
Abstract
Background:
Evaluating the effectiveness of pediatric emergency medicine training is essential to ensure that emergency physicians and emergency medicine residents have sufficient knowledge, skill, and confidence in optimizing care for acute pediatric visits. Although the field of pediatric emergency medicine has experienced phenomenal growth in past decades, it still faces challenges in how to best implement the curriculums in emergency medicine residency training programs.
Objectives:
Exploring emergency physicians’ and emergency residents’ perspectives on pediatric emergency medicine training in emergency residency training programs in Taiwan through a nationwide survey.
Methods:
The survey was distributed to 1281 emergency physicians and emergency medicine residents in 43 teaching hospitals. The survey inquired about demographic data, hospital type, rank of proctored trainers and assessors, and the setting of pediatric emergency medicine training. Participants’ confidence in managing acute pediatric visits and their satisfaction and reflections of their pediatric emergency medicine training were explored.
Results:
In all, 258 responses were received from 117 residents and 141 emergency physicians. Seventy-seven percent reported working in medical centers. Clinical supervision was primarily performed by pediatric attending physicians and emergency physicians. Fifty-eight percent of participants felt satisfied with their pediatric emergency medicine training. However, only 52.3% felt confident managing acute pediatric visits, which was attributed to inadequate exposure to pediatric patients. Residents noted lack of confidence in managing newborns, infants, and clinical procedures. Therefore, simulation training and point-of-care ultrasound learning were considered advantageous.
Conclusion:
The pediatric emergency medicine training in emergency medicine residency programs is diverse in intensive care training, supervisors, and assessors. Surveys demonstrate that learning experience in pediatric wards and emergency department rotations is associated with overall satisfaction with pediatric emergency medicine training; inadequate exposure to pediatric patients contributed to learners having less confidence. Emergency medicine residency program reform might focus on adequate hands-on pediatric patient care.
Keywords
Introduction
Pediatric patients account for 20%–30% of all emergency department (ED) patients.1–3 The importance of the pediatric patient population also lies in their unique anatomic structure, pathophysiological mechanism, pharmacological reactions and dosages, and social and ethical considerations that are distinctly different from those of the general adult population. Pediatric emergency medicine (PEM) is a subspecialty that has been developed based on the unique health-care needs for children’s emergency visits. It is well established in some countries and evolving in some others.4–6 Emergency medicine (EM) doctors treat many pediatric patients in emergency settings. 7 How to optimize the quality of care for children presenting in the general ED consistently raises concerns.8–11 As a result, PEM training has been integrated into the EM residency curriculum in many countries.
Despite PEM training’s acknowledged importance, the number of pediatric patients and the diagnostic case volume seen by EM residents during their residency training vary widely. 11 Variations of confidence about clinical skills, medical treatment, and satisfaction with their residency training program, 12 which contributes to the quality of pediatric emergency patient care, also raise concerns.9,10,13,14 Medical malpractice claims could also arise from errors in diagnoses of pediatric emergency care in the ED setting if the first-line practitioner is not familiar with common medical diagnoses.15,16 The issues of lack of formal curricula or faculty expertise for patient safety and unexpected medical errors for pediatric EM trainees have also been raised. 14 Even though dual training programs that include both EM and pediatrics have been promoted,17,18 there has been a decline in the number of EM-trained physicians in PEM fellowships since 2000 in the United States. The barrier of fellowship training of PEM among emergency residency graduates also attracts attention.5,19 To achieve high-quality emergency care for pediatric patients, PEM education or clinical training is considered key.20–23
How to best implement a PEM residency training program is still controversial,24–26 and most countries lack a formal curriculum. 14 In the United States, the Society of American Emergency Physicians established a Pediatric Education Training Task Force in 1995, seeking to manage the educational experiences of EM residents in the field of pediatric EM. 27 Most training programs included a PEM core curriculum of core lectures, journal clubs, PEM grand rounds, and PEM morbidity and mortality conferences.3,4,25 In some programs, rotations and electives most often included the inpatient pediatric ward, the pediatric intensive care unit (PICU), and the pediatric ED (PED).1,25 In some more advanced PEM training programs, links between PEM scholarship and providing the best practices of PEM practice have already been built into the curriculum. 20 Furthermore, specific areas of care for pediatric emergency patients, for instance, pediatric psychiatric emergencies and pediatric emergency medical services (EMS) courses, are also being planned.28,29
Although the field of PEM has experienced phenomenal growth in the past decades, it still faces challenges in how to best implement a good PEM curriculum.1,3,30,31 Moreover, very few national surveys have investigated perceptions of PEM training among emergency physicians, whether in Asia or worldwide. This study explores the perception of and influential factors for the satisfaction with PEM training and confidence of PEM practice among current emergency physicians in Taiwan using a national survey to generate suggestions for improvements to the current curriculum.
