
Abstract
An adolescent victim of an urban snakebite developed respiratory failure, rhabdomyolysis and consumption procoagulopathy but recovered with two vials of tiger snake antivenom administered after a delay of 48 hours. The clinical significance of a post-bite collapse was not initially appreciated. Tiger snake (Notechis spp.) venom antigen was measurable in blood before antivenom but not after whereas antivenom was measurable in blood for nine ensuing days. This case adds to growing evidence that further pharmacokinetic research of venom-antivenom interaction is required to establish the correct dose and timing of tiger snake antivenom. Antivenom therapy, even when delayed, facilitates recovery from snake envenomation.
Keywords
Introduction
The venoms of species of Australian tiger snakes (Notechis spp.) contain numerous toxins including procoagulants and multiple neurotoxins. 1 The principal neurotoxin, notexin, is a phospholipase A2 and causes rhabdomyolysis with large increases in serum creatine kinase (CK) levels 2 up to 600,000 international units/litre. 3 The procoagulant is a prothrombin activator similar to coagulation factor Xa. Although the clinical onset of procoagulopathy is rapid (within minutes), the onset of paralysis and rhabdomyolysis is usually slow (over hours). Recovery from rhabdomyolysis is determined by the regeneration of tissues provided the toxin has been neutralised. The pharmacokinetics of notexin are largely unknown but this case of delayed treatment with antivenom shows that venom may be detected in blood 48 hours after envenomation.
Case report
An adolescent felt pain in one foot while relaxing during a warm evening in a garden in metropolitan Melbourne. The victim experienced an ‘unconscious collapse’ but recovered quickly. A snake was not seen but the victim recalled seeing one in the garden earlier in the day. In the emergency department of a metropolitan hospital, a diagnosis of snake envenomation was considered unlikely. The victim was discharged home after observation for several hours and no tests were performed. Over the ensuing 24 hours the victim developed increasing foot pain accompanied by lethargy, hoarse voice, difficulty swallowing, slurred speech, blurred vision and sore neck muscles. The victim was transported by ambulance to another metropolitan hospital where clinical examination identified reduced muscle power, absent lower limb reflexes and ophthalmoplegia. Central nervous system infection was considered the likely diagnosis and treatment with dexamethasone, cefotaxime and acyclovir was commenced. However, a diagnosis of snake envenomation was determined when the victim’s serum CK level was reported as 21,000 IU/l (normal range 40–240 IU/l). The National Poisons Information Centre was consulted. Advice was received that because the opportunity to administer antivenom had lapsed, such treatment would not be beneficial and was not recommended. In addition, it was opined that no further neurological deterioration was expected and that treatment should be directed at supportive management of rhabdomyolysis.
The victim was transported to the paediatric intensive care unit (PICU) of the Royal Children’s Hospital (RCH), arriving 28 hours after the estimated bite time. On arrival the victim had inadequate airway protection due to bulbar palsy, had poor muscle power with a weak cough and hypoventilation, had a tender calf (but no signs of compartment syndrome) and dark urine. A purpuric lesion with surrounding erythema was present over the foot. Initial treatment consisted of endotracheal intubation, mechanical ventilation and forced alkaline diuresis. The first CK level was 53,000 IU/l and continued to rise. A mild-moderate consumption coagulopathy with fibrinolysis was present with a serum fibrinogen 1.1 g/l (normal range 1.5–4.3 g/l) and D-Dimer >20 µg/ml (normal level <0.40 µg/ml). The initial blood International Normalized Ratio (INR) was 1.3 (normal range 0.8–1.2) and activated partial thromboplastin time 31 seconds (normal range 27–44 seconds). A snake venom detection kit (Seqirus Australia Pty Ltd, Kings Park, New South Wales) test of the urine was negative. The National Poisons Information Centre was again consulted but the same advice to withhold snake antivenom was received.
At 48 hours after the bite, because the serum CK level had attained 65,000 IU/l two vials of Tiger Snake Antivenom™ (6000 units, Seqirus Australia Pty Ltd) were administered, preceded and followed by withdrawal of blood samples for venom and antivenom detection. 4 Samples withdrawn at 36 hours and at 48 hours after the bite but before administration of antivenom contained tiger snake venom (TSV) antigen at concentrations of 4.1 and 2.8 ng/ml respectively (limit of detection <0.15 ng/ml). TSV antigen was not detectable in serum 12 hours after the administration of antivenom. Serum antivenom was initially assayed at 547 mU/ml at 12 hours after its administration and declined steadily over nine days to 61 mU/ml.
