
Abstract
Background:
Diagnostic ultrasound is increasingly used by nonradiologists in trauma victims and critically ill patients. In the emergency department, the extended focused assessment with sonography for trauma and Polytrauma Rapid Echo-evaluation Program protocol are often used to assess these patients. Dutch Polytrauma Rapid Echo-evaluation Program-trained Emergency physicians are implementing the use of ultrasound in the emergency department but might encounter barriers to overcome.
Objectives:
This study aims to explore individual experiences of Dutch emergency physicians.
Methods:
We performed a qualitative study by conducting semi-structured interviews in Dutch emergency physicians working in a Level 2 emergency department that completed the 2-day Polytrauma Rapid Echo-evaluation Program course at least 1 year before the interviews. Data were analyzed using directed content analysis.
Results:
Eight emergency physicians employed by eight different hospitals were interviewed. Thirteen categories were identified in the transcribed interviews and these were combined into four general themes: (1) the desire to develop the Emergency Medicine specialty, both nationally and local; (2) incentives to start using ultrasound; (3) exploring practical applications of ultrasound; and (4) barriers faced while implementing emergency physician-performed ultrasound on the emergency department. The interviewees regard the course to be a solid base and are eager to independently perform ultrasound examinations, although challenges are faced.
Conclusion:
This exploratory study provides essential insight in Dutch emergency physicians implementing ultrasound in their emergency department. It shows that there is a need to develop a quality assurance system and it identified barriers that have to be dealt with.
Introduction
In trauma patients, diagnostic ultrasound (US) used by nonradiologists is becoming commonplace. It is used successfully in trauma victims and critically ill patients in the emergency department (ED), operating theater, and in out-of-hospital settings. Also, it is used in remote locations such as the battlefield and outer space.1,2
US is used in the ED to answer simple yes/no questions that could make the difference detecting or ruling out life-threatening conditions such as pneumothorax, pericardial effusion, and intra-abdominal bleeding.3–5 Therefore, life-saving interventions such as a tube thoracostomy may be performed more expeditiously, or prevented if deemed unnecessary. 6 Also, US may lead to a reduced usage of other imaging techniques such as chest X-rays and computed tomography (CT) scans.7–10
Various emergency US examination protocols are used. The extended focused assessment with sonography for trauma (eFAST) protocol assesses for free abdominal and pericardial fluid, and pneumothorax. In the Netherlands, the similar Polytrauma Rapid Echo-evaluation Program (PREP) protocol is widely used in EDs and in the prehospital setting. 11 Originally from Nîmes, France, it is taught and used in many European countries and Canada. It offers a uniform and fast five-step method to assess an injured or critically ill patient. 12
During a 2-day PREP course, the candidates are taught ultrasound theory and they will perform at least 20 supervised US examinations on fellow candidates, simulated patients in an ED or prehospital scenario, and peritoneal dialysis patients. The latter group of subjects carry a significant amount of fluid in the peritoneal cavity, resulting in a positive US scan mimicking intraperitoneal bleeding. Nonradiologists can be effectively trained in a brief training to perform eFAST or PREP examinations. 13 Nonetheless, this skill needs to be maintained and improved by routinely using it in everyday practice. Its learning curve is estimated to level off at 30–100 US examinations. 14
Although PREP-trained emergency physicians (EPs) are well prepared, they are facing barriers. Emergency medicine is a young specialty in Dutch healthcare; in 1999, the Dutch Association of Emergency Physicians (Nederlandse vereniging van spoedeisende hulp artsen, NVSHA) was formed and 1 year later the first 3-year training programs started. 15 Implementation of US on the ED is frequently hampered by so called turf battles—about who should perform US on the ED—between radiologists and other medical specialists on one hand, and EPs on the other hand.16,17 Other complicating factors might be unavailable or unfamiliarity with US equipment, easily accessible conventional radiology and CT scanning, and EPs still lacking confidence in their recently acquired knowledge and skills.
Until now, there are no reports on how Dutch EPs implement their US knowledge and skills on the ED and what challenges they encounter. Therefore, the main objective of this study is to explore individual experiences of Dutch PREP-trained EPs who started routinely using US in their EDs.
Methods
Design
A qualitative study by means of semi-structured individual interviews was conducted in January and February 2014, to explore the subjects’ perceptions and experiences. Ethical approval was obtained from the institutional ethics review board of the Radboud university medical center, Nijmegen. Written informed consent was obtained from all participants.
