
Abstract
Background
We aimed to compare the efficacy and safety of laparoscopic pyelolithotomy (LPL) versus percutaneous nephrolithotomy (PCNL) for treating renal stones larger than 2 cm.
Methods
We searched the PubMed, Embase, Web of Science, SinoMed, and Chinese National Knowledge Infrastructure databases for studies that compared the surgical outcomes of LPL and PCNL. We conducted a meta-analysis of the retrieved studies, expressed as weighted mean difference or risk ratios with 95% confidence intervals.
Results
We included 25 studies (1831 patients). LPL was associated with a significantly higher stone-free rate, lower rates of blood loss, complementary treatment, blood transfusion, and complications, and less reduction in hemoglobin level compared with PCNL. LPL and PCNL were similar in terms of duration of hospital stay, conversion rate, changes in glomerular filtration rate and creatinine level, and mean time of postoperative analgesia. However, LPL was associated with a longer operation time than PCNL.
Conclusion
LPL appears to be more effective and safer than PCNL in patients with large renal stones, by increasing the stone-free rate and reducing blood loss, complementary treatment, blood transfusion, and complications compared with PCNL. LPL may thus be a useful modality for treating patients with large renal stones.
Keywords
Introduction
Kidney stones are one of the most common benign urologic diseases and may lead to severe outcomes, such as obstructive uropathy, uronephrosis, and even uremia and tumors. 1 Surgery is therefore required to remove the stones and preserve normal urinary system function. Several therapeutic approaches have been widely used to treat patients with large renal calculi (>2 cm diameter), including shock wave lithotripsy, 2 percutaneous nephrolithotomy (PCNL), 3 open surgery, and laparoscopy. 4 PCNL is currently considered as the gold standard first-line treatment for the management of large renal stones. 5 However, although PCNL has a relatively high stone-free rate (SFR), it may lead to serious complications, such as bleeding and postoperative sepsis. 6 Moreover, PCNL may not be suitable for all patients with large renal stones, such as those with a complex stone burden or large staghorn stones. The treatment of large renal stones thus remains a challenging problem in urology.
In line with the development of laparoscopic surgical techniques, laparoscopic pyelolithotomy (LPL) is increasingly being used as a treatment option for renal calculi. 7 According to the European Association of Urology guidelines, the definite indications for LPL of kidney stones are limited to the following situations: (1) failed endoscopic procedure; (2) complex stone burden, renal and anatomical abnormalities; and (3) indications for open surgery. 8 Although three previous meta-analyses9–11 assessed the efficacy and safety of LPL and PCNL in patients with large renal stones, they produced inconsistent results. Furthermore, none of the studies included Chinese publications or provided data relevant to Chinese urologists. Additional clinical trials have also recently been published, re-evaluating the comparative efficacy and safety of LPL and PCNL for treating large renal stones. We therefore performed an updated meta-analysis including Chinese studies, to enable the critical comparison of LPL and PCNL in terms of their efficacy and safety for the management of large renal stones.
Methods
Search strategy
We conducted this meta-analysis in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 12 We searched the PubMed, Embase, Web of Science, SinoMed (Chinese BioMedical Literature Service System), and Chinese National Knowledge Infrastructure (CNKI) databases from their inception to April 17, 2020, with no language restrictions. The search terms were as follows: ((“kidney pelvis”[MeSH Terms] OR (“kidney”[All Fields] AND “pelvis”[All Fields]) OR “kidney pelvis”[All Fields] OR (“renal”[All Fields] AND “pelvic”[All Fields]) OR “renal pelvic”[All Fields]) AND (“calculi”[MeSH Terms] OR “calculi”[All Fields])) AND ((“laparoscopy”[MeSH Terms] OR “laparoscopy”[All Fields] OR “laparoscopic” [All Fields]) AND pyelolithotomy[All Fields]) AND (“nephrolithotomy, percutaneous”[MeSH Terms] OR (“nephrolithotomy”[All Fields] AND “percutaneous”[All Fields]) OR “percutaneous nephrolithotomy”[All Fields] OR (“percutaneous”[All Fields] AND “nephrolithotomy”[All Fields])). We also manually searched related systematic reviews and meta-analyses, and the reference lists of the included studies to identify potential eligible studies. Discrepancies were resolved by discussion and consensus between the two investigators (TM and NW).
