
Abstract
Objective:
Computerized tomography remains the gold standard imaging in renal colic patients. In this study, we develop a scoring system to select patients in emergency department for unnecessary computerized tomography imaging in order to decrease radiation exposure.
Methods:
Computerized tomography imaging of patients with renal colic in emergency department were retrospectively reviewed. Symptoms, laboratory results were recorded. Significant parameters were determined by univariate and multivariate analysis. Coefficients were found to obtain score points and receiver operating curve was used to find a cut-off value.
Results:
A total of 123 patients with a mean age of 42 years (18–75 years) were enrolled in the study. About, 20.3% of patients were stone-free in computerized tomography. Mean stone size was 6.1 ± 1.89 mm. According to analysis, four parameters were significant; nausea, stone history, creatinine, and hematuria with a total score 9 called as Osmangazi University STONE score. Cut-off value was found as >3, which computerized tomography imaging is recommended.
Conclusion:
Osmangazi University STONE score is useful and simple tool in emergency department to reduce unnecessary computerized tomography imaging in renal colic patients and also lowers cost and ionizing radiation exposure.
Keywords
Introduction
In emergency departments (EDs), renal colic is a common type of complaint. In industrialized countries, about 0.6% of visits are because of ureteric colic. 1 Loin pain with colic pattern usually reflects a suspicion of stone disease. Mostly, symptoms or laboratory tests are not sufficient for the decision of intervention but they are very important for further evaluation. Some of these patients need intervention while some of them not. 10% of patients re-visit ED within 30 days although accurate diagnosis. 2 It is important to diagnose accurately for choosing the right patient whether intervention needed or follow up.
Medical imaging is an important issue for diagnosis especially in ED. In renal colic patients, computerized tomography (CT) is still the gold standard diagnostic imaging study. 3 Any other simple imaging or laboratory test could not replace CT up to now. Ultrasonography (US) alone or in other words, dilatation of the collecting system is not a reliable tool. 4 However, CT has its own disadvantages which are for the patients and healthcare systems. Radiation exposure is a big problem. Especially in clinical practice, a lot of imaging is done by doctors for diagnosis or follow up which may cause secondary malignancies. Radiologists are very sensitive to minimize this radiation exposure and we, clinicians, should attempt to reduce this exposure too. Also, cost of this method is another issue which particularly healthcare systems deal with.
In this study, we aimed to determine the exact patient for further evaluation with CT, with using a scoring system for an objective way.
Materials and methods
After the approval of local ethic committee, 26 December 2016, No: 04, a retrospective analysis was done between 1 January 2014 and 1 December 2016 for patients who were in ED in Osmangazi University Hospital. Patients’ ages between 18 and 75 years with renal colic were determined. Patients with CT evaluations were included, while without CT evaluations were excluded from the study. All symptoms and laboratory tests (urea, creatinine, hemogram, urine analysis, etc.) were recorded. Normal creatinine range was 0.7–1.2 mg/dL; over 1.2 was called higher creatinine level. Hematuria was called as >3 HPF (microscopic or macroscopic all hematuria was accepted as positive). CTs were re-evaluated whether stone exists or not. Familial stone disease and history of stone disease were added to the parameters. Due to the unreliable and missing results, US reports were excluded.
Statistical methods
Statistical methods were based on the methods used in the Framingham study. 4 All observations were included for the accurate estimates of coefficients to construct a scoring system. Multivariate logistic regression was performed to determine the odds ratio and the coefficients of the independent variables. For the scoring system, the coefficients of the independent variables obtained from multivariate logistic regression were adjusted by all coefficients and were divided by the smallest coefficient. Then to obtain score points, the adjusted coefficients were rounded to the nearest integer. Total score points were evaluated for each individual. Receiver Operating Characteristic (ROC) curve analysis was performed to obtain a cut-off value for the total scores. All statistical analysis was performed using IBM SPSS Statistics version 21.0.
Results
In total, 123 patients were included in the study. Mean age was 42 years (18–75 years). In CT examination, 20.3% of patients were stone-free, while 79.7% of patients had urolithiasis. Distribution of patients was summarized in Table 1 according to the presence of urolithiasis. Duration of pain and sex had no impact on CT outcomes (p = 0.13/0.06 and p = 0.2,1 respectively). Nausea, stone history, creatinine, and hematuria were significant parameters (all had p value <0.05) (Table 1).