Since this is a largely unexplored topic, the interviews were guided by an initial topic list aiming to identify the subjects’ motivation (intention) and ability (behavioral control) to perform US examinations on the ED. Topics were based on three sources. First, topics were formulated to identify three factors (attitude toward the behavior, the subjective (social) norm, and perceived behavioral control) that influence the intention to perform a given behavior (performing US on the ED) as conceived in the theory of planned behavior by Fishbein and Ajzen 18 and Ajzen. 19 This also includes any incentives and barriers influencing the behavior. Second, topics were based on earlier discussions the researchers had with other course candidates. Finally, one topic was based on previously mentioned “turf battles.” 16 The topic list is displayed in Appendix 1. Relevant new topics brought up by the interviewees were added to the list.
Recruitment and setting
We contacted randomly selected EPs who successfully completed the PREP course between 1 and 4 years preceding the study (2009–2012). After they agreed to participate, they were further screened for possible inclusion.
Inclusion criteria were EPs employed at a Level 2 hospital for a minimum of 20 h per week since completion of the course. In a Level 2 (ranging from 1 to 3, Level 1 being the highest) hospital, seriously injured and critically ill patients can be treated, although not all facilities, such as neurosurgery, are present. In these hospitals, EPs will have enough exposure to critically ill patients and opportunities to perform US examinations. Level 1 hospitals are generally well-equipped university hospitals where US examinations are typically performed by radiology residents. The interval between the course and interview was chosen to allow the EPs ample time to implement the use of US in their ED and to potentially experience any burden and challenges. We excluded EPs who already performed PREP or eFAST US examinations, at least once a month, preceding the course.
Included subjects received written information in more detail in advance and written informed consent was given prior to the interview. Further inclusion of subjects was continued until no more new codes were determined during the interview process and data saturation was reached.
Procedure
Subjects were interviewed at their own workplace by a trained interviewer (E.V.H.). The interviews were conducted face-to-face in a secluded room without disturbances. Open-ended questions based on the initial topic list were used to initiate the conversations. The interviews were conducted in Dutch and audio-recorded. The mean duration of the interviews was 26 min. Notes on non-verbal communication were taken. Member checks were performed: every participant was invited to read and comment on a summary of the transcription.
Data analysis
Every interview was transcribed verbatim and analyzed directly afterward. The transcriptions were subjected to thematic content analysis, inspired by the work of Braun and Clarke. 20 Thematic analysis was performed using a constant comparative (iterative) method using the OpenCode application (OpenCode 4.0.2. University of Umeå, Sweden). After every transcribed interview, relevant data extracts were selected and coded. New codes were added to the code tree and used in coding of the next transcript. After coding all transcripts, codes were combined into categories using axial coding to match those in the initial topic list, if appropriate. Newly identified categories were added to the list. The data were selectively coded to bring previously defined categories together into themes to see the bigger picture.
Transcripts were anonymized before coding. After completion of the study, data that could trace to an individual subject, including audio recordings, were discarded.
Results
Participants’ characteristics
A total of eight EPs (three males, five females) were interviewed, employed by eight different Level 2 hospitals.
Data analysis and themes
Coding resulted in 225 open codes. These were combined into 13 categories. Next, we identified four themes as displayed in Table 1. Some codes were associated with multiple categories and themes.
Categories and themes related to the initial topic list and newly identified categories.