This study was a meta-analysis using previously published data, and ethical approval was therefore not required.
Selection criteria
Studies were included in our meta-analysis if they met the following criteria: (1) randomized controlled trial (RCT), cohort study, or case-control study; (2) adult patients with large renal calculi (≥2 cm); (3) intervention group LPL; (4) comparison group PCNL; and (5) outcomes SFR, operation time, duration of hospital stay, blood loss, postoperative analgesia, mean reduction in hemoglobin, mean change in total glomerular filtration rate (GFR), conversion to open surgery, and complications. If several publications reported on the same population, we only included the latest one with the most information. Reviews, editorials, comments, and letters were excluded from this analysis.
Data extraction
A standard data-extraction sheet was constructed based on the Cochrane Consumers and Communication Review Group data extraction template. The following data were extracted and entered using this sheet: first author’s name, year of publication, study design, location, number of patients in each group, patient characteristics (age, sex, mean stone size), and outcome measures (SFR, operation time, duration of hospital stay, blood loss, postoperative analgesia, mean reduction in hemoglobin, mean change in total GFR, conversion to open surgery, and complications).
Methodological quality assessment
For RCTs, we assessed the risk of bias using the method recommended by the Cochrane Collaboration. 13 This method evaluates the quality of the study based on five items: blinding, method of randomization, allocation concealment, follow-up, and intention-to-treat analysis. 13 Each study was classified as having a high, low, or unclear risk of bias.
The methodological quality of non-randomized studies (cohort or case-control studies) was assessed using the modified Newcastle–Ottawa scale (NOS), 14 which includes three items: patient selection, comparability of intervention/control group, and outcome assessment. 14 The total available NOS score was 9 points, with a higher score indicating better quality. 14 Studies with >5 points were considered high quality.
Statistical analysis
We analyzed the data using Stata version 12.0 (Stata Corporation, College Station, TX, USA). Dichotomous variables were expressed as risk ratio (RR) with 95% confidence intervals (CIs), and continuous variables were expressed as weighted mean difference (WMD) with 95%CIs. Before the data were synthesized, we tested for heterogeneity among the included studies using the Cochrane Q and I2 statistics, 15 with a P value <0.10 or I2 > 50% defined as significant heterogeneity. Pooled estimates of RR or WMD were calculated using a fixed-effects model (Mantel–Haenszel method) 16 or a random-effects model (DerSimonian–Laird method), 17 depending on the heterogeneity among the included studies. In the event of heterogeneity, we conducted sensitivity analysis by omitting each study in turn to explore its influence on the overall risk estimate. We also performed subgroup analyses based on stone features, study design, and country, to explore the sources of heterogeneity and the impacts of these variables on the overall estimates. We performed cumulative meta-analysis to assess the evolution of evidence for LPL effectiveness over time. The studies were sorted by year and the effect estimates of the studies were added to the pooled estimates of the studies accrued up to that date. A random-effect model was used for the cumulative meta-analysis. Publication bias was assessed by Begg’s 18 and Egger’s tests. 19 A two-tailed P value <0.05 was considered statistically significant, except where a certain P-value was specified.
Results
Identification of eligible studies
The initial search identified 2156 relevant publications. Among these studies, 1337 were excluded because of duplicate records and 791 were excluded after reviewing the abstract and title. Twenty-eight studies were therefore subjected to full-text information review, of which two were excluded because they compared PCNL with other surgical treatments, and one because it was unrelated to our topic. Twenty-five studies3,20–43 including 1831 patients finally met the inclusion criteria and were included in this meta-analysis (Figure 1).

Eligibility of studies for inclusion in the meta-analysis.
