
Abstract
Mosquito-borne diseases are global problems. The use of topical insect repellents is a key measure recommended by health authorities to prevent mosquito-borne diseases. Despite more than a hundred commercial products available in the market, there are relatively few active ingredients used across these formulations. The most common active components are diethyltoluamide, picaridin, p-menthane-3,8-diol, ethyl butylacetylaminopropionate (IR3535) and a range of plant-derived products. Research has shown that each of these active ingredients vary in the duration of protection provided against biting mosquitoes. However, the wide spectrum of commercial preparations and various recommendations from different health authorities make it a challenge to pick an effective product for end users as well as healthcare personnel. A local market survey was conducted to assess the mosquito repellent formulae in available products in Hong Kong, and a review of the current recommendations issued by local and overseas authorities on choosing the suitable insect repellents is performed with consideration of recent research and currently available topical repellents in the market.
Introduction: the clinical situation and question
Traveling across the globe is very common nowadays. Worldwide travelers are susceptible to different kinds of mosquito-borne diseases, including malaria, dengue and Zika. Malaria is endemic mainly in Africa, Asia and the Americas. In Hong Kong, annual malaria notifications ranged from 20 to 55 cases since 1998. The majority of these cases were imported from outside Hong Kong. 1 Special attention was paid to dengue fever in Hong Kong. According to data from the Center for Health Protection (CHP), 99 cases of dengue fever were confirmed in 2017, including one local case, compared with 119 imported cases in 2016.2,3 Dengue fever is now endemic in more than 100 countries in Africa, the Americas, the Eastern Mediterranean, Southeast Asia and the Western Pacific. This includes popular tourist destinations for Hong Kong people including the Philippines, Thailand, Indonesia, Malaysia and Singapore. 4 Recently, outbreaks of Zika virus infection have been recorded in Africa, the Americas, Asia and the Pacific. In Hong Kong, one imported case and two imported cases of Zika virus infection was reported in 2017 and 2016, respectively. 5 As recommended by Port Health of Department of Health in Hong Kong, travelers who returned to Hong Kong sick and feverish would seek medical attention, most likely from one of the Accident and Emergency Departments.
As emergency physicians, our duty lies beyond making the correct diagnosis and providing timely treatment. We are also obliged to offer advice to out patients for preventing mosquito-borne disease in the future. We may be faced with a common clinical scenario: A 30-year-old lady who recovered from an episode of dengue infection will be discharged from the Emergency Medicine Ward. Which insect repellent would you recommend in order to lower the risk of dengue hemorrhagic fever in the future?
A vast amount of information regarding the use of insect repellents is readily available on the Internet, be it from commercial sources or health authorities. However, inconsistencies between the recommendations and available repellent formulations may cause confusion in the community. A local market survey was thus designed to understand the active ingredients contained in the insect-repellent products on the market and to compare the findings with current recommendations issued by local and overseas health authorities. These results will shed light on how to choose effective insect repellents.
Local market survey of insect repellents
Methodology
This local market survey was conducted by three emergency physicians from 6 to 11 October 2017 in the Hong Kong Special Administrative Region (HKSAR). A sample of items was selected from local retail stores, including supermarkets, outdoor gear shops, department stores, convenience stores, local pharmacies and cosmetics stores, and local online stores. Visits to physical stores by the emergency physicians was limited to Wan Chai and Causeway bay, which are two main shopping centers and commercial areas in the HKSAR. The online stores were identified via the Google search engine. Items with wordings illustrating their use as topical mosquito repellents were included. Non-topical mosquito repellent products, including those in the form of wristbands and patches, those used on clothing and outdoor gear, and area repellents such as lanterns and coils, were excluded. Brand name, place of origin, form, active ingredients with their corresponding concentrations, and protection duration of each individual selected item were recorded. Data were entered into an excel file and analyzed by the three emergency physicians by using descriptive statistics.
