
Abstract
Background:
Cold weather has been known to cause various cold-related local injuries as well as accidental hypothermia.
Objectives:
The aim of this study is to investigate the basal characteristics, outcomes, and risk factors of patients with cold-related comorbidities using prospective emergency department–based surveillance system in high-risk area.
Methods:
We designed a prospective emergency department–based surveillance system throughout northern part of Gyeonggi province located in the northernmost of South Korea. A total of 20 emergency departments participated in the surveillance system. Patients who visited emergency department with cold-related comorbidities from 1 December 2012 to 28 February 2013 were prospectively enrolled in final analysis. We analyzed risk factors associated with outcome and correlation between climate factor (wind-chill index) and incidence.
Results:
During the study period, 54 patients with cold-related comorbidities were used for final analysis, including 35 hypothermia, 15 frostbite, and 4 trench foot. Among 35 patients with accidental hypothermia, 11 patients were admitted to intensive care unit and defined to have major adverse outcome. Hypothermic patient with major adverse outcome had lesser possession of coat as outwear when exposed to the cold (9.1% vs 58.3%, p < 0.01). Lower wind-chill index was likely to develop higher incidence of cold-related comorbidities (incidence rate ratio per 1°C decrease in wind-chill index: 1.086 (95% confidence interval: 1.038–1.135)).
Conclusion:
Patients with cold-related comorbidities were successfully monitored with emergency department–based surveillance system. Absence of coat was associated with major adverse outcomes in patient with accidental hypothermia. Lower wind-chill index was associated with higher incidence of cold-related comorbidities.
Introduction
Increasing impact of cold-wave on morbidity and mortality of general population is a major concern in public health. Cold environment can cause cold-related local injuries by freezing body tissue resulting in frostbite and trench foot and also cause accidental hypothermia, which could be fatal.1–4
To build effective strategies to prevent and manage cold-related comorbidities properly, it is crucial to be fully aware of the characteristics and risk factors of victims from cold-related comorbidities. There were several previous reports regarding the characteristics and risk factors of patients with accidental hypothermia and cold-related local injuries.2,5–12 However, most of these studies were based on retrospective autopsy reports of fatal cases and small number of patients or only extraordinary case reports of patients visiting emergency departments (EDs). In addition to our knowledge, characteristics of victims of accidental hypothermia and cold-related local injuries in South Korea have not been studied before.
The aim of this study is to investigate the basal characteristics, outcomes, and risk factors of patients with accidental hypothermia and cold-related local injuries as well as association between incidence of these morbidities and metrological factors using a prospective ED-based surveillance system in high-risk area with cold climate during winter.
Materials and methods
We designed a prospective ED-based surveillance system throughout northern part of Gyeonggi province in South Korea. A network consisting of 20 regional hospital–based EDs was built. Demographic and clinical information of patients with accidental hypothermia and cold-related local injuries were collected on a daily basis using the surveillance network. This study protocol was reviewed and approved by the Institutional Review Board of study site.
Surveillance network and participating EDs
Gyeonggi province is located at the most northern part of South Korea and therefore the coldest region in the country. All 21 EDs in northern Gyeonggi Province were initially enrolled for network setup. One ED could not participate in our surveillance network due to the lack of human resources. Finally, total of 20 regional EDs participated to set up the surveillance network (Figure 1). Because northern Gyeonggi Province is wide spread in shape, we decided to divide participating EDs into groups according to four districts to maintain homogeneity of meteoroidal data within district.