Methodology
Study design and setting
This cross-sectional online questionnaire survey was distributed by the secretary of the Taiwan Society of Emergency Medicine (TSEM). In Taiwan, a pediatric committee under TSEM was established to organize and supervise PEM training programs for EM residents in 2004. Currently, PEM training courses consist of a 2-month pediatric ward rotation and a 2-month emergency pediatric training. This study was approved by the local ethics boards (IRB No. 201800667B0D001) and was qualified for a waiver of informed consent.
Participants
According to TSEM, there are 43 Resident Review Committee (RRC)-approved EM training hospitals. In all, 1281 physicians were invited (905 attending physicians and 405 residents), and 258 responses were received. The overall response rate was 20.14%. The participants include those who had received or currently were receiving PEM training in EM residency training programs. We exclude the physicians who left RRC-approved EM training hospitals.
Questionnaire development and dissemination
The questionnaire was developed by senior emergency physicians in the Committee on Pediatric Emergency Medicine of the TSEM via consensus methods. The content included (1) the pediatric ward/intensive care unit/pediatric emergency rotation time and satisfaction, (2) department that is in charge of PED rotation, (3) supervision for PED rotation training, (4) responsibility for learning assessment, (5) pediatric emergency case loading, (6) clinical pediatric management confidence, and (7) open questions about this training program (including training pattern and advice for training program).
Data analysis