Result
In all, 113 topical insect repellents were included in this study from the methodology described above. They were from different places of origins, including the United States, the United Kingdom, Hong Kong, Italy, China, Australia, Japan, Netherlands, and so on. Among the 113 topical insect repellents, 40 (35%) were synthetic, 70 (62%) were natural, and 3 (3%) contained both synthetic and natural active ingredients (Chart 1). Among the 33 synthetic repellents, 25 (64%) were N,N-diethyl-m-toluamide (DEET), 7 were picaridin (18%), 1 was ethyl butylacetylaminopropionate (IR3535) (3%) and 6 (15%) were p-menthane-3,8-diol (PMD) (Chart 2). The concentrations of DEET in different formulations ranged from 6% to 95%. In all, 19 of 25 DEET products contained DEET 20% or more, in which 5 of them is 50% or above (Chart 3). The concentrations ranged from 9% to 25% for picaridin and 20% to 75% for PMD. The concentration of IR3535 in the formulation found was 20%. One synthetic repellent contained both DEET and PMD. Of those, three contained both synthetic and natural active ingredients, two contained picaridin and one contained IR3535. Natural active ingredients included citronella (found in 59% natural repellents), peppermint (43%), lemongrass (36%), cedar (26%), rosemary (13%), red tomato extract (9%), clove (4%), cedar (4%), caster (1%) and so on. Among the 70 natural repellents, 10 contained citronella only and 2 contained lemongrass only, while the remaining ones (58/70) contained more than one natural oil. In all, 5 of the 70 natural repellents only labeled “natural essential oils” without clearly stating the ingredients. In all, 5 of the 113 topical insect repellents were combined with sunscreen.
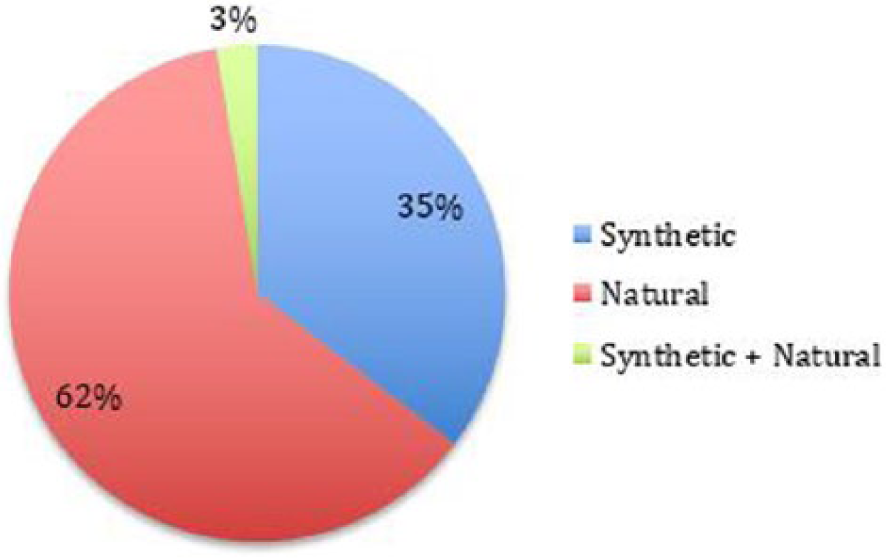
Distribution of synthetic “vs” natural insect repellents.
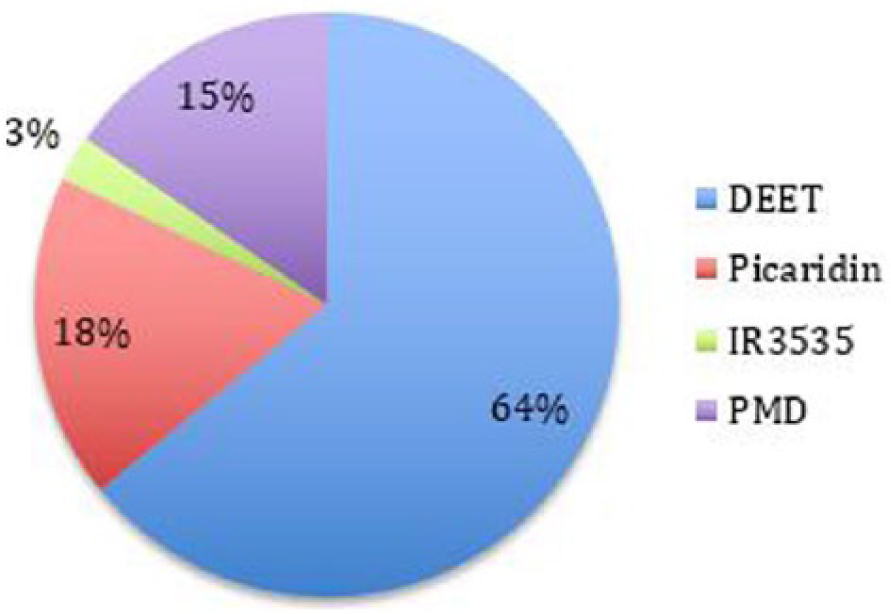
Distribution of active ingredients in synthetic insect repellents.