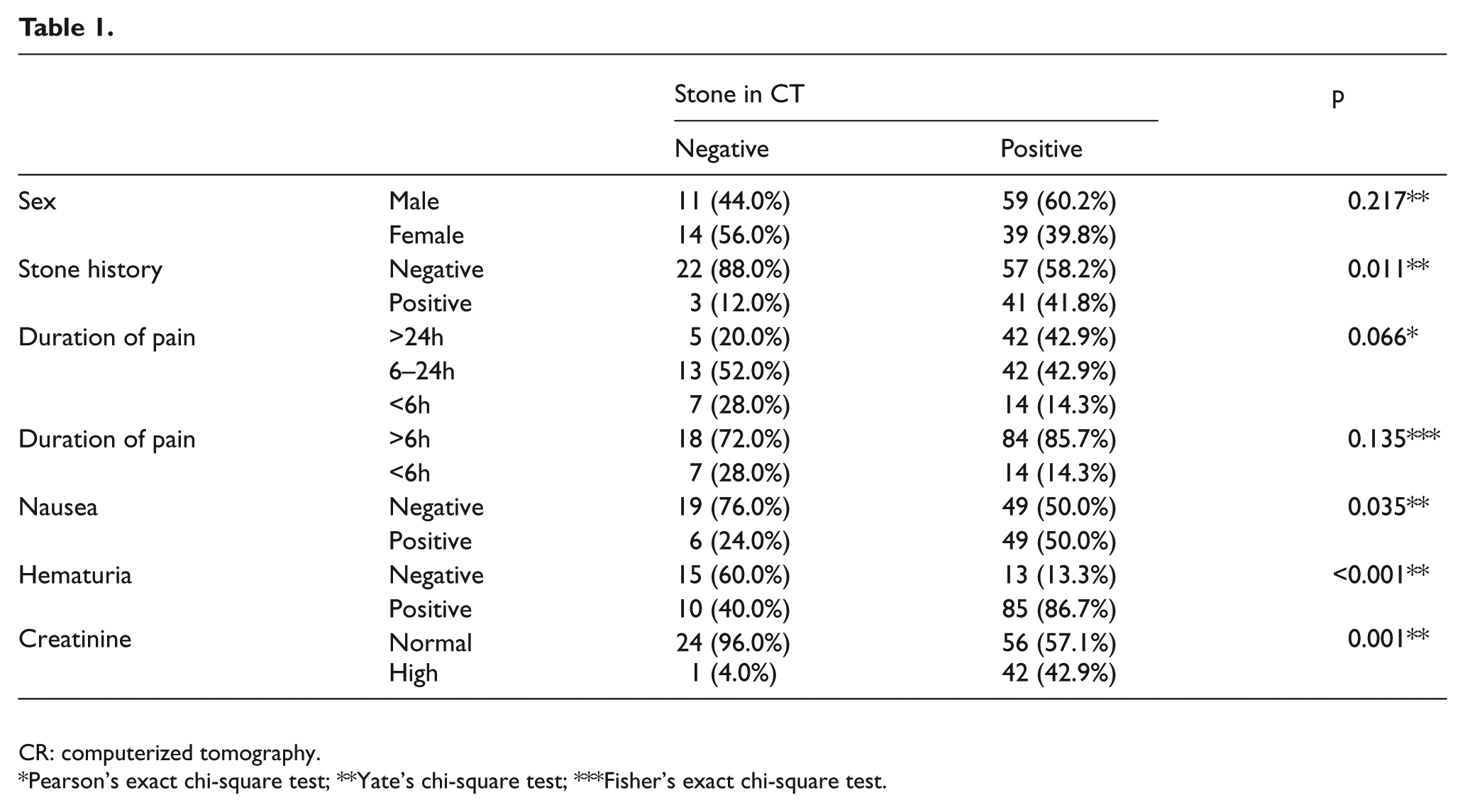
CR: computerized tomography.
Pearson’s exact chi-square test; **Yate’s chi-square test; ***Fisher’s exact chi-square test.