Following antivenom therapy, the victim’s CK level increased briefly to 72,000 IU/l and then declined progressively below 5000 IU/l at 3–4 days and below 600 IU/l at ten days after antivenom whereas the serum alanine aminotransferase level peaked at around three days after envenomation and thereafter declined (Figure 1). The serum fibrinogen remained below the normal range (Figure 2) and INR above the normal range until after antivenom was administered. The victim’s clinical condition improved slowly. Forced alkaline diuresis was given for four days and renal function remained intact. Muscle weakness improved gradually day by day after antivenom but intubation for bulbar palsy and mechanical ventilation for respiratory failure was required for nine days. At four weeks after antivenom, the victim’s forced vital capacity was 66%. A trial of anticholinesterase therapy (neostigmine) after six days of mechanical ventilation had no beneficial effect on ptosis. The victim was discharged from PICU 11 days after presentation and discharged home from hospital after 14 days and has physically recovered well. Magnetic resonance imaging of the brain five days after presentation to RCH revealed no abnormality. Parental permission was given for publication of this report.
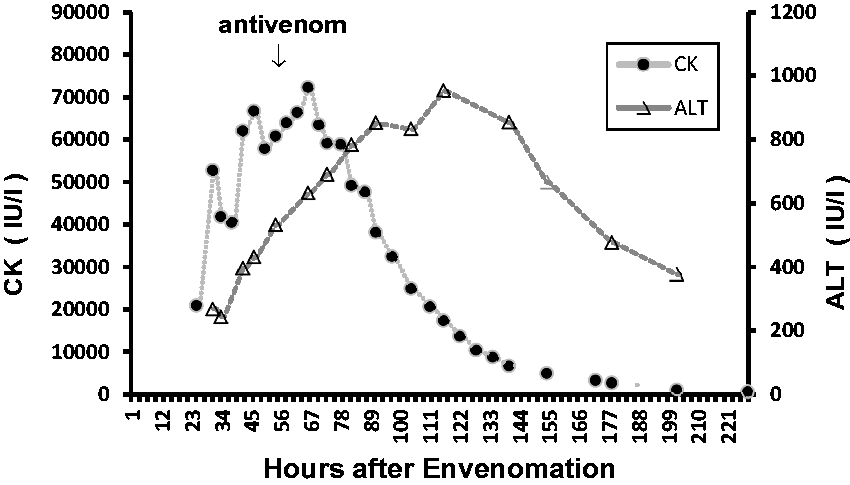
Serum creatine kinase and alanine aminotransferase levels.
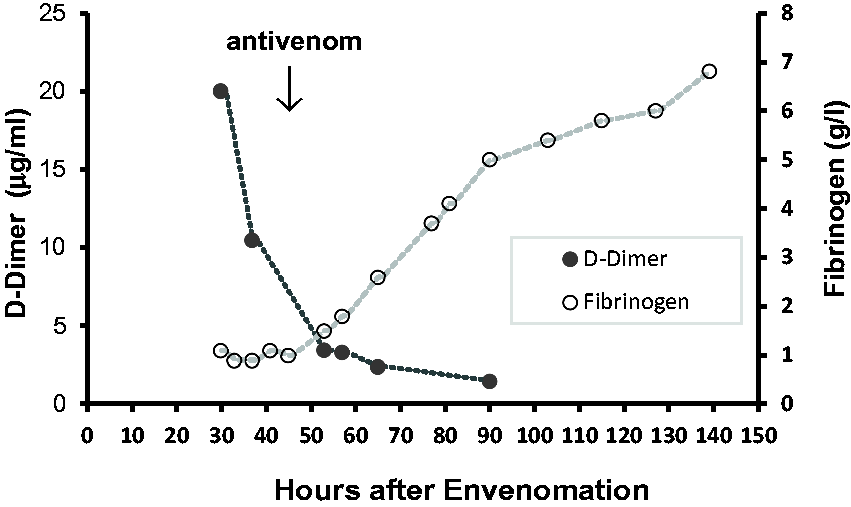
Serum D-Dimer and fibrinogen levels.
Discussion
This case and its medical management raise important issues in the management of snake bite.
Suspicion of snake bite and envenomation
At approximately 3000 bites per year, snake bite in Australia is uncommon with a death rate of about 1/1000 bites. 1 The bite of an Australian elapid snake may go unnoticed and even if a bite site is identifiable, a state of envenomation may not develop because venom may not be injected. Nonetheless, a high index of suspicion is required because fatalities after unrecognised snakebite have occurred in children who presented with non-specific symptoms. 5 After recognised snakebite, if no symptoms or signs are present on examination, a period of observation and a laboratory test of coagulation is required to exclude envenomation. 1 Coagulopathy is a reliable test of envenomation in all locations in Australia except where there is a possibility of bite from a death adder (Acanthophis spp.), whose venom is not significantly coagulopathic. Early collapse, with or without spontaneous recovery, is associated with significant envenomation and is probably related to the rapid onset of procoagulopathy. 1
Delayed diagnosis in this case contributed to subsequent development of severe complications. This case also demonstrates that snakebite is not only a rural phenomenon--severe and even fatal cases can occur in urban settings, in temperate as well as tropical Australia.
