a well-defined border and was skin coloured, fluctuant and tender on the right waist which was believed to be a haematoma according to previous ultrasound. We decided to confirm that by puncturing with a large bore needle. In total, 75 mL of purulent fluid was drained (Figure 2). Smear with Gram stain and culture was performed on the aspirated fluid and the smear showed Gram stain positive. Pus culture proved Nocardia and susceptibility results showed that the majority of the commonly used antibiotics were sensitive. Unfortunately, due to limited laboratory facilities we failed to identify the subtype. Hence, we arranged a series of examinations to search for other abscess throughout the body. Ultrasound showed multiple enlarged lymph nodes on the left neck, the largest of which was 2.5 × 1.2 cm2, and a low-echo zone to the surface of the right femur, the range of which was about 11.1 × 2.6 cm2 with no blood flow signals. Moreover, culture of the purulent fluid from these abscess also showed Nocardia. Cardiac ultrasound also revealed moderate echogenic mass (21 × 21 mm2) on the atrioventricular groove and a small amount of pericardial effusion. The patient was submitted to a CT scan of the brain, which was normal. She had no headache and disturbance of consciousness. Meningeal irritation signs were all negative. There was no evidence of meningitis. To avoid the risk of bleeding during lumbar puncture, we decided not to do it.
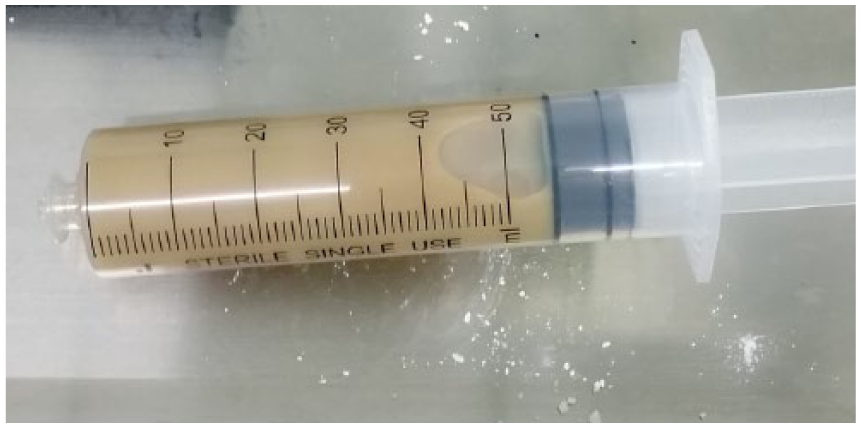
Purulent fluid drained from the abscess on the right waist.
We chose TMP-SMX plus ceftriaxone as the initial regimen, to avoid side effects of drugs including thrombocytopenia and impairment of the liver or kidney and to maintain a long course of treatment, taking into account the cost at the same time. Unfortunately, our patient did not respond well. Then we exchanged ceftriaxone for meropenem, then linezolid and achieved the resolution of the symptoms. After a month, the patient’s body temperature returned to normal. The patient was then treated with TMP-SMX (4.32 g/day) and minocycline (200 mg/day) for 4 months, resulting in the involution of the subcutaneous nodules and significant radiological improvement (Figure 3). Despite improvement of her infection, she unfortunately had a severe relapse of ITP, resulting in gastrointestinal haemorrhage 2 months later and died.
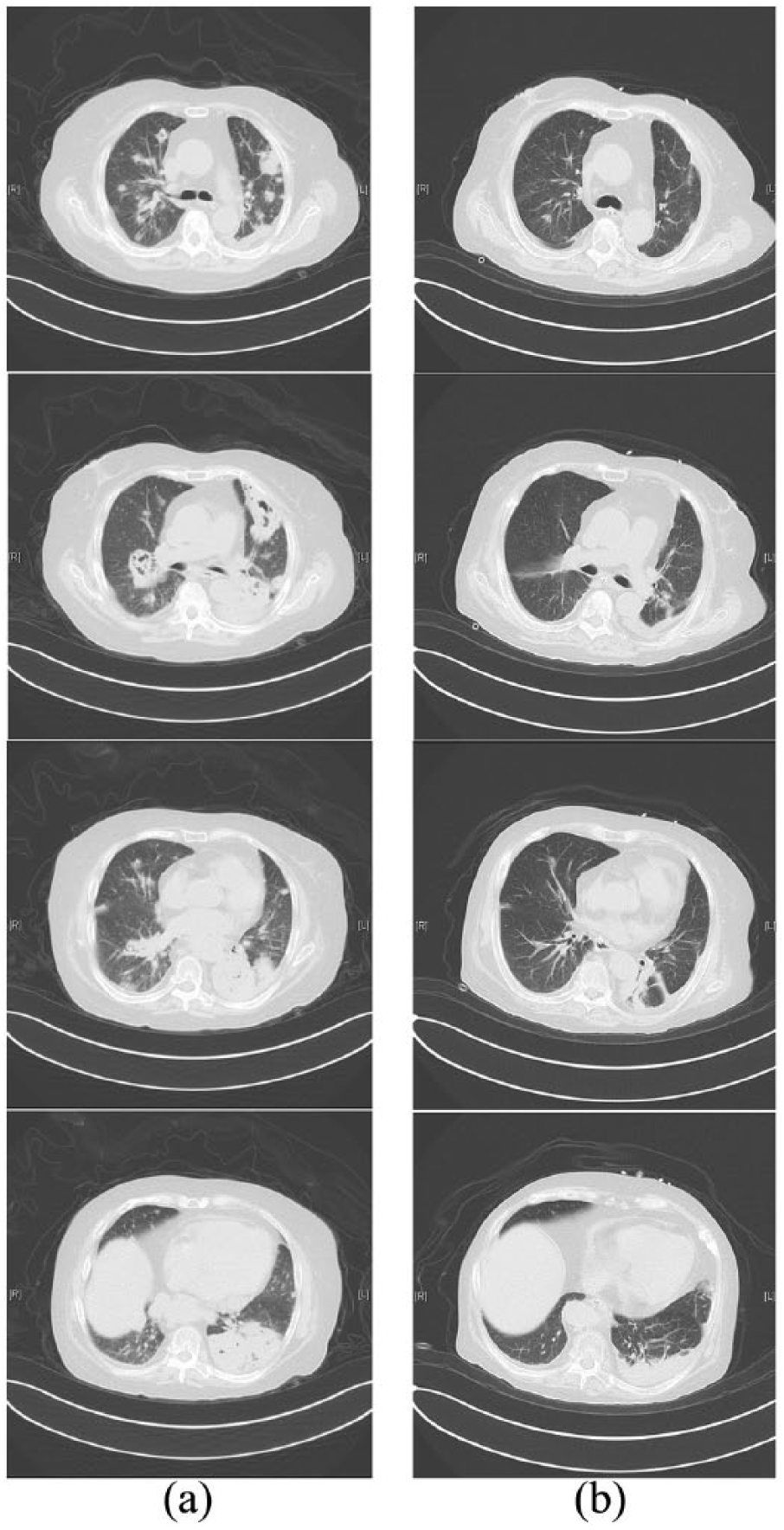
Lung CT (a) before and (b) four months after treatment.