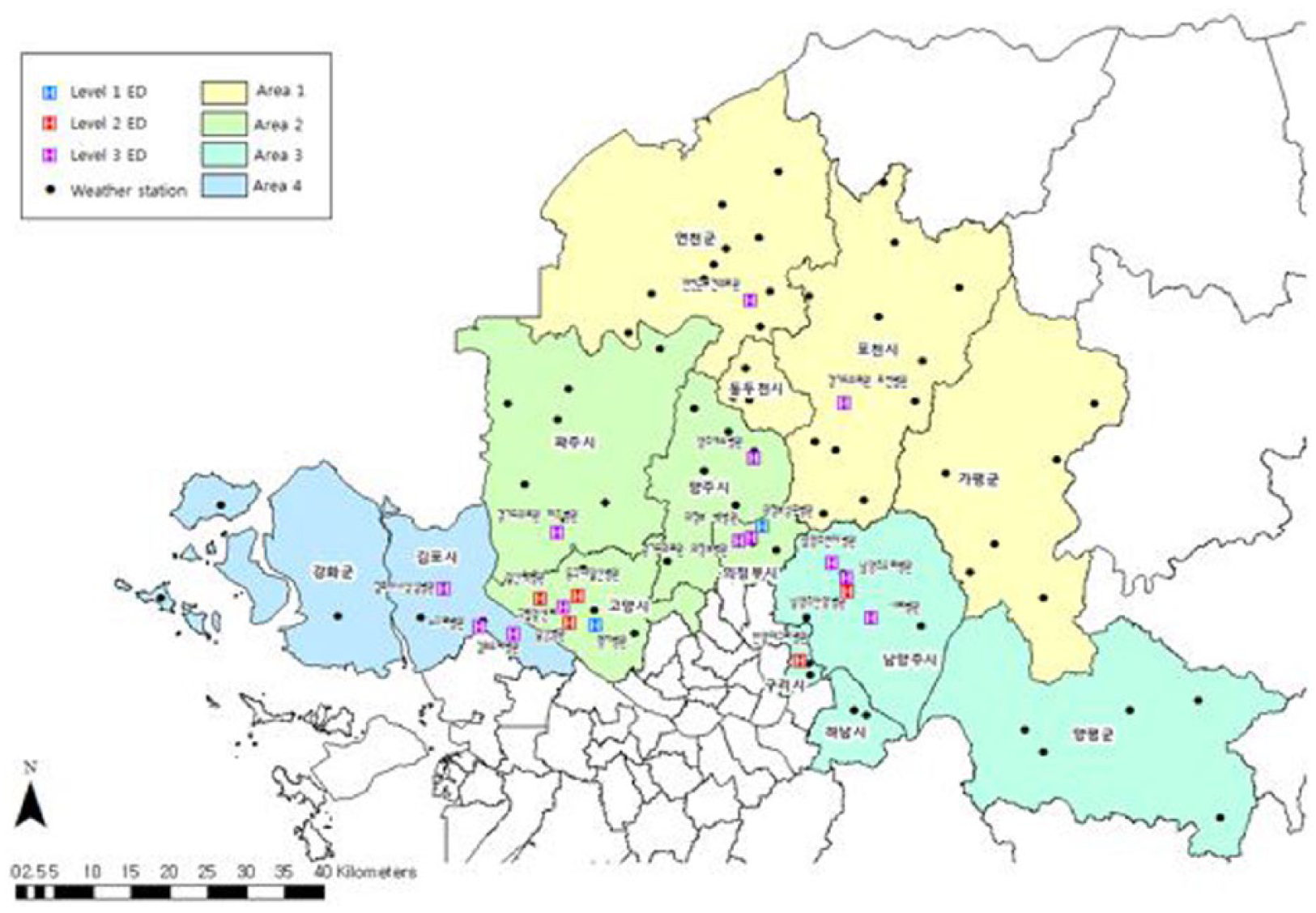
Map of the northern Gyeonggi province and emergency departments participated in surveillance.
All EDs in South Korea are designated by government as levels 1–3 based upon each ED’s human resources, essential instruments, and equipment. Among 20 EDs in the surveillance network, 2 EDs were level 1 centers, 10 EDs were level 2 centers, and 8 EDs were level 3 centers. At least three people for each ED were designated as surveillance personnel in charge of data gathering and transmission to central server, quality control of database, and overall system management, respectively. Person in charge of data gathering and transmission in each ED sent surveillance data collected in previous day to central server located in the Korea Centers for Disease Control and Prevention (CDC) through website before 10 a.m. of next morning at the latest. Prior to launching of surveillance system, these surveillance personnel in charge of data transmission were gathered to attend a 4-h training course regarding the purpose and structure of surveillance system as well as methods of filling out the registry.
Data collection
From 1 December 2012 to 28 February 2013, patients’ information was collected by the surveillance system. Inclusion criteria for patient enrollment were diagnosis of accidental hypothermia and cold-related local injuries. Accidental hypothermia was generally defined as core temperature less than 35°C.1,3 However, due to low accessibility of core temperature measurement in most of the participating rural hospital EDs, we decided to enroll all patients whose initial body temperature measured in ED were less than 35°C regardless of body part where temperature was measured (peripheral or core). Death on arrival patients who were hypothermic and those who were not accidentally hypothermic were excluded from surveillance. Cold-related local injuries included non-freezing localized cold injury (trench foot, chilblain) and freezing localized cold (1°~2° for superficial frostbite, 3°~4° for deep frostbite). Patients’ data collected by the surveillance system included demographic data such as age, sex, address, marital status, income, level of education, occupation, time of ED visit, type of insurance, and transportation to ED. Clinical data such as initial vital signs, injury site, ED result, admission results, and medical diagnosis were collected as well using hospital records. We also collected variables regarding known risk factors of cold-related local injuries and accidental hypothermia identified from literature review,1,8–10,12,13 including the underlying medical condition, alcohol and drug consumption, types of activities, homeless, or wearing warming outwears such as hats and coats.