Characteristics of eligible studies
The main characteristics of included studies are presented in Table 1. All the studies were published between 2001 and 2019. The sample sizes ranged from 20 to 198. There were nine RCTs and 16 prospective or retrospective cohort studies. Eleven studies were conducted in China, five in India, two in Turkey, two in Iran, and the remaining five in Kuwait, USA, Egypt, Korea, and France, respectively. Staghorn calculi were reported in four studies,20,26,27,43 solitary renal pelvic stones in 20 studies,3,21–25,29–31,33–43 multiple pelvic stones in one study, 28 and pelvic and calyx stones in one study. 32 The baseline characteristics of the populations, including age, sex, and body mass index, were comparable between the LPL and PCNL groups. The mean stone size in all studies was larger than 2 cm, and was comparable between the two groups.
Baseline characteristics of patients in the trials included in the meta-analysis.

LPL, laparoscopic pyelolithotomy; PCNL, percutaneous nephrolithotomy; RCT, randomized controlled trial; SD, standard deviation; NA, not available; NR, not reported; NOS, Newcastle–Ottawa score.
Quality assessment
All the included RCTs were considered to have a high risk of bias because it was not possible to blind the patients and medical personnel to the type of surgery.
The median NOS score for the non-RCTs was 6 points (range 5–7), indicating that these studies were high quality (Table 1).
SFR
Twenty-one studies reported the SFR.3,20,22–29,31,32,34–36,38–43 The SFRs in the LPL and PCNL groups were 96.0% and 82.3%, respectively. Pooled estimates showed that LPL was associated with a significantly higher SFR than PCNL (RR = 1.14, 95%CI: 1.08, 1.20; P < 0.001) (Figure 2). The test for heterogeneity was significant (I2 = 62.3%, P < 0.001) and we therefore performed sensitivity analysis to explore the potential source of heterogeneity. Excluding one trial with a small sample size (n = 20) 31 did not change the overall estimate substantially (RR = 1.15, 95%CI: 1.11, 1.19; P < 0.001), but the heterogeneity remained (I2 = 60.9%, P < 0.001). However, excluding one trial with outliers 38 altered the result slightly (RR = 1.13, 95%CI: 1.10, 1.17; P < 0.001), but removed the heterogeneity (I2 = 44.7%, PP = 0.019). This indicated that the trial conducted by Yu et al. 38 contributed to the heterogeneity across the included studies.

Forest plot comparing laparoscopic pyelolithotomy and percutaneous nephrolithotomy in terms of stone-free rate. Studies are listed by first author’s name.
Operation time
Twenty-four studies reported data on operation time.3,20–37,39–43 The mean operation times in the LPL and PCNL groups were 119.72 ± 33.67 and 92.23 ± 23.41 minutes, respectively. LPL was associated with a significantly longer operation time than PCNL (WMDP = 31.19 min, 95%CI: 22.50, 39.89; P < 0.001) (Figure 3). The test for heterogeneity was significant (I2 = 94.2%, P < 0.001), and sensitivity analysis by excluding each single study did not change the overall estimate or heterogeneity substantially.

Forest plot comparing laparoscopic pyelolithotomy and percutaneous nephrolithotomy in terms of operation time. Studies are listed by first author’s name.
Duration of hospital stay
Twenty-two studies reported data on hospital stay.3,20–27,29–36,39–43 The mean durations of hospital stay in the LPL and PCNL groups were 4.59 ± 1.67 days and 4.83 ± 1.42 days, respectively. The pooled results indicated that patients treated with LPL and PCNL had similar durations of hospital stay (WMDP = −0.28 days, 95%CI: −0.84, 0.27) (Figure 4). The test for heterogeneity was significant (I2 = 95.0%, P < 0.001). Excluding the trial with a small sample size (n = 20) 31 changed the overall estimate, resulting in a significantly shorter duration of hospital stay in the LPL group (WMDP = −0.88 days, 95%CI: −1.00, −0.76; P < 0.001), but the heterogeneity remained (I2 = 95.3%, P < 0.001). Excluding the trial with outliers 41 also affected the overall estimate (WMDP = −0.75 days, 95%CI: −0.87, −0.63; P < 0.001), but did not remove the heterogeneity (I2 = 94.0%, P < 0.001).