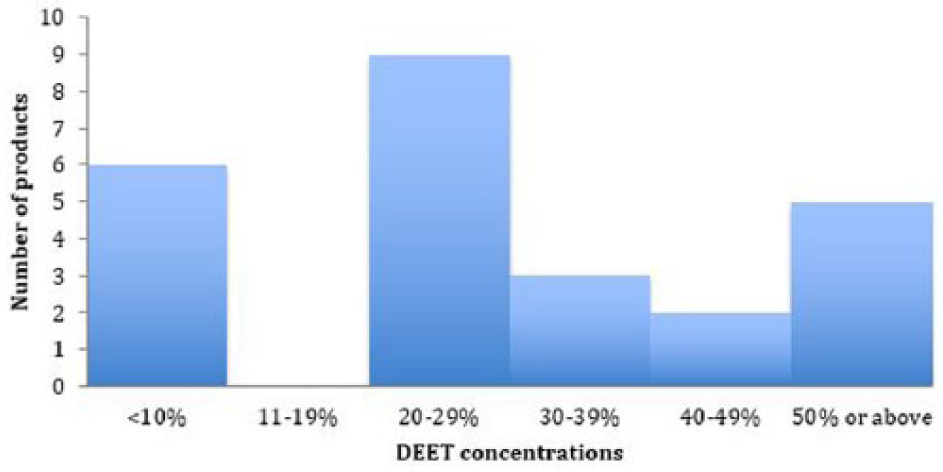
Distribution of DEET concentrations.
Discussion
Insect repellent is one of the major preventive methods from mosquito-borne diseases, mainly dengue, malaria and Zika. This is particularly important for travelers to endemic areas who engage in outdoor activities and are exposed to mosquito stings. Products containing different active ingredients in different concentrations are available in the market. Some products claim to contain natural ingredients, while some claim to be long lasting. Consumers may find it difficult to choose the most effective yet least harmful ones among all those available. One may resort to follow recommendations from either local or overseas health authorities to find the suitable insect repellents. Such recommendations from local and major overseas authorities are summarized in Table 1. DEET, picaridin, IR3535 and PMD are the four recommended active ingredients with DEET being the most frequently recommended one. These four compounds as well as botanical extracts and the recommendations issued from the major health authorities will be discussed in detail.
Local and overseas recommendations on the choice of active ingredients and their concentrations.
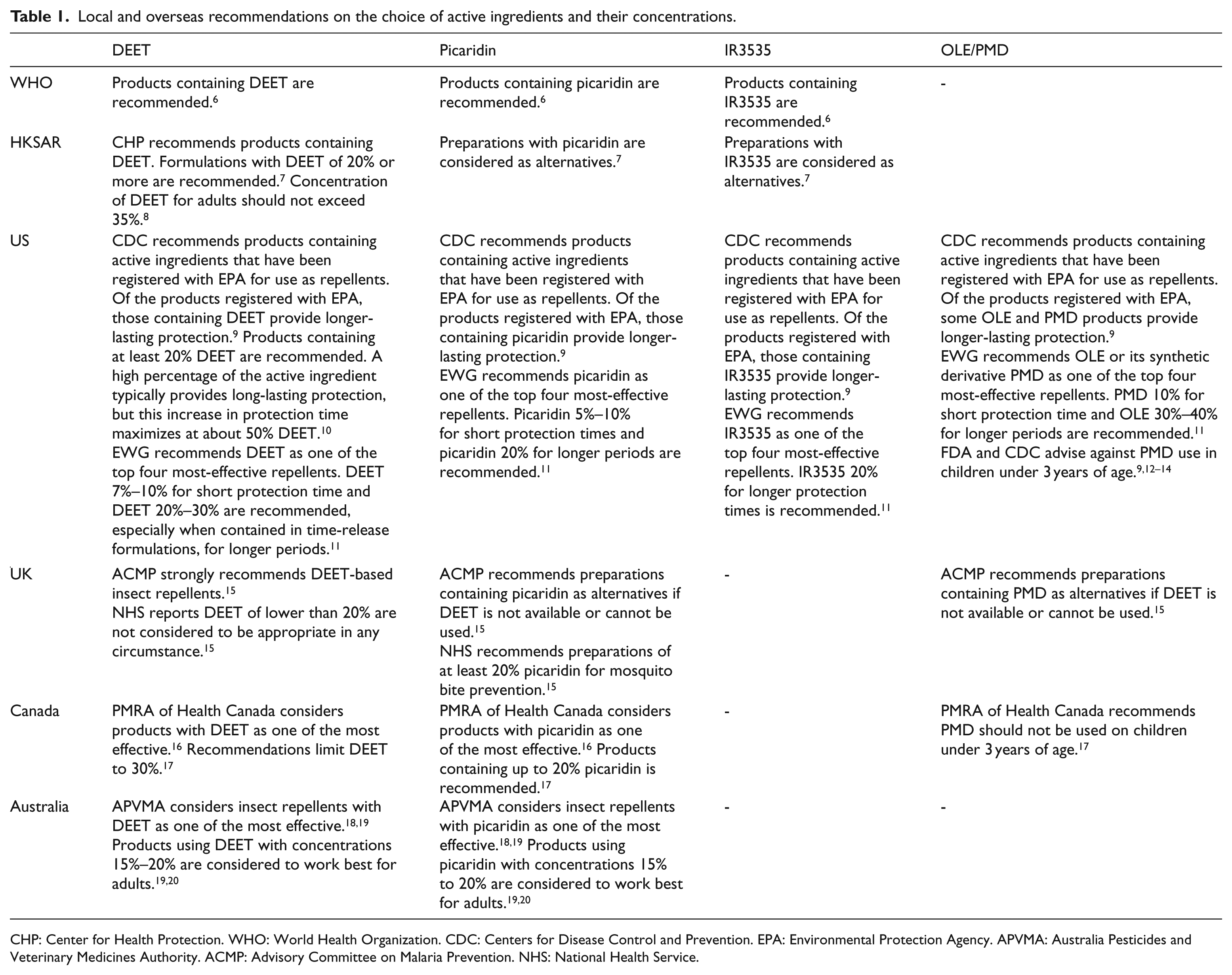
CHP: Center for Health Protection. WHO: World Health Organization. CDC: Centers for Disease Control and Prevention. EPA: Environmental Protection Agency. APVMA: Australia Pesticides and Veterinary Medicines Authority. ACMP: Advisory Committee on Malaria Prevention. NHS: National Health Service.
DEET
DEET is a broad-spectrum insect repellent, first developed by the US Department of Agriculture in 1946 for use by the US military. 21 Being the most widely tested and used compound, it is considered the gold standard insect repellent by the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) for protection against malaria, and is the standard by which other insect repellents are compared.22–24 It is also recommended by other health authorities, including CHP (HKSAR), Environmental Working Group (EWG) (USA), Advisory Committee for Malaria Prevention in Travellers (ACMP) and National Health Service (NHS) (UK), Australian Pesticides and Veterinary Medicines Authority (APVMA) (Australia) and Pest Management Regulatory Agency (PMRA) of Health Canada.7,11,15,16,18,19 Interestingly, many natural repellents products specifically write down they do not contain DEET on their packaging according to our market survey. This is in big contrast to the evidence that supports DEET as one of the most effective active ingredients available since 1940s. There is a misconception that DEET is unpleasant to use or may pose a severe health risk. It does give off a distinct odor, and can melt plastic, rubber and vinyl.7,25 It is also known to irritate the eyes and in intense doses may induce neurological damage.26,27 After reviewing reports of seizures, however, the Environmental Protection Agency (EPA) concluded the rate of adverse reactions to be rare—about one per 100 million persons. 28 The toxicology of DEET has been more closely scrutinized than any other repellent. A number of studies that investigated health risks associated with use of topical DEET-based repellents found that, when used as directed, it poses minimal health risk.17,29,30 It has been deemed safe for human use,28,31 including use on children, 29 pregnant women, 27 and lactating women. 30 It is considered to be safe by many public health authorities and organizations, including the CDC, the EPA, the American Academy of Pediatrics (AAP), and WHO (CDC 2013D, EPA 1998, AAP 2005, WHO 2012). Public education and promotion should be emphasized in this particular aspect in order to effectively prevent mosquito-borne diseases.
Generally, DEET of concentration between 20% and 35% is recommended according to the local and overseas authorities (Table 1). Such recommended range has been shown to be the minimal amount needed to provide complete protection against Aedes, Anopheles, and Culex mosquito species for 6–13 hours, with protection time proportional to concentration with a plateau effect at approximately 50%.12,32 However, our results showed that some of the products on the market are out of this range. In all, 5 (20%) of the repellents contain DEET concentration higher than 50% and 6 (24%) products contain DEET concentration lower than 20%. Products with lower concentration may affect the efficacy and duration of action as mosquito repellents while those with higher concentration may provoke seizure if applied more frequently than recommended.