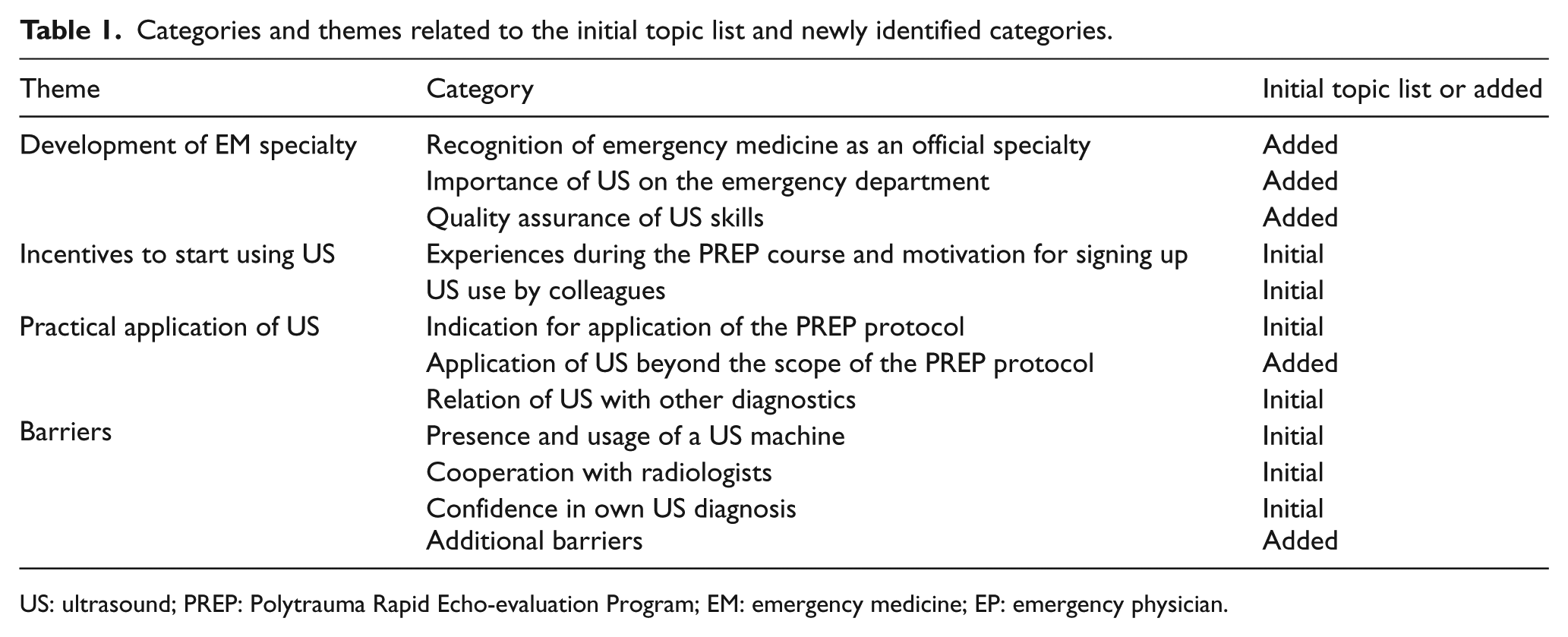
US: ultrasound; PREP: Polytrauma Rapid Echo-evaluation Program; EM: emergency medicine; EP: emergency physician.
Themes
Development of the emergency medicine specialty
Importance of US on the ED and the recognition of EPs as a medical specialty
EPs are relative newcomers in Dutch healthcare. Ever since their introduction, skills, and responsibilities have begun shifting.
Participants have stressed the importance to improve the recognition of their medical specialty and wanted to show their added value to the hospital. According to some, implementing US clearly contributes to these goals. They experienced criticism from other specialties: However, in The Netherlands there are some scientific associations, such as anesthesiology and internal medicine, that still express some criticism regarding the presence of EPs. And yes, I believe this has to do with a feeling of land grabbing (p.2). And then it is difficult to bring into the limelight that we also largely fill in a new area. And are taking over a non-existent area (p.3).
In addition to recognition of the specialty, implementation of US on the ED would yield independence, time saving, and logistical advantages: And I think it is super convenient no longer having to depend on radiologists that I have to call into the hospital or to have patient undergo US examinations in places that are not safe for them to be at (p.3). So yes, for that matter, I can see the added value. It is an imaging technique that is fast to perform. Basically, it takes a few minutes to complete an US examination (p.2). When I do an US examination and detect free fluid, I’m not afraid to be energetic and rush the patient to the CT scanner. That is added value, the logistics process (p.3).
Quality assurance of skills
In over half of the hospitals, EPs were looking for a suitable quality assurance system. In one hospital, together with radiologists, they developed an in-hospital training program. In another, they planned to commence radiologist-supervised US examinations.
Quality assurance of US skills was frequently mentioned. On one hand, individual responsibility was highlighted: Yes, I believe that during time one has to develop their skills. You then have to decide for yourself whether to make official statements about your examinations or not (p.7).