The continuous data are presented using mean and standard deviation (SD), and categorical data are presented using counts and percentages. Differences between two groups are compared using independent t-test or Wilcoxon rank-sum test for continuous variables and Chi-square test or Fisher exact test for categorical variables. The relationship between overall and site-specific pediatric training satisfaction is assessed using Pearson’s correlation coefficient. The statistical analysis was performed using SAS software version 9.3 (SAS Institute Inc., Cary, NC, USA). A p value of less than 0.05 was considered statistically significant. Content analysis is used to determine the presence of certain words, themes, or concepts within given text in the surveys.
Results
Among the 258 participants (Table 1), there were 117 (45.4%) residents and 141 (54.6%) attending physicians. About three-fourths reported working in medical centers. Pediatricians took charge of most pediatric emergency training (69.4%) and assessments (65.1%) for EM residents. Emergency physicians still contributed to training (25.2%) and assessment (29.5%), and one-quarter of pediatric emergency training programs were conducted collaboratively by both pediatric and EDs (Table 1). Table 2 presents the length of training in pediatric wards, PICUs, and PEDs and site-specific satisfaction. The most common EM training course comprised a 2-month or longer pediatric ward rotation plus a 2-month or longer PED training, but it lacked a PICU rotation. The proportions of participants who felt satisfied with their PEM training and who possessed sufficient confidence in pediatric patient management were 58.5% and 52.3%, respectively (Table 2).
Descriptive results of the participants.
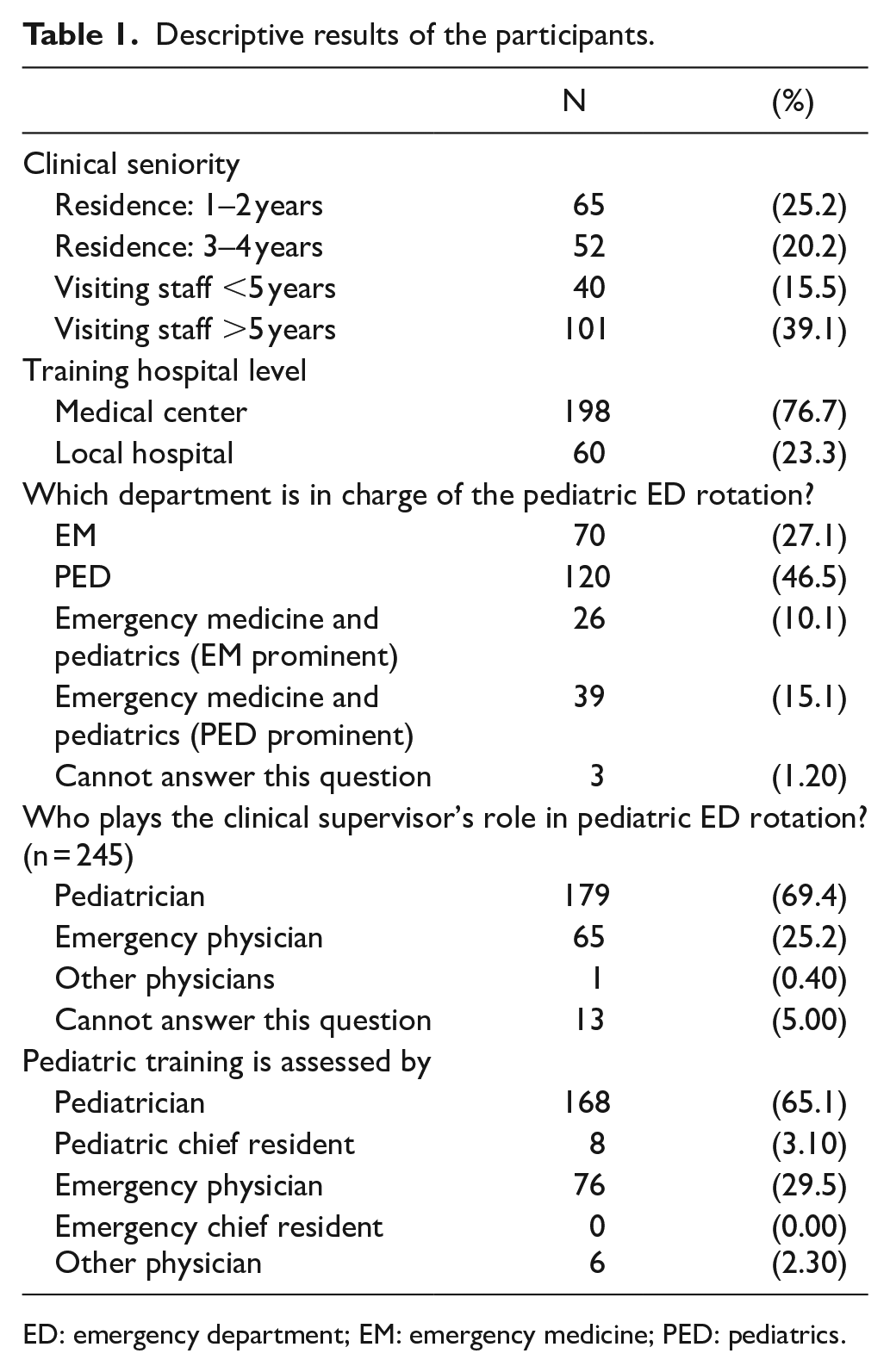
ED: emergency department; EM: emergency medicine; PED: pediatrics.
Satisfaction with the pediatric emergency medicine training in EM residency training program.
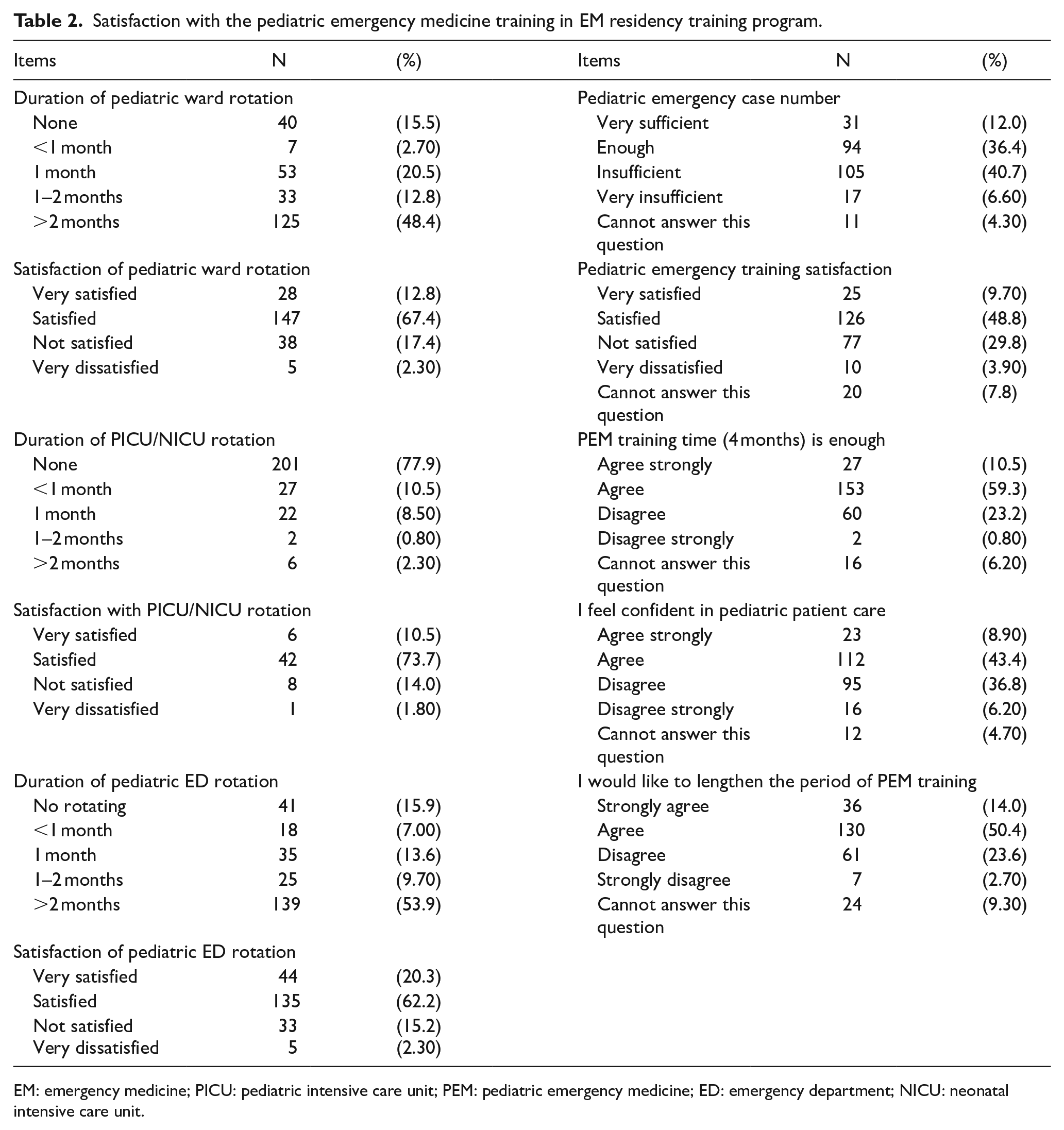
EM: emergency medicine; PICU: pediatric intensive care unit; PEM: pediatric emergency medicine; ED: emergency department; NICU: neonatal intensive care unit.