Discussion
In this case, the patient took prednisone because of ITP for several years which led to immunosuppression. She lived in her bungalow in a very small village called Tuanshan, which is far from Beijing city. She did not have satisfactory oral hygiene or skin health and her rural, agricultural environment predisposed her to contract Nocardia infection. We believed that the Nocardia infection began from the skin rupture on her right ankle and then spread all over the body. She manifested multiple system involvement, with the most prominent feature of multiple abscess and lung infection. Although she visited the local hospital repeatedly due to skin lesions, the final diagnosis was delayed for 6 months because of neglected respiratory symptoms and lack of bacterial culture. Skin biopsy was once taken but no culture was performed. Infectious disease should be considered first based on overall clinical profile, especially opportunistic infection. Pathogen determination was essential. So, we acquired the specimens of sputum, skin ulceration secretions, blood and pus repeatedly for bacterial, fungal and tuberculosis (TB) culture. The pus culture eventually found Nocardia.
The most commonly used specimens are phlegm, bronchoalveolar lavage fluid (BALF), pleural effusion and percutaneous lung puncture to detect Nocardia infection. Bacterial smear is the most rapid method. By positive Gram staining and weakly positive acid-fast staining, doctors can make preliminary judgement of Nocardia infection, which has a good sensitivity. Bacterial culture and identification are the gold criteria for diagnosis. It is an aerobic bacterium that can grow on a non-selective medium. Because of slow growth, it takes 2 weeks for culture. But if the plate is contaminated by other bacteria, Nocardia may be covered by the other bacteria. In recent years, the diagnostic methods of molecular biology had been developed. By the detection of specific genes, we can distinguish it from other bacilli and identify the subspecies at the same time. The genes commonly used for detection are 16S rRNA and hsp65. But this method is currently confined to the laboratory and is not widely used in clinical practice.
Although the Clinical and Laboratory Standards Institute has published recommendations for antimicrobial susceptibility testing for Nocardia and other aerobic actinomycetes 7 , the prevalence of sulphonamide resistance has been debated in recent years. There have been no randomized clinical trials demonstrating the best therapeutic regimen. Sulphonamides have been the standard treatment for the last 50 years. Alternative antimicrobial agents include amikacin, imipenem, meropenem, ceftriaxone, cefotaxime, minocycline, moxifloxacin, levofloxacin, linezolid (nearly 100% antibacterial activity), tigecycline and amoxicillin clavulanic acid. Combination therapy may provide enhanced activity. 8 Patients with severe Nocardia infection or immunosuppression are suggested to combined therapy with more than two drugs. The total course of treatment is at least 6 months. Our patient took TMP-SMX and minocycline for 6 months. It has been reported to recommend prophylaxis with TMP-SMX routinely in immunosuppressed patients for the prevention of pneumocystis pneumonia. In order to reduce Nocardia, there are similar recommendations in the literature and continues to be under exploration. 9
Conclusion
Nocardiosis is an infection that often resulted in delayed diagnosis because of lack of specificity of the clinical profile and the difficulty in culturing the bacteria. It should be included in the differential diagnosis of patients in whom there are cutaneous, respiratory or neurological manifestations, especially in immunosuppressed individuals. It is important to evaluate the response to the initial treatment or adverse reactions and adjust the treatment plan according to susceptibility results.
Footnotes
Acknowledgements
Thanks to all faculties in EICU of Emergency Department of Peking University Third Hospital who have been involved in daily diagnosis, treatment and especially skin care of the patient. The manuscript is submitted for consideration on consent given by all contributing authors. The manuscript has been submitted solely to this journal and is not published, in press or submitted elsewhere. The authors disclose any prior posting, publication or distribution of all or part of the manuscript to the Editor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
All the information of the patient is available from the electronic medical record system of our hospital and cannot be legally or ethically uploaded here.
Informed consent
The patient died. A written informed consent was obtained from the patient’s legally authorized representative (her son) for her anonymized information to be published in this article. See Supplementary File.