On the other hand, there appeared to be a clear need for a certification system in which knowledge and skills would be documented. On one ED, the EPs themselves determined that they were not qualified to perform diagnostic US scans: Well, the biggest objection the other consultants had to implementing US on the ED was they couldn’t tell how our knowledge and skills were going to be assured. We discussed this and realized we couldn’t tell either. So, they are right! We feel it is important and we want to practice so we can take US usage by EPs to another level. But now we are not ready for it, yet (p.6).
Others reported initial suspicion as well but took a different approach: I can really empathize with the surgeon who witnesses an EP do an US examination he has never seen do one before and then wonders: are you sure you can do this? I feel that is a logical reaction. And it is up to us to prove this can be implemented for years to come. It will take time, but that’s the case for a lot of novelties (p.2).
Five out of eight participants were developing a system to document every EP’s US skills. Frequently mentioned was the performance of radiologist-supervised examinations: We have agreed with the radiologists we will actually, for a certain period of time, will do it really together. So, they will stand next to us and supervise. And from the moment they will say they are confident enough, they will supervise us from a distance (p.8). But ideally our knowledge and skills will be tested by a very wise person, the radiologist, and says: “Indeed, you can do that well enough” (p.3).
Incentives to start using US
Motivation to sign up and experiences during the PREP course
Course participants regarded the PREP course to be very instructive and primarily a basic course to start learning US: You are scanning the same set of regions and the US approach to those regions is always the same. I think that is very good of PREP. It doesn’t teach everything I could possibly make an image of. It only teaches to produce a standard image on the screen. It is all for dummies (p.3).
Peritoneal dialysis patients are recruited to serve as models during the course. Two participants explicitly appointed this to be of added value to the course. Another basic US course covering a range of topics including eFAST is organized by the Dutch Association of Emergency Physicians (NVSHA). Two participants indicated to prefer this over the PREP course: At this moment, I would pick the NVSHA course, rather than the PREP. But it wasn’t available at the time (p.6).
US use by colleagues
A motivation to start using US in general was that some colleagues were using US already. We asked the EPs why they signed up for the PREP course.
Why? Because one of my colleagues who participated earlier told me about it. She was very excited about the course! (p.2)
Conversely, another was struggling stimulating colleagues to use US: I have to put in a lot of effort to get my colleagues on board. Some colleagues get cold feet. I suppose they find it difficult to draw conclusions from their ultrasound images. That is the hardest part of it, I suppose, because just putting a transducer on somebody is easy! (p.5)
Multiple participants said every EP should be proficient in emergency US: I wanted to sign up for the course because I feel that being an EP means you must be able to do an emergency US examination. And that’s very important (p.7). I brought up the subject again at our latest meeting. I believe the other consultants should be able to count on us to all have equal high standards and skills (p.5).
Practical application for US
Indication for application of the PREP protocol
Some participants felt that US is not always indicated in a patient that sustained high-energy trauma, and that it is more important to let the clinical picture prevail: ATLS dictates: assess the patient and based on the clinical picture a US examination is done (p.2).
Conversely, participants told that US examinations are performed on patients with minor injury without much pain. It is then regarded as an opportunity to practice US skills, without an obvious indication. In fact, this opportunity was regarded as a separate indication. Other reported indications were abdominal pain, cardiovascular instability, distracting injury, intoxication, and undifferentiated shock.
One participant only performed US examinations in patients with a low probability of serious injury. In every other case, the radiologist was consulted: The bottom line is that on the patients with low suspicion (…) from whom you expect no real injury (…) those cases we use the US on (p.1).
Application of US beyond the scope of the PREP protocol
Several participants describe the PREP course as a stepping stone to start with US in the ED. They were excited about the different US applications they discovered after having completed the course. Deep venous thrombosis (DVT), hypotension, intravenous access, regional anesthesia, hydronephrosis, kidney and gallstones, foreign bodies, Achilles tendon rupture, fracture position (after repositioning), and Inferior vena cava (IVC) measurements for volume status were mentioned: We are continuously expanding, also in respect to US. We will be using US for DVT as well. Um, so yes, we are expanding, but specifically within the scope of emergency US (p.7).
Relation of US with other diagnostics
All participants agreed that US examination has taken a prominent place in diagnostic imaging techniques and was considered by some participants for certain indications to be more reliable than chest X-ray: For instance, in a trauma victim with suspected pneumothorax, we will put more confidence in our own US than in one supine chest X-ray without pathology (p.4).
