
Abstract
Brown recluse spider (Loxosceles reclusa) envenomations with subsequent necrotic skin lesions occur infrequently, and systemic loxoscelism is rarer still. We report a case of 2 successive developing necrotic lesions, each on adjacent medial aspects of the legs, secondary to presumed Loxosceles envenomation. A 31-year-old man with no significant past medical history presented to the emergency department with 2, large, necrotic lesions, 1 on each medial thigh. They had progressed over the course of 1 month from small blisters to large necrotic lesions with eschar. He underwent surgical debridement without skin grafting with no further complications. Bites from recluse spiders that progress to necrosis usually present as single lesions. The differential diagnoses for a necrotic skin lesion is large. The presence of more than 1 lesion argues against Loxosceles envenomation; however, in the absence of underlying infection, systemic diseases, immunodeficiency, or malignancy, the diagnosis must be considered if the case presents in an endemic area. Brown recluse spiders rarely bite multiple times, thus confounding the diagnosis of an already nonspecific clinical finding.
Introduction
The incidence of envenomation from the brown recluse spider (Loxosceles reclusa) is low, despite the effects being well described. Of the 1495 brown recluse bites reported to the American Association of Poison Control Centers in 2010, there were 562 that were seen in a healthcare facility, and only 14 reported major complications. There were no deaths. 1 The passive nature of the spider, limited geographic range of the species (Figure 1), and individual susceptibility explains the rarity and variability of clinically significant spider bites.2,3 Additionally, the medical literature includes numerous indeterminate cases, and even cases reported to local poison control centers may be suspect. 4 The likelihood of a single patient exhibiting multiple necrotic lesions from multiple simultaneous envenomations is lower still. In 2006, Nunnelee 5 described the only case of multiple concurrent lesions secondary to brown recluse envenomation in the medical literature. We report a case of presumed Loxosceles envenomation resulting in necrotic ulcers with eschar each on adjacent medial aspects of the legs after 2 separate but temporally related bites. To our knowledge, a case has never been described in which the spider bites 1 limb, and shortly thereafter a different limb on the same patient.
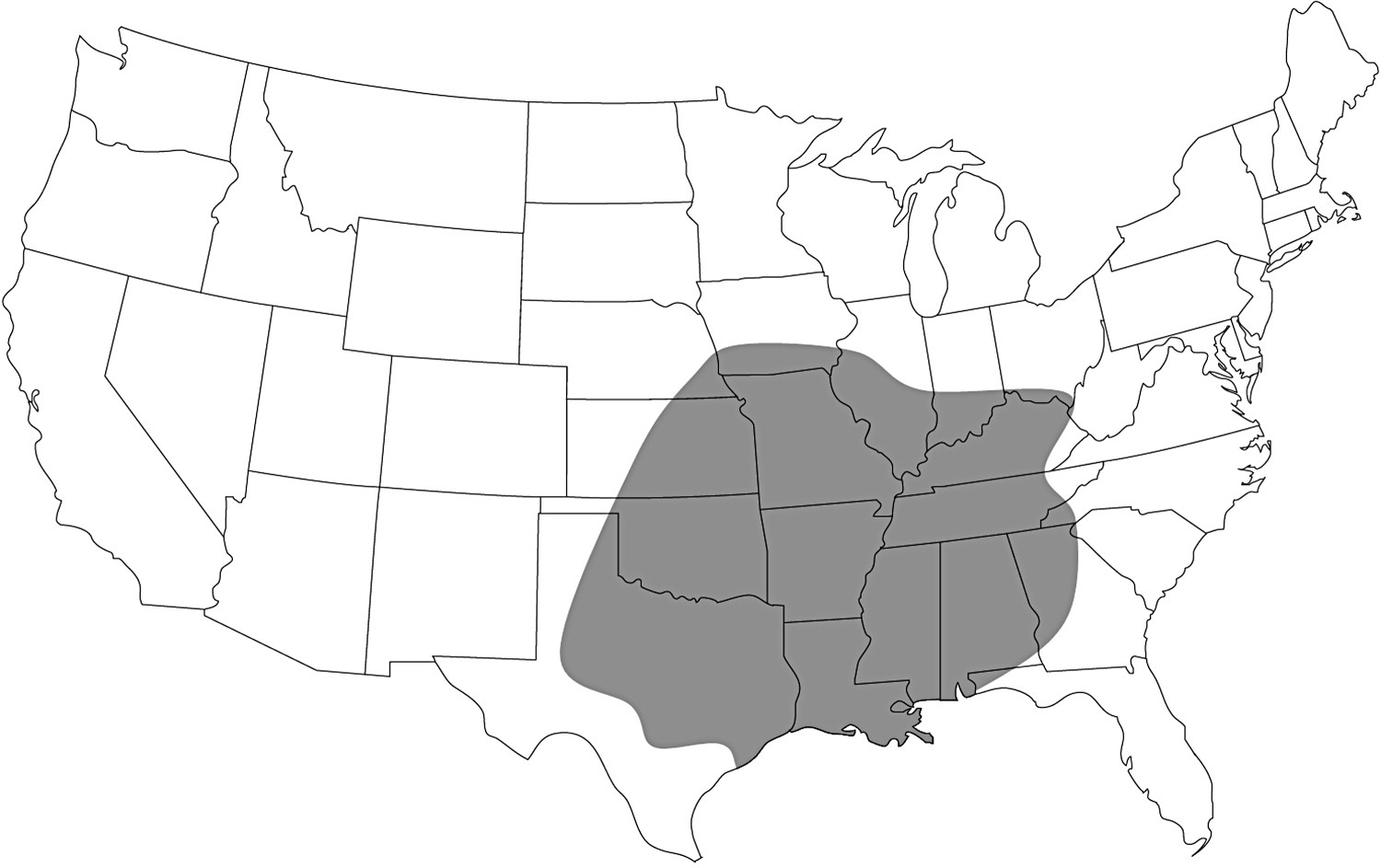
Endemic range of L reclusa.
Case Report