In the analysis of influential factors associated with pediatric training satisfaction or overall confidence in pediatric practice, a stratified comparison is shown in Table 3. Participants who worked in medical centers (2.72 ± 0.69 vs 2.63 ± 0.79, p < 0.05), who felt they had sufficient duration of training (2.81 ± 0.69 vs 2.44 ± 0.68, p < 0.001), who received more than 1 month of pediatric ward training (2.83 ± 0.63 vs 2.48 ± 0.78, p < 0.001), who received more than 1 month of PED rotation training (2.80 ± 0.66 vs 2.48 ± 0.76, p < 0.01), and who believed they had sufficient case exposure (3.04 ± 0.59 vs 2.36 ± 0.66, p < 0.0001) reported significantly higher training satisfaction ratings. However, participants who felt they had sufficient duration of PEM training (2.69 ± 0.68 vs 2.37 ± 0.83, p < 0.01), who received more than 1 month of PICU training (2.56 ± 0.75 vs 3.14 ± 0.69, p < 0.05), who received more than 1 month of PED training (2.34 ± 0.76 vs 2.71 ± 0.72, p < 0.001), who had emergency physicians in charge of their PED training (2.74 ± 0.77 vs 2.48 ± 0.72, p < 0.05), and who believed they had sufficient case exposure (2.75 ± 0.72 vs 2.45 ± 0.76, p < 0.001) reported significantly stronger clinical confidence ratings (Table 3).