US might replace some other imaging techniques, too: In the case of a hemodynamically instable patient, we actually let it guide treatment decisions. If the patient is suspected of intra-abdominal injury and there is also free fluid detected by US … Well, we put two and two together and rush the patient to surgery (p.8).
Whenever US was followed by another imaging technique, this was considered to be an important verification: Whenever, for instance, a CT scan is performed, to us there is the added value to verify the results of our US examination. That is very important to us (p.7).
Conversely, gaining experience by performing an US examination after a diagnosis is made with other diagnostics was also mentioned: … the other day there was a pneumothorax. I thought: ah, let’s have a look with ultrasound. You know, let’s see if I can see it, too (p.1).
Barriers
Presence and usage of a US machine
In four out of eight hospitals, the ED owned an US machine. Three departments have entered into a loan agreement with either the radiology or urology department. One ED had no disposal of a US machine at all: We are working on it. Together with the radiologists (p.8).
On another ED where no US machine was available when requested, the (resident) radiologist would visit and bring the US machine. They then allowed the EP to perform the actual US examination.
Cooperation with radiologists
We noted significant differences in the way the EPs cooperated with the radiology department. In one hospital, EPs were not allowed to perform US examinations by themselves: That is what we agreed on with the radiologists. Whenever an US examination is warranted, we do one first and the radiologist repeats it afterwards (p.6).
In multiple hospitals, the radiologists preferred the EPs to perform the US examinations themselves: At our hospital radiologists are very satisfied with us doing the US scans on trauma victims. During night and weekend shifts for instance, they then don’t have to rush into the hospital (p.7). We have a very good relationship with the radiology department. They really do understand, but some are genuinely concerned about possible degradation of the quality of US exams. And I believe that is a legitimate concern (p.3). Besides that, there is an issue that radiology residents have to make sure they perform enough US exams of their own so they develop their skills, too (p.6).
In some other hospitals, the sentiment regarding EPs using US was quite different: Some radiologists aren’t very happy with us doing US exams. And neither are some of the other consultants. Some consultants are very comfortable with us performing the exams, and others just aren’t (p.6).
This phenomenon has been called land grabbing and gives rise to political debate: … it is just land grabbing. Is has got nothing to do with them thinking we can’t do US examinations. They will claim that’s the reason. But hey, US scanning is just like an intubation. Anyone can be taught how to do it (p.2). I do remember that when we got our first US machine and especially afterwards, at the political level there has been quite some quibbling about it. The radiologists still feel US belongs to them. Obviously, it is no longer true that certain diagnostic techniques are a prerogative of a particular discipline (p.2).
Confidence in own US diagnosis
There was a wide variety in the degree of confidence that each participant had in their US diagnosis: I lack the confidence, so I always ask somebody else to do another US examination. In 95% of cases I’m confident about my diagnosis (p.4). I do the exam myself, I interpret it myself, and if necessary I take action (p.5).
The importance of practice was emphasized and it was mentioned that after 50 examinations, confidence would grow: You just have to do it often and must expose yourself to repeated US examinations and that just requires an investment of time and energy. A lot of time has to be invested (p.1).
Differences in perceived difficulty between assessment of the chest and abdomen appear to be personal: Well, it can be hard sometimes to detect a pneumothorax. Free intraperitoneal fluid, on the other hand, isn’t hard to detect at all (p.2).
Additional barriers
In addition to the lack of a US machine preventing the use of US, other limitations were a lack of time and a shared responsibility between physicians for a patient: Whenever there is an indication to do an US examination and, um, I am there, I’ll do it myself primarily. If there is a lack of time or somebody else is caring for the patient, then I’ll call the radiologists.
Discussion
In this study, we mapped the factors influencing the experience, confidence, and practical application of emergency US. Every EP valued the use of US and it was described to be an indispensable tool in daily practice. They were highly motivated to use their new skills. This is in concordance with the results of Heinzow et al. 21 who interviewed a group of medical students before and immediately after a basic US course and also found them to be highly motivated to apply the newly acquired US skills in daily practice.
In the Netherlands, no guidelines exist on the implementation of EP-performed emergency US on the ED. Every ED has the responsibility to assign specific (US) qualifications to the individual physicians. EDs in the United States, however, adhere to the Ultrasound Guidelines, developed by the American College of Emergency Physicians (ACEP). 22 These guidelines are helpful starting an emergency US program and provide recommendations for proper implementation of emergency US on the ED, including a minimum number of clinical training hours.