Meteorological data
Daily minimal temperature and maximal wind speed of the four districts were obtained in order to calculate wind-chill index. Meteorological data measured by regional weather station was obtained from Korean Meteorological Administration (accessible from http://www.kma.go.kr). Wind-Chill index is well known to be associated with cold-related injuries. 14 In cold environments with temperatures below −10°C, wind speed increases the risk of cold-induced injuries. There is a high risk of frostbite at a wind-chill index of −25. Skin freezes in minutes at a wind-chill index of −45.14,15 Daily wind-chill index of each district was calculated and saved in central server for final analysis.
Statistical analysis
Basal characteristics of enrolled patients with cold-related local injuries and accidental hypothermia were analyzed. For patients with accidental hypothermia, subgroup analysis between patient group with major adverse outcome and patient group without major adverse outcome was performed. Death or being admitted to intensive care unit (ICU) was defined as major adverse outcome. Continuous variable were compared using student t-test. Categorical variables were compared using chi-square test. To clarify correlation between climate factor (wind-chill index), and incidence of cold-related local injuries or hypothermia, Poisson regression analysis was performed with incidence rate ratio (IRR) in 95% confidence intervals (CIs).
Results
A total of 60 patients with cold-related local injuries and accidental hypothermia were initially reported in the surveillance system. After reviewing all surveillance records, six patients including four patients whose records were duplicates, and two patients who were misdiagnosed as cold-related local injuries or accidental hypothermia were