Comparison of pediatric emergency medicine training satisfaction and clinical confidence.
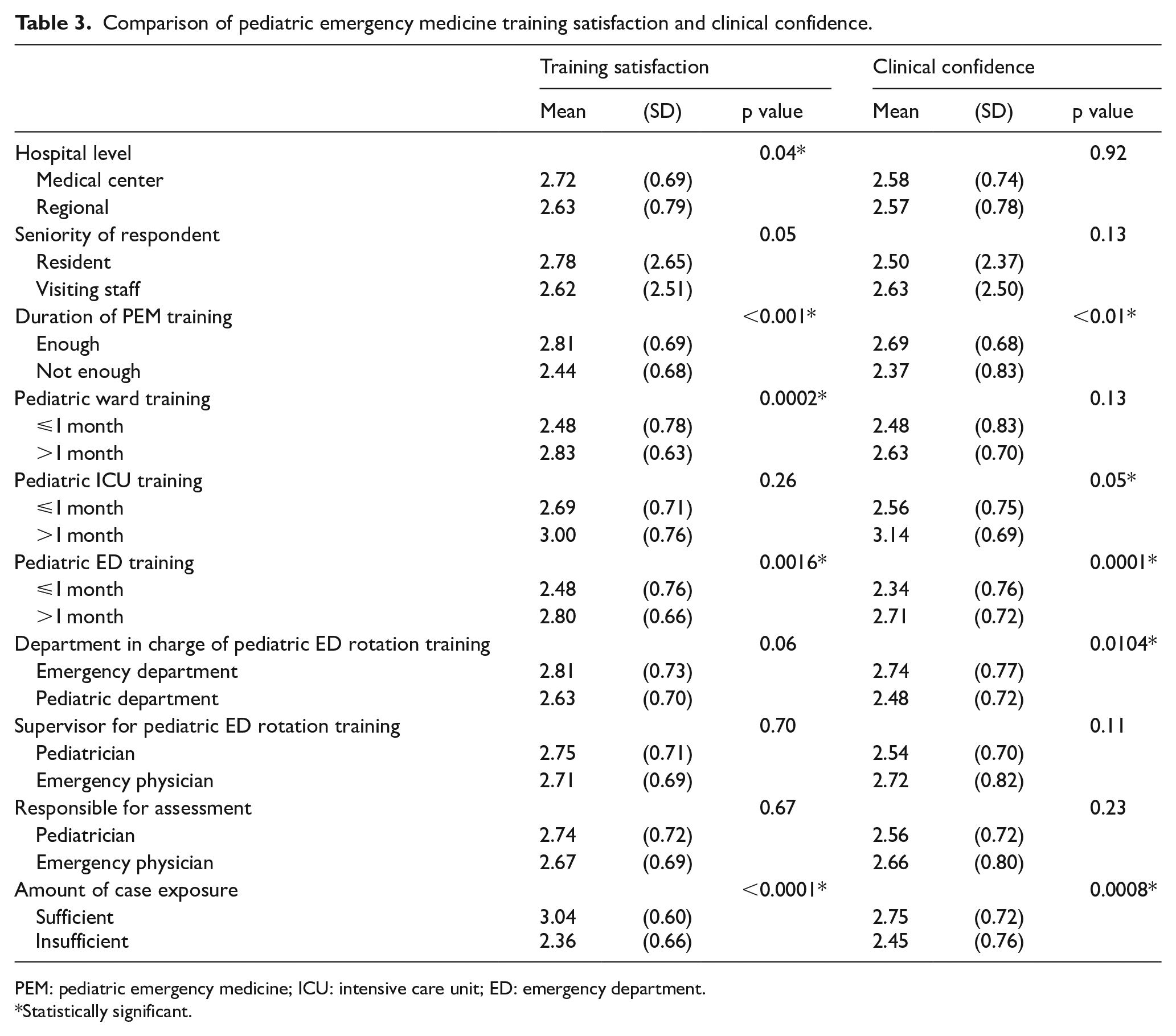
PEM: pediatric emergency medicine; ICU: intensive care unit; ED: emergency department.
Statistically significant.
Figure 1 shows the pediatric training satisfaction stratified by the seniority of the participants. Different levels of the satisfaction for received PED training decrease with seniority. Further correlation analysis was done to examine how site-specific satisfaction is associated with overall satisfaction (Table 4). The results showed that overall satisfaction with pediatric emergency training was associated with both pediatric ward training satisfaction (ρ = 0.392, p < 0.0001) and PED training satisfaction (ρ = 0.505, p < 0.0001). Only PED training satisfaction contributed to the overall confidence level (ρ = 0.333, p < 0.0001). The content analysis of the open-ended questions disclosed participants’ advice to strengthen the PEM training among EM residency program, which encompassed what training content needed to be added and which training model is preferred for best PEM learning (Table 5).
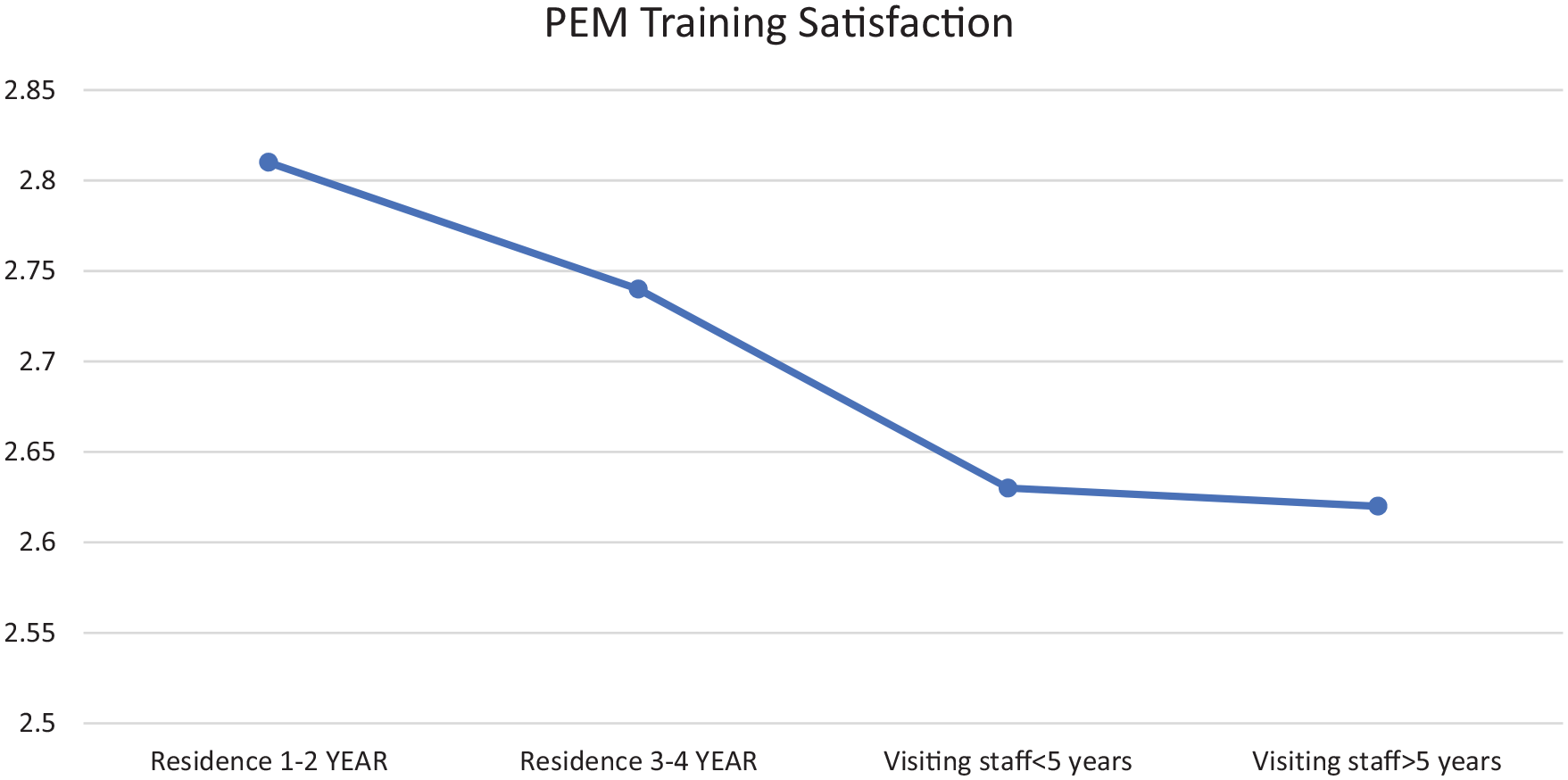
Pediatric emergency medicine training satisfaction, stratified by seniority of the participants.