The cooperation with the radiology department appeared to be very agreeable in some hospitals, while in others, tensions were reported. Participants indicated that radiologists themselves, rightly or wrongly, were concerned about the quality of EP-performed US examinations. Therefore, we would recommend the development of national guidelines comparable to the ACEP.
This study shows that there is a need for a quality assurance system for US skills. The purpose of such a system may be to keep a record of every EPs knowledge and skills. It might consist of course certificates and a collection of stored US images or video clips demonstrably supervised by radiologists or expert colleagues. In one hospital, a lack of quality assurance resulted in mandatory verification of every US examination by a radiologist. In another, EPs are simply relying on the skills of their colleagues. Meanwhile, a Dutch US certification program for EPs has been adopted by the general assembly of the NVSHA in June 2017.
US training has recently become a compulsory item in the residents’ curriculum. It is essential to remain confident with the PREP protocol and US images. Therefore, it is advised to schedule regular practice to improve on speed, accuracy, and recognition of negative US images in healthy subjects. Regular practice should be part of the quality assurance system.
Budhram et al. reported an effective emergency US training program for EPs, including eFAST. The participant’s goal was to complete and record 25 technically adequate eFAST studies on their EDs. To record the knowledge and skills on every participant’s ED, and for quality assurance, an on-site archiving system was put in place. 23 They also observed the turf battles: the radiology department questioned the EP’s competency and a they feared a reduction in their department’s study volumes.
Strength and limitations
This study yields new information about the experiences of Dutch EPs running a US protocol in practice. We gained insight in the role of Dutch EPs on their EDs, their collaboration with colleagues, the varying levels of confidence, and the need for a quality assurance system. Because we used open-ended questions, new topics emerged that complemented the initial topic list.
A limitation of the study is that one researcher coded the transcripts. This might impact the reliability of coding. Furthermore, this study is limited in its scope by including a homogenous group of EPs employed by Level 2 hospitals only. Also including EPs from Level 1 and 3 hospitals might have produced a more complete overview.
To successfully implement US, EPs should focus on the development of a quality assurance system. However, it remains unclear whether a uniform (national) system is preferred or departments prefer to develop their own system.
Furthermore, emergency US should be defined more clearly to benefit accreditation and uniformity. The ACEP 22 Ultrasound Guidelines include a list of basic US applications considered part of emergency US.
Conclusion