The patient was a 31-year-old African American man who presented to an emergency department (ED) in western Missouri with 2 large necrotic lesions on his medial thighs. One month earlier, he had noticed 2 small blisters, 1 on each medial thigh, each about 1 cm in diameter, with associated redness and pain. One day after their appearance, the blisters opened spontaneously, the area of redness enlarged, and the pain increased. The patient then presented to an outside facility and was treated for cellulitis with a course of cephalexin. No initial wound cultures were taken. One week later, the pain and redness had not improved, and the blisterlike lesions continued to enlarge. The patient returned to the same ED, where he was then prescribed a course of trimethoprim/sulfamethoxazole. The patient reported finishing both courses of antibiotics. He then came into our ED because the lesions had ulcerated and grown substantially.
On examination, we noted 2 lesions, 1 on the medial aspect of each thigh (Figure 2). The lesions were not symmetrical. The lesion on the right thigh (Figure 3) was 12 cm by 8 cm, with eschar measuring 10 cm by 4 cm. The lesion on the left thigh (Figure 4) was 15 cm by 10 cm, with eschar measuring 8 cm by 3 cm, and was slightly inferior in comparison to the right lesion. Both were similar in appearance: blackened eschar centrally, with surrounding areas of erythematous ulcerated tissue. The epidermis around the ulcerations was thickened, had minimal erythema, and did not blanch with pressure. There were no areas of fluctuance. The wounds were minimally tender, with reduced sensation centrally. Acute pain resulted from instrumentation of the peripheral edges of the lesion. The patient also reported diffuse paresthesia surrounding each lesion, with a cramping feeling in the muscles of his thighs. He denied previous fever, rash, arthralgias, vomiting, or hematuria. He also denied observing a spider. The remainder of his review of systems was normal. His vital signs were normal, and the remainder of his physical examination was unremarkable. His body mass index was 28.8 kg/m2. A complete blood count, electrolyte panel, urinalysis, and coagulation panel were all normal. Creatinine kinase was slightly elevated at 498 IU/mL. A medical toxicologist was consulted, who evaluated the patient and concurred with the assessment of a brown recluse envenomation. The patient declined a skin biopsy, but a swab culture was obtained and subsequently suggested contamination with normal skin flora.

Bilateral thigh lesions.

Detail of right lesion.

Detail of left lesion.