Correlation of overall satisfaction and practice confidence with site-specific pediatric training satisfactions.
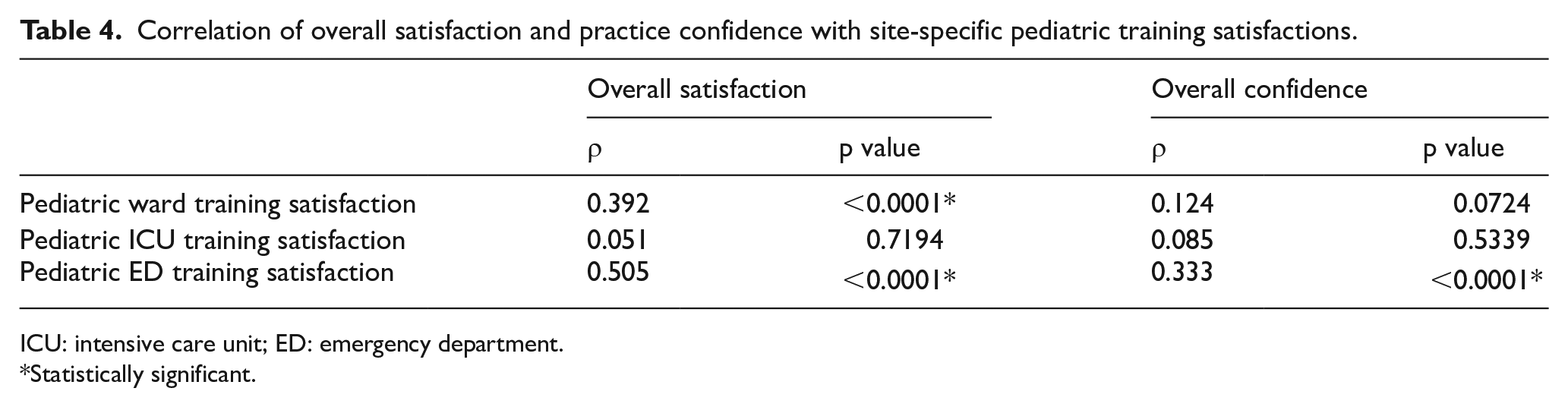
ICU: intensive care unit; ED: emergency department.
Statistically significant.
Content analysis of the open-ended questions about the advice to strengthen the training program.