Picaridin (KBR 3023)
Picaridin, a derivative of piperidine, was first marketed in Europe in the 1990s. 33 It is recommended by the WHO, CDC and EWG (USA), ACMP and NHS (UK), APVMA (Australia) as well as PMRA of Health Canada6,7,9,11,15,16,18,19 for protection against mosquito bites same as DEET, while in Hong Kong, CHP considers picaridin as an alternative to DEET. Picaridin has the advantages of being not irritating to skin and eyes, devoid of pungent odor and plastic friendly. 25 It evaporates from the skin more slowly than DEET or IR3535 and may repel insects for longer periods. Developed by Bayer AG in the 1980s and sold in the US since 2005, picaridin does not carry the same neurotoxicity concerns as DEET but has not been tested as much over the long term.6,34 It is considered safe to use for children, pregnant, and breastfeeding women.9,23 Picaridin’s comparable efficacy to DEET and favorable side-effect profile make it an appealing option and an acceptable alternative for protection against malaria and other vector-borne diseases in endemic areas. 35 Despite these advantages, only 7 out of 33 synthetic products in our survey contain picaridin. This can be explained by the fact that picaridin is less well known in the local community than DEET, probably due to the marketing strategy of these products.
There is lack of consensus on the recommended concentration of picaridin. Guidelines from the UK, Canada and Australia recommend concentration of picaridin concentration at least 20% to be effective, while EPA registration data indicates that picaridin at a concentration of 10% is effective against mosquitoes and ticks for 3.5-8 hours, and 20% is effective for 8-14 hours. 6 Picaridin 20% spray was shown to be comparable to 20% DEET for protection against Aedes, Anopheles, and Culex mosquito species, with no loss of protection over a 5-hour period. 35 Locally, the CHP does not give any specific recommendation on the concentration of picaridin.
PMD or oil of lemon eucalyptus
Oil of lemon eucalyptus (OLE) is an extract of the leaves of the lemon eucalyptus tree, Corymbia citriodora. The leaf extract is refined to increase the concentration of a naturally occurring substance, PMD. 34 Science has not yet determined the differences between PMD and OLE, but studies found that OLE provides longer protection than the equivalent concentration of synthetic PMD. 6 Our survey shows that PMD constitutes a smaller proportion (6 out of 33 synthetic repellents, 15%), similar to picaridin, in the market. PMD has been proven to be suitably efficacious and safe to compete with DEET in the field of disease prevention, and repellents have been recognized by WHO as a useful disease prevention tool to complement insecticide-based means of vector control. 36 There has been a single clinical study on the use of PMD to lower malaria incidence. 37 It was shown to provide comparable protection against malaria as DEET and is recommended by the CDC for use in malaria-endemic areas. Nevertheless, CHP of HKSAR does not recommend PMD as the repellent of choice to public.
Laboratory studies demonstrated a 30% PMD formulation provided comparable duration of protection against biting mosquitoes to low-dose (5%–10%) DEET- and picaridin-based repellents.38,39 Such concentration of PMD offers complete protection for 4-6 hours against Aedes, Anopheles, and Culex species, 12 and ticks. 32 PMD’s maximum protection time against mosquitoes and ticks is shorter than DEET’s, according to EPA documents, 6 and therefore, it requires more frequent application. 12
Several important points related to PMD should be noted. PMD products should not be confused with eucalyptus-based essential oil formulations, which are generally ineffective for long period of protection against biting mosquitoes, 40 and not approved for use as an insect repellent. 36 Because the dangers to children have not been thoroughly explored, Food and Drug Administration (FDA) and CDC advised against PMD use in children under 3 years of age.6,9,12–14
Ethyl butylacetylaminopropionate (IR3535)
After being launched in Europe for more than 20 years, IR3535 was found to be as effective as DEET against midges, and more effective against black fly and sand fly bites than DEET, with a longer duration of protection.34,41 IR3535 can be irritating to the eyes and may dissolve or damage plastics, but poses few other safety risks.8,11,34 Despite the effectiveness as an insect repellent, IR3535 is not popular in our local market and we only found two products containing it. Some studies showed 20% IR3535 offers complete protection against Aedes and Culex mosquitoes for 7-10 hours, 12 but only 3.8 hours of protection against Anopheles in some other studies. 32 NHS reported IR3535 to have a shorter duration of protection than DEET, which gives protection times against Anopheles 20%–25% higher than IR3535 at equal concentrations. 15 Therefore, IR3535 is not considered an adequate insect-repellent option in malaria-endemic regions, although it is included in the recommendations from WHO, CHP (HKSAR), CDC and EWG (USA). 12
Natural oils (botanical extracts)