Forest plot comparing laparoscopic pyelolithotomy and percutaneous nephrolithotomy in terms of duration of hospital stay. Studies are listed by first author’s name.
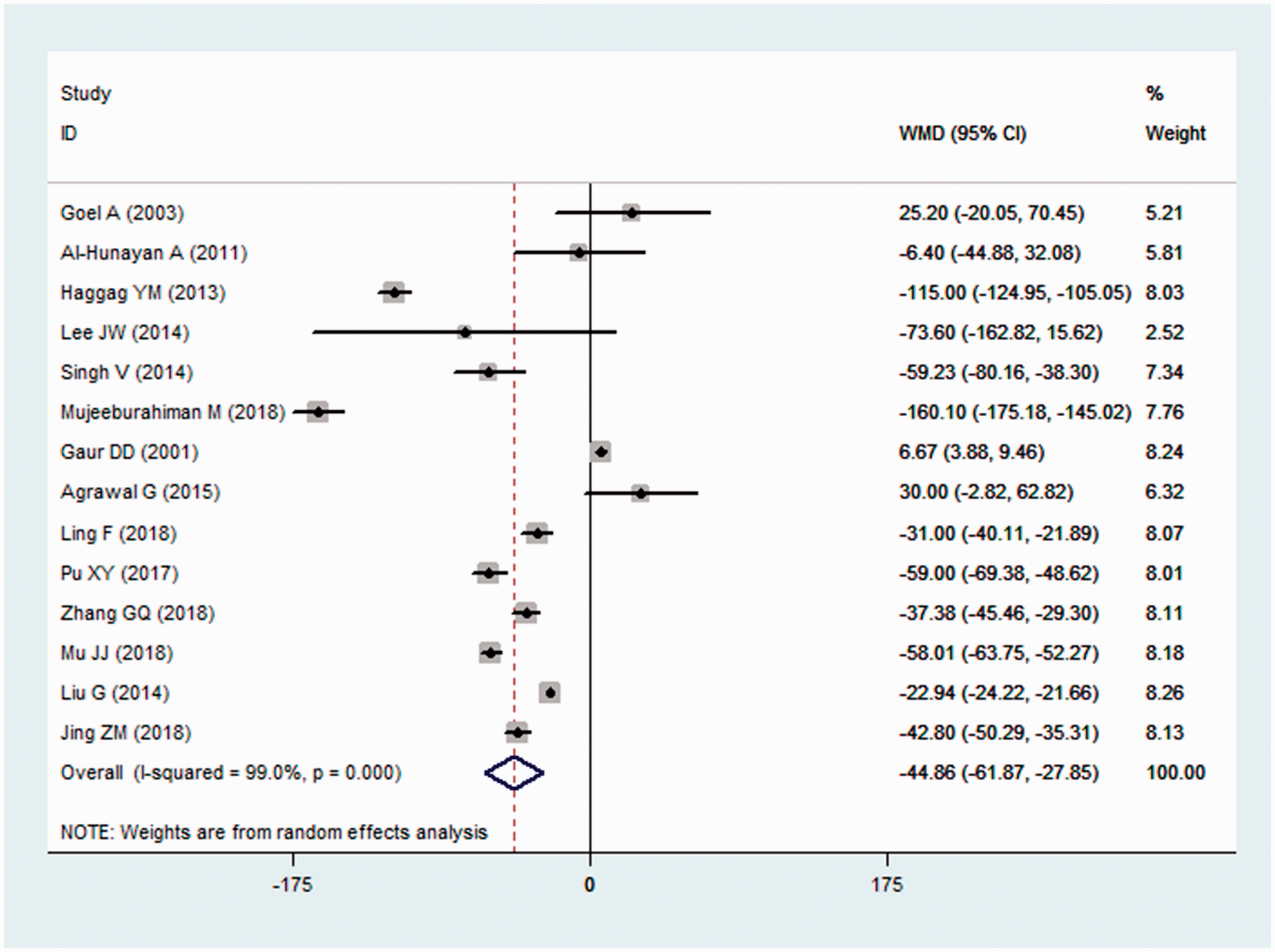
Estimated blood loss
Fourteen studies reported data on blood loss.21,22,24,26,28,31–36,40–42 The mean estimated blood losses in the LPL and PCNL groups were 81.25±34.37 mL and 124.37±45.45 mL, respectively. LPL was associated with significantly less blood loss than PCNL (WMDP = −44.86 mL, 95%CI: −61.87, −27.85; P < 0.001). The test for heterogeneity was significant (I2 = 99.0%, P < 0.001), and sensitivity analysis excluding each individual study did not meaningfully change the magnitude of the overall estimate.