This exploratory study provides essential insight in Dutch EPs implementing US on their ED which could be further studied in a national survey with all EPs. Furthermore, the study shows that there is a need to develop a quality assurance system and barriers to overcome were identified. Every EP recognized the importance of EP-performed emergency US and regarded it an indispensable tool in daily practice and of value for the recognition of their specialty. The EPs all valued the PREP protocol to be a solid foundation when starting to learn and implement emergency US. Also, every EP stressed the importance of practice.
Footnotes
Appendix
Motivated initial topic list.
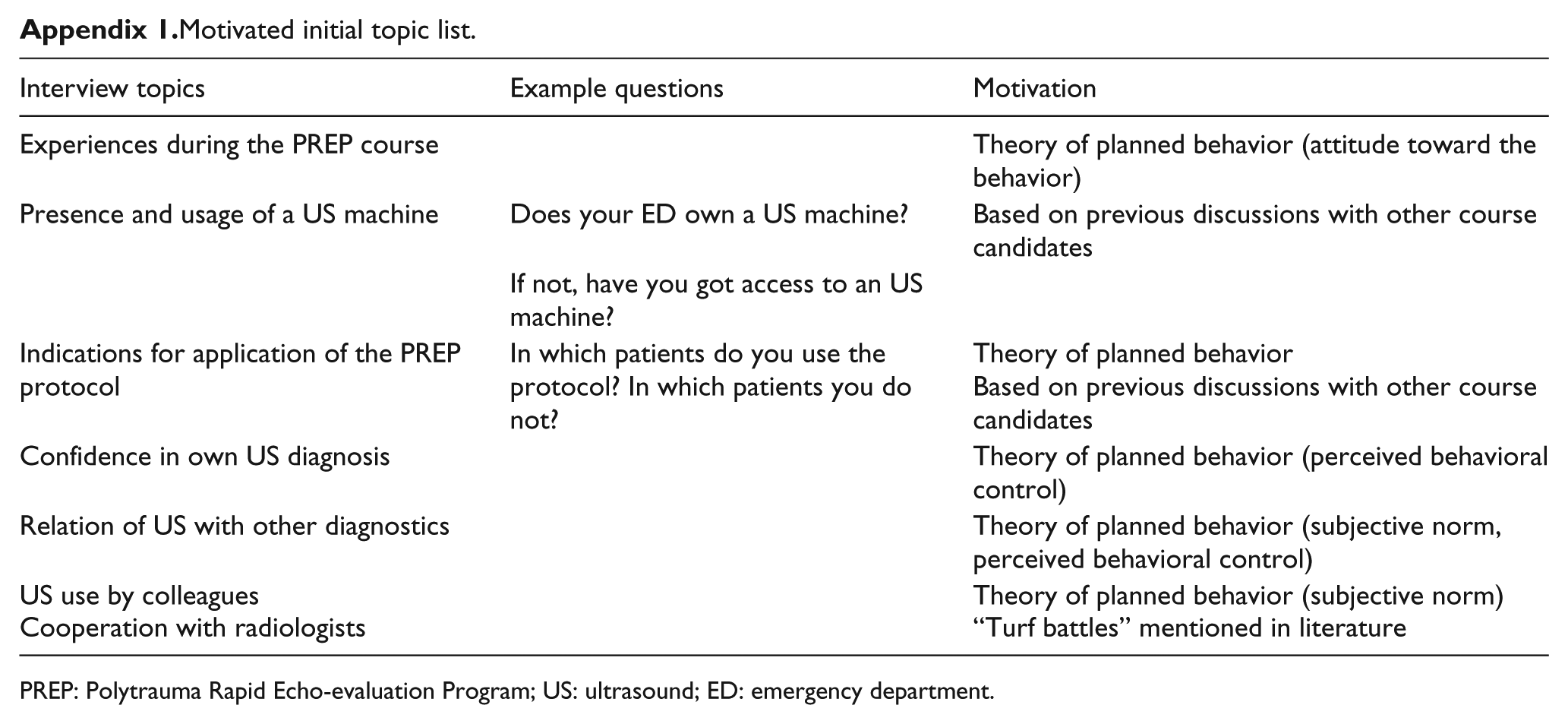
| Interview topics | Example questions | Motivation |
|---|---|---|
| Experiences during the PREP course | Theory of planned behavior (attitude toward the behavior) | |
| Presence and usage of a US machine | Does your ED own a US machine? | Based on previous discussions with other course candidates |
| If not, have you got access to an US machine? | ||
| Indications for application of the PREP protocol | In which patients do you use the protocol? In which patients you do not? | Theory of planned behavior |
| Confidence in own US diagnosis | Theory of planned behavior (perceived behavioral control) | |
| Relation of US with other diagnostics | Theory of planned behavior (subjective norm, perceived behavioral control) | |
| US use by colleagues | Theory of planned behavior (subjective norm) | |
| Cooperation with radiologists | “Turf battles” mentioned in literature |
PREP: Polytrauma Rapid Echo-evaluation Program; US: ultrasound; ED: emergency department.
Acknowledgements
All authors contributed substantially to the manuscript and all agree with this definitive version. E.V.H. was responsible for conducting, transcription, and coding of the interviews. R.K., L.P.B., and E.V.H. collaborated on the design and conduct of the study, and the interpretation of the data. Early versions of the manuscript were written by E.V.H. and R.K. M.W. was responsible for writing and revising the manuscript and providing valuable insight in the emergency physicians point of view. G.J.S. and N.H. contributed significantly through expert advice and on completing of the manuscript. Y.E. provided valuable input on qualitative research methodology, interpretation of the data, and completion of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and material
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study. The transcripts of the interviews are archived at the Fontys University of Applied Sciences, Eindhoven, the Netherlands. Numerous quotes from the transcripts are included in the manuscript.
Informed consent
Written informed consent was obtained from all participants for their anonymized information to be published in this article.
Ethical approval
The Fontys University of Applied Sciences approved the study. Ethical approval was obtained from the institutional ethics review board of the Radboud university medical center, Nijmegen, and decided it to be exempt from further formal ethical review (2017-3147).