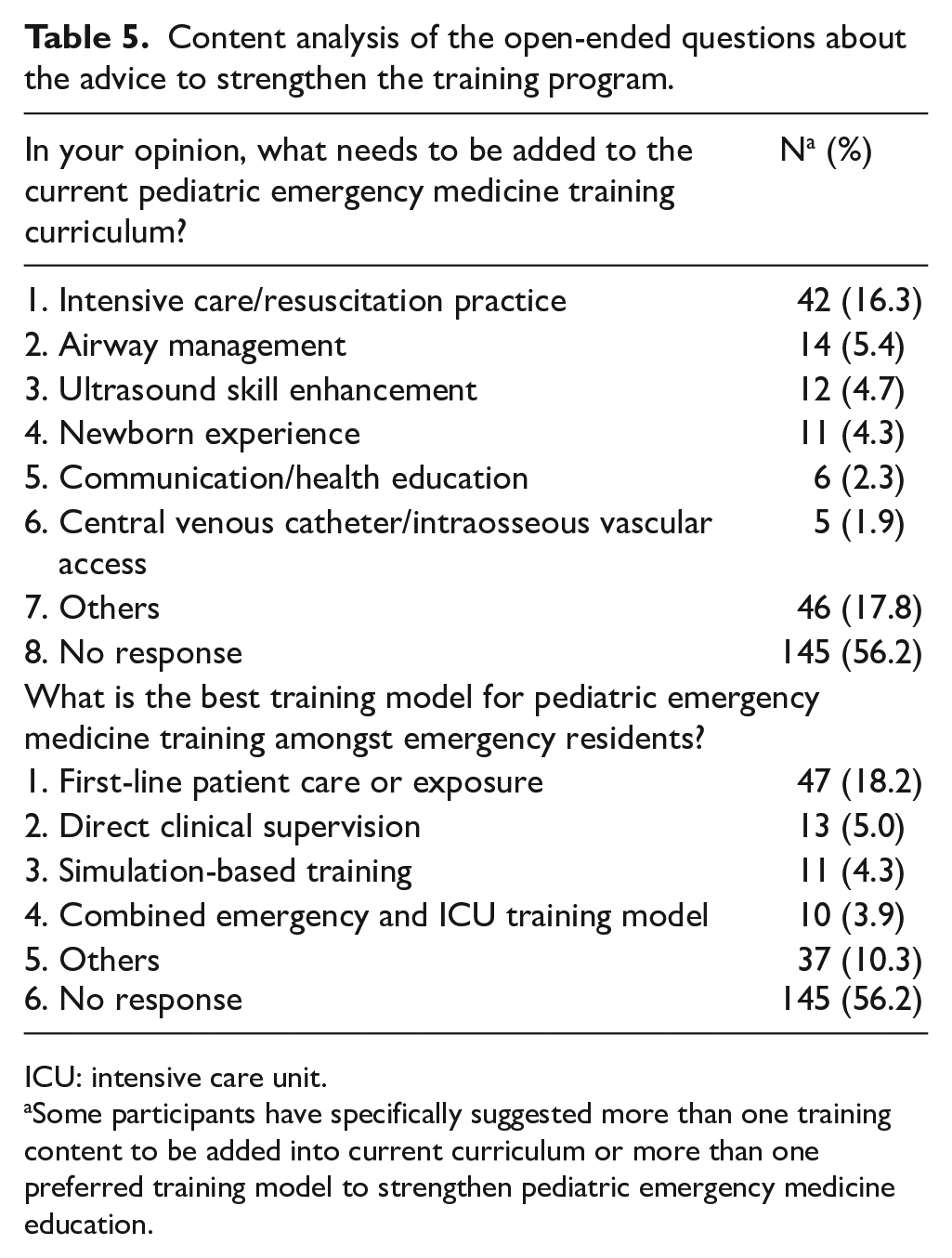
ICU: intensive care unit.
Some participants have specifically suggested more than one training content to be added into current curriculum or more than one preferred training model to strengthen pediatric emergency medicine education.
Discussion
This study is the first national survey about current PEM education in EM resident training programs in Taiwan. The participants enrolled in our study varied in their career stages and seniorities and thus offered a broad spectrum of opinions about how the PEM training has been conducted for EM residents in the past several decades and how this training contributed to trainees’ satisfaction with PEM training and confidence in clinical practice. The results are useful for further adjusting PEM training in the study country and may as well be applicable in other countries with similar PEM practice environments and training curricula.
Generally speaking, the overall satisfaction with PEM training and confidence in PEM clinical practice are adequate and are somewhat influenced by the duration of the training and the amount of case exposure. In our national survey, the total PEM training times are mostly around 4 months (9.5%; total EM training time: 42 months), including 2 months of pediatric ward rotation and 2 months of PED training. In contrast, the percentage of time spent in PEM training in Western countries was 13%–17% of the total training time of EM residency programs.1,3,25 The length of PEM training in EM residency programs varies with different health-care systems, contexts, or community needs,5,25,32 and pediatric readiness in the ED is always a concern.7,33 In our survey, 45.1% of the participants did not feel confident in clinical practice for pediatric patient care, and 49.4% considered their pediatric case exposure insufficient during their residency training. Most of the current PEM training in our EM residency programs include only 2 months of the pediatric ward and 2 months of PED rotations. This situation needs to be reformed. In EM training in other countries, rotations and electives usually included the PICU, the ED (general and pediatric), the pediatric ward, urgent care, the pediatric outpatient clinics, and the emergency medical service.5,25 In our study, over half of the participants would like to have had more PEM training, which might be related to limited case exposure and lack of confidence in their clinical practice in PEM. There is no universal consensus about the rotation training of PEM in the literature. However, the rotation length and pediatric case exposure issue among current EM residency programs still need to be examined because our rotation length/total EM training time is inappropriately lower than the proportion of pediatric patients to total EM visits. 30
In this study, more than 80% of the respondents were satisfied with the PEM training in all three usual training units, namely, pediatric ward, PED, and PICU. But the satisfaction with overall PEM education in EM training programs is only 58.5%. This gap highlighted that the satisfaction with the PEM training does not represent the sum of satisfaction of each clinical rotation. The satisfaction with PEM training among EM residency programs is determined by multiple factors. To keep up trainees’ core medical knowledge and develop their clinical skills and attitude in PEM, most EM training programs include core lectures, various case discussions, and clinical rotations, which are hard for EM residents to thoroughly experience if training time reserved for PEM is limited. Moreover, some training hospitals do not have faculties that specialize in PEM, and most participants did not get PICU or NICU rotations for caring for critically ill pediatric patients during their PEM training. In the ED, critical events involving children, while less frequent, may be especially distressing.4,34 This lack of experience in managing critically ill pediatric patients and in pediatric or neonatal resuscitation occurs worldwide.22,25,35 To compensate, proper clinical supervision, debriefing, feedback, or retrospective case discussion after pediatric critical events is important and effective to improve PEM training in the ED setting.36–38 Implementation of simulation-based training for EM residents is also essential in the clinical setting, in which pediatric case exposures are limited.35,39–42