The patient was discharged with pain medication, supplies for wound care, and a follow-up appointment in the surgery clinic for wound debridement. At this follow-up appointment, there was no noticeable increase in the size of the lesions or change in his symptoms. Wound debridement was performed without skin grafting, and the patient has suffered no further complications.
Discussion
This is an unusual and unexpected presentation of a well-described phenomenon. Reactions to brown recluse spider bites are variable, ranging from minor skin irritation to systemic loxoscelism. 2 Although single necrotic wounds are a known complication of brown recluse bites, development of 2 concurrent lesions is an unusual phenomenon and has only been reported once previously. Nunnelee 5 described a 32-year-old man with 2 wounds on his right upper arm that progressed to necrotic lesions. The patient underwent debridement and skin grafting at week 7. The initial wounds were within several centimeters of each other, thus raising the possibility that the wounds were a result of the same single envenomation, and not 2 separate wounds as initially believed. 5
Brown recluse spider venom is a complex mixture of various enzymes and glycoproteins. The main constituent of the venom that is responsible for the pathophysiologic effects is sphingomyelinase-D. This enzyme inserts into the lipid membrane, rendering the cell susceptible to the complement system. 6 It also stimulates platelet aggregation, release of inflammatory mediators, and activation of polymorphonuclear cells. These effects result in the development of necrotic wounds. Likewise, this cascade of events can result in systemic loxoscelism. Severity of symptoms in the patient is dependent on the gender and species of Loxosceles. 3
Cutaneous loxoscelism manifests as pain, erythema, pruritus, or blister formation that begins within several hours of envenomation. Wounds may evolve for several days or 2 weeks and are characterized by edema, induration, or ulcer and eschar formation. Frank necrosis may or may not occur. Healing typically occurs over the course of several weeks to months. Systemic loxoscelism may result in fever, systemic rash, vomiting, and myalgia. Life-threatening manifestations of systemic disease include hemolytic anemia and disseminated intravascular coagulation. 2 These serious complications are rare, even in areas where Loxosceles species are endemic. At our institution, 10 cases occur per year requiring transfusion owing to hemolysis.
The diagnosis is clinical, and there are no confirmatory laboratory tests available at this time. Positive identification of the offending spider (Figure 5), a requirement for a confirmed diagnosis, occurs infrequently. 7 The differential diagnoses for necrotic skin lesions is large, and includes cellulitis, contact dermatitis, anthrax, Lyme disease, herpetic infection, toxic epidermal necrolysis, ecthyma gangrenosum, pyoderma gangrenosum, pyogenic gangrenosum, sporotrichosis, vasculitis, vascular insufficiency, Martorell ulcers, diabetic ulcers, pressure ulcers, erythema nodosum, medication reactions, thermal burns, tularemia, and Chagas disease. 8 –10 Many of these often present with multiple lesions. However, our patient had no recent travel and was a long-term resident of the area. He had no recent ill contacts, was not taking any medication, and had no history or clinical evidence of immunological, endocrine, or rheumatologic disease. He had no history of methicillin-resistant Staphylococcus aureus and had never served in the military or been incarcerated. He had already completed 2 courses of antibiotics and displayed no signs of continuing infection. The lesions were not symmetrical, which argues against contact dermatitis, and there were no burns or trauma to the area. The lesions developed in the summer, when recluse spiders are more active. 11 The clinical presentation and absence of other etiologies, along with the fact that the patient lives in a region where brown recluse spiders are endemic, reduces the likelihood of misdiagnosis in this case. 10

Brown recluse specimen. Note the distinguishing features of L reclusa: 6 eyes in 3 pairs of 2, and the finely haired exoskeleton without course bristles. Coloration is rusty brown, and many specimens feature a darker stripe along the abdomen. The classic violin-shaped marking is not always apparent.
Treatment is supportive. Typical wound care is sufficient as most cutaneous wounds do well with conservative management. Other therapies including steroids, dapsone, and hyperbaric oxygen have not shown definitive benefit and are not recommended.12,13
In conclusion, brown recluse envenomation can rarely result in multiple, successive cutaneous necrotic lesions. Within endemic areas, the diagnosis of cutaneous loxoscelism should be considered in such cases after excluding other etiologies.
Footnotes
No grant money or sources of funding have been applied to the preparation of this case report.