Conversion to open surgery and complementary treatment
Eight studies reported data on conversion to open surgery.20–22,27,30,32,33,37 The conversion rates in the LPL and PCNL groups were 4.84% and 2.19%, respectively, indicating similar conversion rates in both groups (RR = 1.89, 95%CI: 0.88, 4.06). There was no significant heterogeneity among the included studies (I2 = 0.0%).
The rates of use of complementary treatments in the LPL and PCNL groups were 9.84% and 30.91%, respectively. The pooled estimate indicated that patients treated with LPL had a significantly lower rate of complementary treatments compared with the PCNL group (RR = 0.32, 95%CI: 0.14, 0.75; PP = 0.008). There was no evidence of heterogeneity among the included studies (I2 = 0.3%).
Blood transfusion
Eight studies reported data on blood transfusions.20,22,24,25,27,35,37,43 The blood transfusion rates in the LPL and PCNL groups were 1.8% and 7.39%, respectively. LPL was associated with a significantly lower rate of blood transfusion than PCNL (RR = 0.31, 95%CI: 0.15, 0.65; PP = 0.015). The test for heterogeneity was not significant (I2 = 0.0%).
Mean changes in hemoglobin, total GFR, and creatinine
Eleven studies reported data on mean decrease in hemoglobin.3,20,23,25–27,29,30,36,39,43 The mean decreases in the LPL and PCNL groups were 2.62 ± 2.34 g/dL and 5.18 ± 3.42 g/dL, respectively. The mean decrease in hemoglobin level was significantly lower in the LPL group compared with the PCNL group (WMDP = −1.20 g/dL, 95%CI: −1.72, −0.68; P < 0.001). The test for heterogeneity was not significant (I2 = 8.4%).
The mean changes in total GFR were 7.13 mL/minute for LPL and 3.43 mL/minute for PCNL. The mean changes in total GFR were similar in the LPL and PCNL groups (WMDP = 4.43 mL/minute, 95%CI: −0.37, 9.24).
The mean changes in creatinine level were −0.03 mg/dL for LPL and −0.01 mg/dL for PCNL. The pooled estimate showed that the changes were similar in both groups (WMDP = −0.03 mg/dL, 95%CI: −0.11, 0.04).
Postoperative analgesia
Six studies reported data on the use of postoperative analgesia.22,24,33,35,36,42 The mean durations of postoperative analgesia in the LPL and PCNL groups were 2.06 ± 0.70 days and 2.10 ± 0.70 days, respectively. These durations were comparable between the two groups (WMDP = −0.11 days, 95%CI: −0.22, 0.01). There was no significant heterogeneity among the included studies (I2 = 0.0%).
Complications
Thirteen studies reported eligible data on complications.3,24–26,29,32,33,35,36,40–43 The complication rates in the LPL and PCNL groups were 27.0% and 38.0%, respectively. The complication rate was significantly lower in the LPL compared with the PCNL group (RR = 0.69, 95%CI: 0.58, 0.83; PP = 0.005).