More than half of the topical mosquito repellents in the market contain natural oils either alone or in combination with synthetic products mentioned above. These botanical-based insect repellents have recently gained increasing popularity among consumers, as these are commonly perceived as a “safer” choice than synthetic repellents.42,43 However, such beliefs are unfounded. EWG research indicated that unregistered botanically based bug repellents are often not the best choice. 6 These so-called natural products may contain human allergens in much higher concentration than other personal care products, leading to skin allergy/dermatitis in the presence of sunlight.15,36 Besides, their duration of action, if at all effective, may be shorter than DEET, picaridin- and PMD-based repellents, so frequent reapplication is needed. 40
Insect repellents and sunblock
The CDC recommends the use of both a sunscreen and an insect repellent when staying outdoors. In general, the recommendation is to apply sunscreen first and let it dry, followed by repellent.9,10 It was found in our survey that 5 of the 113 topical insect repellents contain combinations of synthetic repellents with sunscreen. However, the FDA recommends against using these products because the frequency of application of insect repellent is different from that of sunscreen. 25 Sunscreen should be reapplied more often than insect repellent.9,10,14 In 2004, Ross and coinvestigators demonstrated increased absorption of DEET applied under sunscreen in a mouse model, which resulted in an FDA recommendation to always apply sunscreen before DEET application. 44 The user could be overexposed to active ingredients in insect repellents if these instructions are not followed. 34
Protection against midges
In recent years, there has been increasing public concern about biting midges in Hong Kong. They are not regarded as important as mosquitos as a human disease vector, though some can transmit parasite and virus to humans. Patients may complain of intense itchiness after being bitten by such a tiny insect. Scratching aggravates the itch and may lead to secondary bacterial infection and slow-healing wounds. 45 Compared with mosquito bites, protection against biting midges is something that the public is less aware of. DEET repellents are much more popular and readily available in the market than those containing IR3535, picaridin and PMD. However, some studies showed that topical insect repellents containing IR3535, picaridin, or PMD may offer better protection than topical DEET alone when exposure to biting midges is anticipated, especially when exposed skin is covered by permethrin-impregnated clothing. 41
Back to our patient
This 30-year-old lady has just recovered from an episode of dengue infection. To prevent her from dengue hemorrhagic fever in the future, insect repellent that is effective at protecting against biting mosquitos carrying the dengue virus should be recommended. Aedes aegypti and Aedes albopictus (commonly found in Hong Kong) are the main vectors spreading dengue fever. Repellents containing 20%–25% DEET should be recommended, with protection time proportional to concentration. DEET is widely available in local shops, supermarkets and online stores, and different preparations including cream, spray and lotion can be found easily. DEET is considered to be safe and suitable for our patient who may subsequently be found to be pregnant. Picaridin and IR3535 can be the alternatives to DEET, especially when skin/eye irritation and plastics-friendliness is a concern. PMD can also be used but more frequent application is required.
Conclusion
Our local market survey found more than one third of the insect repellents contains synthetic products. The most commonly found synthetic formula is DEET. It is recommended by both local and overseas authorities as the first repellent of choice to prevent mosquito-borne diseases. Other synthetic ingredients, including picaridin, IR3535 and PMD, although recommended constitute a rather smaller portion in the market. However, natural products either alone or in combination with synthetic compounds constitute a larger proportion of samples (65%). These so-called natural products are not recommended by health care authorities. In fact, they are less effective with shorter duration of protection and some of them may even pose health risk if used for longer duration. More efforts should be made to educate the public to select clinically proven formulae to prevent emerging mosquito-borne diseases and ease the fear of rare side effects caused by DEET and other synthetic products. It is also our duty as emergency physicians to give advice on the correct choice of mosquito repellent to our patients to minimize their risk of reacquiring mosquito-borne disease, in particular, dengue hemorrhagic fever.
Footnotes
Acknowledgements
WL Lo, KL Mok and S Yu conducted the survey. WL Lo and KL Mok analyzed the data. WL Lo drafted the manuscript. KL Mok guided the outline and direction of the manuscript and finalized the version to be published. All three authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data of the survey would be available in form of Excel on enquiry.