Withholding antivenom
In an envenomated patient, withholding antivenom is only justified if the risks of its administration outweigh its potential benefits. Unfortunately, our knowledge of the pharmacokinetics of specific venom toxins, of antivenom antibodies and of toxin-antibody interactions is limited. Moreover, it is not yet possible to rapidly and routinely measure the concentration of venom toxins in bodily tissues. What little information is available suggests that snake venoms, when uninfluenced by antivenoms, have an elimination half-life of approximately ten hours. 6 Thus in this case, 24 hours after the bite, a substantial proportion of the venom (approximately 25%) would have remained. In any case, TSV was identified in the victim’s blood 48 hours after the bite in a concentration equivalent to the median in 50 severely envenomated victims, albeit measured with a different method. 2 Although 48 hours appears to be the latest timepoint yet recorded for venom detection in a case of Australian elapid envenomation, it has been reported this late in other snakebites. 6
Snake antivenoms are preparations of foreign proteins and pose a risk of immediate and delayed allergic reactions. In the Australian Snakebite Project, the incidence of adverse reactions to tiger snake antivenom among 59 victims was 41% of which six (10%) were severe but non-fatal anaphylaxis. 7 It would be appropriate to withhold antivenom if the effects of envenomation were not life-threatening or so mild that spontaneous recovery could be expected but in this case, the effects were serious and life-threatening.
Choice of antivenom
In Victoria, a combination of brown snake and tiger snake antivenom effectively neutralises the venoms of all dangerous species. 1 In early envenomation it is difficult to differentiate the syndromes caused by bites of the eastern brown snake (Pseudonaja textilis) and the tiger snake (Notechis scutatus) because both cause procoagulopathy and paralysis. However, because brown snakes do not cause rhabdomyolysis, the occurrence of rhabdomyolysis recognised late in this case permitted the restriction of treatment to tiger snake antivenom.
Dose of antivenom
Eventually the victim was treated with two vials of TSV. This is more than that recommended by the claimed outcome of the Australian Snakebite Project in which only a single vial is recommended for all types and all severities of snake envenomation. 8 It has been argued elsewhere9–14 that a single vial is insufficient as a routine initial dose and that it should be two vials. 9 This is particularly so in the case of victims with higher than usual venom concentrations and/or delayed presentations.
Correction of procoagulopathy
Procoagulopathy cannot be reversed with antivenom but this treatment permits hepatic restoration of coagulation factors consumed in venom-induced procoagulopathy. However, an interval of at least six hours is required for restoration of coagulation after venom neutralisation. Replacement of coagulation factors, usually with fresh frozen plasma, is usually not necessary unless haemorrhage is present. In this case the consumption coagulopathy, accompanied by endogenous fibrinolysis, was relatively mild and did not require treatment with coagulation factors.
Treatment with anticholinesterase
Although an anticholinesterase may reverse or ameliorate postsynaptic neuromuscular blockade in envenomation by Australian or Papuan New Guinean death adders (Acanthophis spp.), 1 , 15 , 16 such treatment would not be helpful in the management of dense neuromuscular paralysis caused by the presynaptic neuromuscular blockade of tiger snake envenomation. Notexin destroys the axolemma of the synaptic junctions and synaptic vesicles as well as cellular organelles. 1 Although TSV also contains postsynaptic neurotoxins (which may be reversible with antivenom), an anticholinesterase would not be able to release acetylcholine from presynaptic membranes destroyed by notexin. If an anticholinesterase is used, it should be accompanied by atropine to prevent bradycardia.
Snake venom detection kit test
This is an in vitro enzyme-linked immunosorbent assay test of venom in biological samples. It can detect venom down to a concentration of 10 ng/ml and is designed to indicate which antivenom to administer to an envenomated victim. 1 It differentiates the venoms of the five main groups of snake genera (brown, tiger, death adder, taipan and black). However, its accuracy is operator dependent 17 and, as with all tests, may provide false positive and false negative results. In this case, based on symptoms, signs and serum CK levels, it was clinically probable that the victim had been envenomated by a tiger snake.
Conclusions
It is impossible to accurately specify the duration after snake envenomation that antivenom would be ineffective. However, this case of delayed administration of antivenom shows that venom may, in untreated cases, be still present in blood in substantial concentration at 48 hours and antivenom therapy, even when delayed, is beneficial in limiting rhabdomyolysis and assisting in restoration of coagulation. This case adds to growing evidence that further research of the pharmacokinetics of venom and antivenom is required to establish the correct dose and timing of tiger snake antivenom.
Footnotes
Acknowledgements
We thank the Australian government’s National Health and Medical Research Council for funding support to Dr Winkel and Seqirus for funding support to the Australian Venom Research Unit medical advisory service at the time of this case. None of these organisations had any role in the analysis or write up of this case.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.