Among the common adverse events, LPL was associated with a significantly lower incidence of postoperative fever than PCNL (RR = 0.44, 95%CI: 0.25, 0.76; PP = 0.004), but similar incidences of uncontrolled bleeding (RR = 0.14, 95%CI: 0.01, 2.73) and prolonged urine leakage (RR = 7.00, 95%CI: 0.37, 133.57) (Table 2).
Summarized risk ratios for complications between laparoscopic pyelolithotomy and percutaneous nephrolithotomy.

RR, risk ratio; CI, confidence interval.
Cumulative meta-analysis of SFR
We performed a year-wise cumulative meta-analysis to compare LPL and PCNL in terms of SFR. Comparative SFR data were available from the year 2001, and further studies slightly changed the overall effect size without changing the magnitude or direction of the estimates (Figure 5). The CIs for overall effect size were broader in the years 2013 and 2014, but the addition of estimates from new studies reduced the CI while the overall estimate remained relatively stable (1.08–1.15). This confirmed the reliable and significant advantage of LPL over PCNL in terms of SFR.
Forest plot showing the cumulative meta-analysis for stone-free rate. Studies are listed by first author’s name.
Subgroup analysis
The results of subgroup analyses based on stone features, study design, and country are presented in Table 3.
Subgroup analysis based on study design and country for outcomes between laparoscopic pyelolithotomy and percutaneous nephrolithotomy.

Data expressed as overall estimate, (95% confidence interval), P value. RCT, randomized controlled trial.
Publication bias
There was no significant publication bias among the included studies (Egger’s test: tP = −0.37; Begg’s test: ZP = 0.39).
Discussion
This meta-analysis compared the efficacy and safety of LPL and PCNL for the treatment of patients with large renal stones. The results suggested that LPL was associated with significantly higher SFR, longer operation time, less blood loss, lower rates of complementary treatment, blood transfusion, and complications, and less reduction in hemoglobin level compared with PCNL. However, LPL had no benefit in terms of duration of hospital stay, conversion rate, mean changes in GFR and creatinine level, and mean duration of postoperative analgesia.
Several previous meta-analyses10,11,44 have compared LPL with PCNL for the management of large renal stones. All found that LPL was associated with a higher SFR, less decrease in hemoglobin level, and lower rate of postoperative fever compared with PCNL. The current meta-analysis expanded on these earlier studies by better characterizing the evidence base for LPL in patients with large renal stones. First, we included more studies with large sample sizes than the previous studies, which enhanced the statistical power for comparing surgical outcomes between LPL and PCNL. The latest date for studies included in the previous meta-analyses was September 2015, with 766 patients enrolled in the 13 included studies. In comparison, the current meta-analysis included 25 studies with 1831 patients, making the results more precise and persuasive. Second, we performed subgroup analyses based on stone features, study design, and country, which were not analyzed in the previous meta-analyses. We also searched several Chinese databases and included Chinese articles in our meta-analysis, thus providing valuable information for Chinese urologists. Third, we performed a cumulative meta-analysis to assess the evolution of evidence for LRL effectiveness in relation to SFR over time, which was not addressed in the previously published meta-analyses.10,11,44 Fourth, we also evaluated the effects and safety of LPL and PCNL in terms of mean changes in GFR and creatinine level, and postoperative analgesia, which were not considered in the previous studies.10,11,44
The present meta-analysis indicated that LPL was associated with a significantly higher SFR than PCNL, consistent with the findings of the previous meta-analyses.9,10,44 This might be because most stones could be removed intact by LPL, whereas PCNL might leave some residual stones that could form nuclei for stone recurrence, thus requiring auxiliary procedures and retreatments to remove them. This would accordingly reduce the success rate. Several studies assessed the effects of LPL in patients with single renal stones and reported encouraging results. They found that LPL provided comparable results to PCNL for solitary pelvic stones.3,22 Moreover, several recent studies26,45,46 used LPL in patients with multiple renal stones. Salvadó et al. 45 reported a 100% SFR for LPL in four patients with multiple renal stones in different poles, while Lee et al. 26 found SFRs of 91.1% for LPL and 64.1% for PCNL for the management of multiple complex renal stones. However, the management of complex renal stones, such as staghorn stones and calyceal diverticular stones, remains challenging, 45 and LPL could be a useful option for patients with these types of stones.