Construction of scoring system
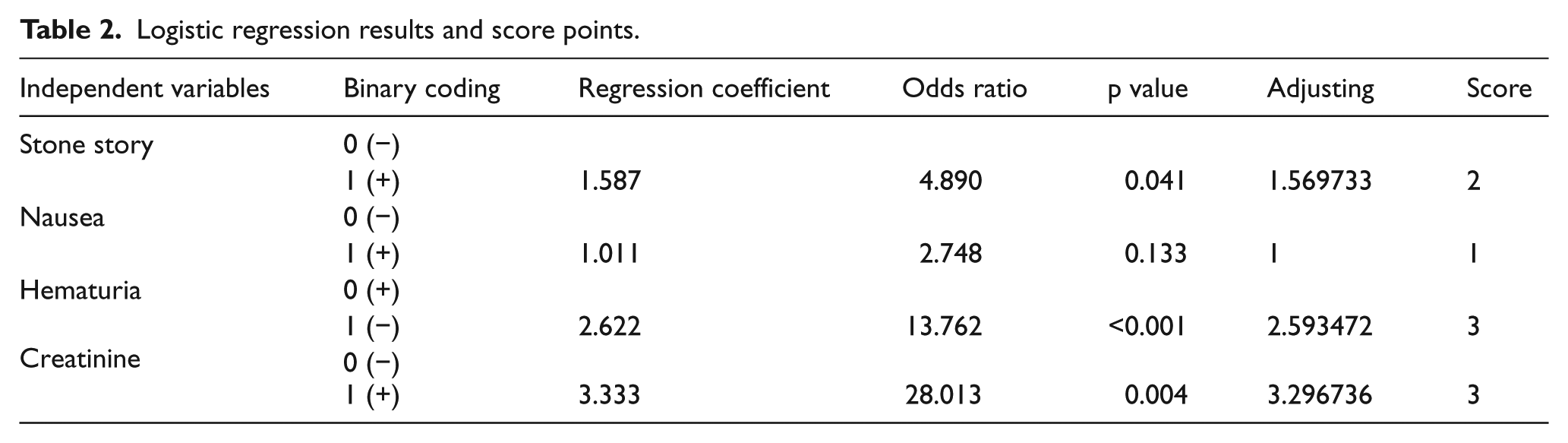
The CT results were used as a binary dependent variable (0: no stone, 1: having stone). Stone story, nausea, hematuria, and creatinine were taken as independent binary variables (0: negative, 1: positive) and logistic regression analysis was performed. As a result of the analysis, independent variables were scored according to the regression coefficients obtained (Table 2).
Logistic regression results and score points.
As a result of the analysis, cut-off value was found as over 3 points for the CT imaging with 0.88 AUC (area under curve) (Table 3).
ROC analysis.

ROC: Receiver Operating Characteristic; AUC; area under curve; SE: standard error; CI: confidence interval.
Discussion
The classic presentation for a patient with acute renal colic is the sudden onset of severe pain originating in the flank and radiating inferiorly and anteriorly; at least 50% of patients will also have nausea and vomiting. 5 Patients with urinary calculi may have infection or hematuria. Pain in the flanks is due to the passage of a stone from the ureter. First goal is to identify the exact diagnosis and second goal is to choose the patients who require intervention for stone diseases or other unrelated diagnosis. About, 37%–68% of patients diagnosed with stones were referred to the urologists from ED and interventions were needed for 15%–20% of them. 6 People with a history of urolithiasis have recurrence rates of 50% in 10 years. 7 Similarly, stone history correlated with positive CT in this study.
In literature, there are attempts to become new first-line imaging for US in renal colic patients. The reasons are concerns about ionizing radiation, cost, and easy-fast applicability. However, the results are not the same as we thought. Song et al. 8 demonstrated that in 11% of patients with ureteral stones showed no hydronephrosis in US. Also, hydronephrosis was shown in 13.9% of patients without stone disease in CT. Sternberg et al. 9 found that US did not accurately predict 25% of stone disease in CT. These findings are correlated with our study which the US could not reach to a significant level. Controversy to these studies and our study, Bindman et al. found that US was a discrimination power especially in high-risk diagnosis, complications. In that study, sensitivity for accuracy for diagnosis of nephrolithiasis was 85%. But also they were explaining their results do not suggest that patients should undergo only ultrasound imaging, but rather that US should be used as the initial diagnostic imaging test. 10 Parallelly, CT use is not associated with patient outcomes according to studies.11,12 Although our sensitivity score was lower; increased AUC, 0.88, in our study could be a promising parameter in future studies which will combine US and this scoring system.