Based upon our national survey data, the influential factors for training satisfaction are hospital level, training time, pediatric ward training, PED training, and the amount of case exposure. Enough training time, PED training, and the amount of case exposure also affect the trainees’ confidence in clinical practice in PEM. The hospital level at which participants train influences the satisfaction rate, which might be related to better clinical supervision, consultation, and enough case exposure. While analyzing the correlation of overall satisfaction and practice confidence with site-specific pediatric training, the PED rotation is the only determining factor for practice confidence (Table 4). In our survey, only 22.1% of trainees had ICU/NICU training in their EM residency training. In our analysis, the pediatric ICU rotation does not influence training satisfaction, but it dramatically impacts the residents’ confidence. Most of the participants in our study reported that they were not confident in critical care and pediatric/newborn resuscitation. This might also be related to limited experience in managing pediatric critical cases. Critical care and pediatric/newborn resuscitation are very important in PEM training. 25 The rotations in a PICU and urgent care serve as an effective way to supplement limited ED experience. 43 We suggest extending PED rotation lengths to enhance trainees’ practice confidence. We also recommend that PICU or NICU rotation training be regularly and essentially implemented into EM residency programs to fill the gap.
Compared to programs in Western countries, some parts of our EM residency programs can still be improved. Based upon the opinions of the participants in this study, the current training curriculum, which has been followed for two decades, needs to be strengthened with more training on intensive care/resuscitation practice (16.3%), airway management (5.4%), ultrasound skill enhancement (4.7%), and newborn experience (4.3%). The perceived effectiveness of the PEM training is better for newly registered EM residents compared to senior visiting staff members, which to some extent indicates that PEM training has improved in Taiwan in the past two decades (Figure 1). Moreover, our participants considered the determining factors of the best model of PEM training to be more first-line patient care or exposure (18.2%), direct clinical supervision (5%), and implementation of simulation-based training preparedness (4.3%). In our study, physicians in charge of PEM education are mainly emergency physicians or general pediatricians. Enhanced clinical supervision of EM trainees could improve patient and educational outcomes. 38 However, few PEM fellowship training curricula are available for EM residents in training, which might be one factor that influences good clinical supervision in general ED.
In the near future, our PEM training curriculum not only needs to be reformed by adding extended critical care rotations, pediatric emergency placements, and clinical skill training, but also needs to aggressively cultivate pediatric emergency educators. Novel teaching and learning methods such as simulation sessions,44–46 animal model drills,35,47–49 or ultrasound applications50–52 may be also incorporated into the current curriculum to improve the clinical competencies and preparedness of EM residents.
Limitations
This is a single cross-sectional national survey study, so cultural and contextual differences should be considered before generalizing the results to a different country or setting. In addition, the response rate is 20.14% of the total population. The relatively low response rate may be due to the nature of a national survey, emergency work culture, and lack of incentive, which could possibly influence the validity and transferability of the results.
Conclusion
The pediatric emergency training in EM residency training programs varies in intensive care training, clinical supervisors, and assessors. Our survey showed that the learning experience in pediatric wards and EDs rotations is associated with overall satisfaction with PEM training, while inadequate pediatric patient exposure in ED contributed to less confidence of EM learners. EM residency program reform might focus on adequate hands-on pediatric patient care in the ED, pediatric intensive care, and procedure skills training.
Footnotes
Acknowledgements
All authors acknowledged the contribution of the Committee on Pediatric Emergency Medicine of the Taiwan Society of Emergency Medicine for conducting cross-sectional online questionnaire survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The study data are available on request to the corresponding author (
Informed consent
The informed consent was waived by the IRB because the present study analyzed the results of anonymous questionnaire surveys.
Ethical approval
This study was approved by the local ethics boards: Chang Gung Medical Foundation Institutional Review Board (IRB No. 201800667B0D001).
Human rights
The present study did not include the patients.