In this study, LPL was associated with significantly longer operation time than PCNL. This result was in line with most of the included studies, but conflicted with the reported by Li et al., 27 who found a mean operation times of 90.87±33.4 minutes for LPL and 116.8±44.4 minutes for PCNL. 27 Operation time is influenced by many variables, including the type of approach, surgeon’s experience, and differences among individual patients and equipment used. 27 In view of these variables, Li et al. attributed the shorter operation time of LPL to the easier anatomical approach of LPL (retroperitoneal approach), with less involvement of the vascular anatomy than PCNL, and that the stones could be removed intact by LPL, thus reducing the likelihood of residual stones, as well as the operation time. 27
Compared with PCNL, LPL resulted in less blood loss in patients with large renal pelvic stones. LPL does not damage the renal parenchyma, thus reducing the risk of bleeding. In contrast, PCNL depends on the access location and dilation technique, and the risk of bleeding is thus higher. 27 Bleeding is the most important and frequent complication in patients undergoing PCNL. However, Goel et al. 21 found greater estimated blood loss in patients undergoing LPL compared with PCNL (173.1 (60–400) mL and 147.9 (75–200) mL, respectively), though the difference was not significant. 21 Similar results were observed in a cohort study conducted by Agrawal et al., 33 who reported greater mean blood loss in the LPL compared with the PCNL group (180.25±63.28 vs. 150.5 ± 34.06 mL, respectively), with no need for blood transfusion in any of the cases. 33
In terms of conversion rate, we found no significant difference between the two surgical approaches. This was in agreement with the previous meta-analyses by Wang et al. 9 and Wang et al. 10 Wang et al. 9 pooled data from 363 patients and found comparable conversion rates between LPL and PCNL (ORP = 1.72, 95%CI: 0.76, 3.88), while Wang et al. 10 also reported equal conversion rates between the two surgical modalities (RDP = 0.02, 95%CI: −0.01, 0.05).
Regarding complications, LPL was associated with a significantly lower incidence of complications than PCNL. There was a significantly higher incidence of postoperative fever in the PCNL group compared with the LPL group. Postoperative fever is a common medical complication associated with PCNL (23%–25%), and a small fraction of these febrile patients (1%–2%) develops urosepsis. 47 According to the previous review, the overall complication rate of PCNL was as high as 83%, including fever (21%–32.1%), transfusion (11.2%–17.5%), extravasation (7.2%), sepsis (0.3%–4.7%), and colonic injury (0.2%–0.8%). 48 These results suggest that LPL may be a more feasible modality than PCNL with respect to safety.
This study had several potential limitations. First, there was considerable heterogeneity among the included studies, which was not surprising given the differences in study designs, study populations, regions, surgical practices, equipment used, surgeons’ experience, and stone characteristics. These factors may have affected the results. However, we used a random-effect model to pool estimates, which could reduce the bias to some extent. Second, the relatively small sample sizes in some studies might have influenced our results, given that studies with small samples were more likely to overestimate the treatment effect than larger trials. Third, our results may have been biased because most of the included studies were retrospective cohort studies, and we therefore could not exclude the possibility of selection bias. Fourth, stone bulk was an important factor potentially influence the SFR. However, we were unable to calculate the SRF adjusted for stone bulk because of insufficient data across the included studies.
In conclusion, the present meta-analysis suggests that LPL might be more effective and safer than PCNL for the treatment of patients with large renal stones, by providing a higher SFR, less blood loss, and lower rates of complementary treatment, blood transfusion, and complications. LPL could be thus considered as a useful modality for removing large renal stones. However, more large-scale, prospective studies are needed to verify our findings and to explore the effects of LPL in patients with different types of renal stones.
Footnotes
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.