CT has become first-line test for diagnosis of stone disease in US since 1996. Also CT imaging is widely used in whole world and use of CT in EDs has increased over 300% from 1996 to 2007. 13 Although it is a diagnostic advantage, radiation exposure is growing parallel. The mean effective doses were found 7.7mSv with unenhanced CT. A certain level of risk is always present with radiation exposure and is proportional to the level of exposure. Radiation risk is defined as the stochastic effect associated with the lifetime probability of a cancer fatality in the general population and the hereditary effects on the next generation. 14 Special concern has been raised regarding the relatively young population who present repeatedly with acute flank pain (repeated kidney stones), and who therefore undergo multiple radiologic examinations during their lifetime. This is important because there is direct radiation exposure to the female gonads, although only scatter radiation to male gonads. In order to minimize the radiation-induced cancer risk, imaging should be selected for appropriate patients. According to Moore et al., a non-kidney stone cause was found 9%–14% with a prevalence of symptomatic stones about 48% in CTs. 15 About 43% of cases were found no causes of pain. It looks like there is a big amount of unnecessary CTs and we should attempt to reduce ionizing radiation. Our scoring system is an attempt to show a reliable tool to reduce unnecessary imaging without diagnostic confusing. However, our study is not the first one in literature. Moore et al. presented their STONE score by using significant variables such as sex, duration of pain, origin, hematuria, and nausea-vomiting with a maximum score of 13. There were three risk groups: low 0–5, moderate 6–9, and high 10–13. They determined that if the score is high, a CT might be avoided or reduced dose CT could be an alternative. 16 As an opposite view, we still suggest to perform a CT imaging for the scores over 3 to avoid the delay of intervention requirement. STONE score was externally validated by Hernandez et al. 17 Due to 0% of Black patients in our study, we tried to explore a new scoring system rather than adopting STONE score (Appendix 1). Our study also needs an external validation.
Conclusion
In the last decade, CT became a popular imaging technique. Although its efficacy, especially in stone disease, increased, radiation exposure is a negative point of this technique. To avoid this radiation exposure, some modifications are needed. Our scoring system is an initial attempt with 69% sensitivity and 84% specificity to lower the CT imaging number. We expect our study to be a beginning point for studies with higher sensitivity and specificity.
Footnotes
Appendix
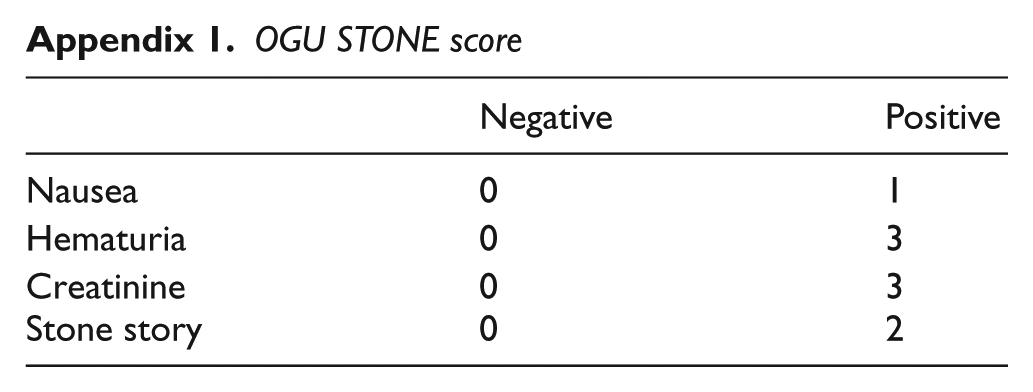
OGU STONE score
| Negative | Positive | |
|---|---|---|
| Nausea | 0 | 1 |
| Hematuria | 0 | 3 |
| Creatinine | 0 | 3 |
| Stone story | 0 | 2 |
Acknowledgements
B.B contributed to the design of this study. E. O., H. D., E. A., and N. A. contributed to the data collection. Statistics was contributed by M.B. and E.C.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Could be sent in SPSS format if requested.
Ethical approval
Local ethic committee (Osmangazi Univ Ethic Committee; date: 26 December 2016, No: 04. This study has been approved by our institutional review board (IRB) and has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.