excluded in final diagnosis. After exclusion, surveillance records of 54 patients were enrolled for final analysis. Among the 54 patients, 35 were initially hypothermic at ED presentation and 19 patients were diagnosed with cold-related local injuries (4 deep frostbite, 11 superficial frostbite, and 4 trench foot). The basal characteristics patients with accidental hypothermia and each cold-related local injury are summarized in Table 1. The mean age of patients with hypothermia or deep frostbite was 52.9. For superficial frostbite and trench foot, the mean ages are relatively young (25.5 and 26.3 years, respectively). A total of 28.6% of patients with accidental hypothermia and 50.0% of patients with deep frostbite were homeless. A total of 57.1% and 75.0% of patients with accidental hypothermia and deep frostbite were drunk at the time of cold exposure. All patients with cold-related local injuries were on outdoor activity at the time of cold exposure. Only 2.9% of patients with accidental hypothermia were wearing hat and 42.9% were wearing coats at the time of cold exposure.
Characteristics of patient with hypothermia and cold-related local injuries.
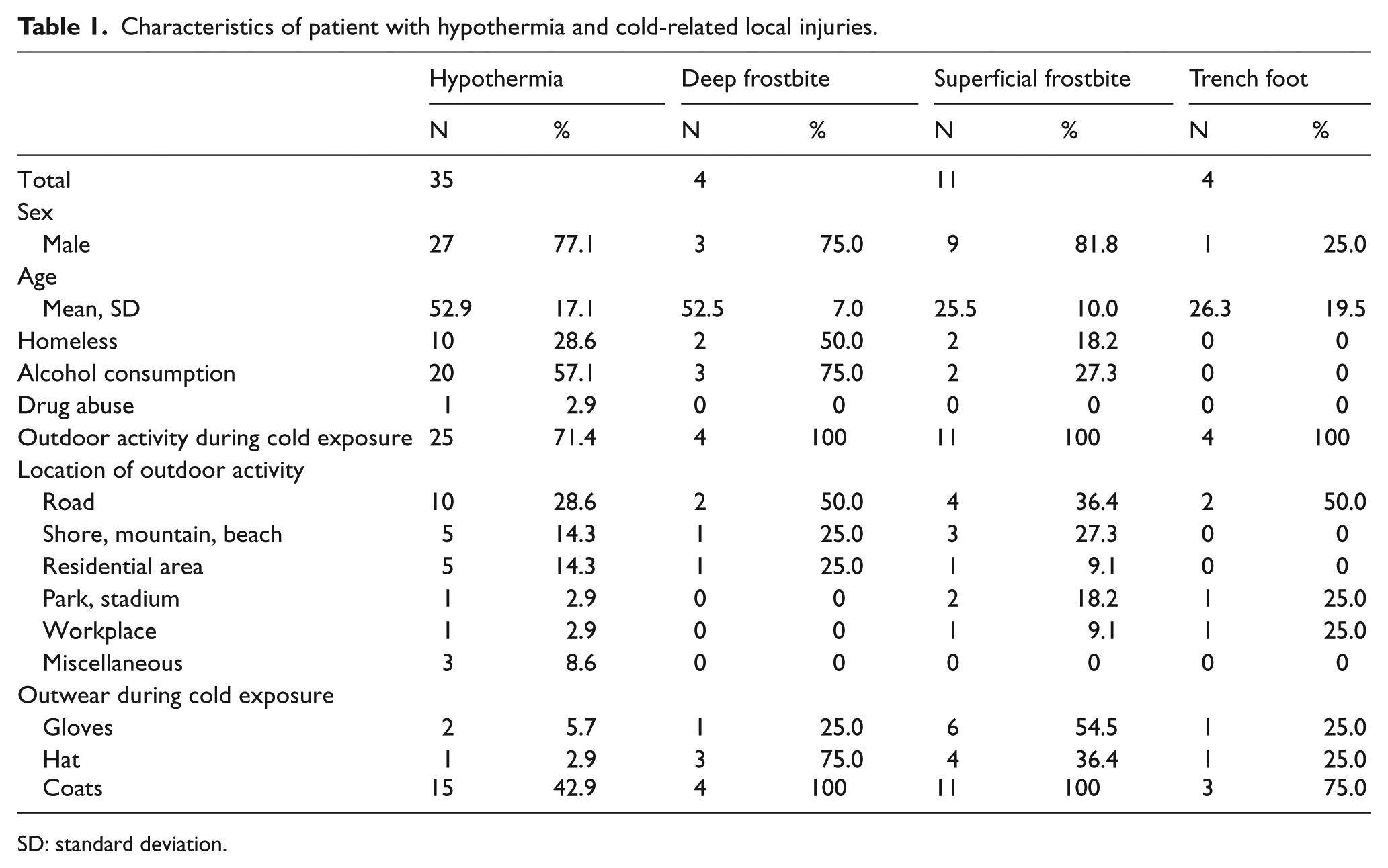
SD: standard deviation.
No patient with accidental hypothermia or cold-related local injuries died at ED during the surveillance period. A total of 14.3% of patients with accidental hypothermia and 50.0% of patient with deep frostbite were admitted to the general ward. And, 31.4% patients with accidental hypothermia were admitted to ICU for advanced intensive monitoring and management (Table 2).
ED results of patient with hypothermia and cold-related local injuries.
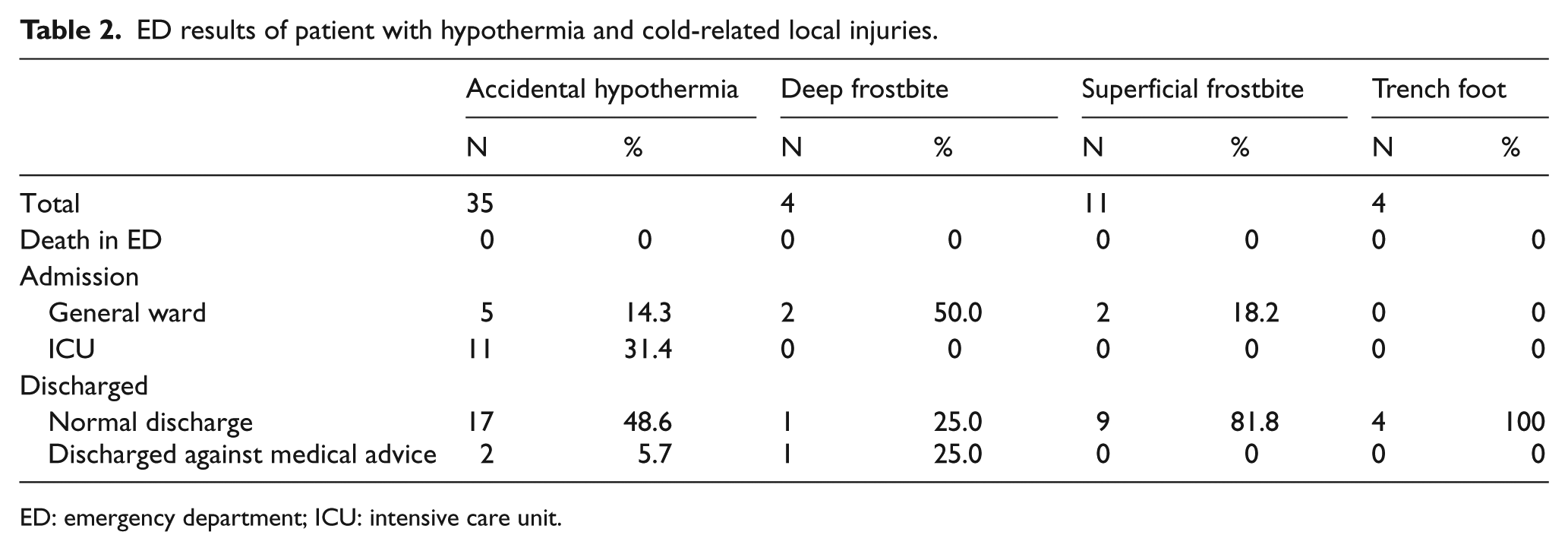
ED: emergency department; ICU: intensive care unit.
For 35 patients with accidental hypothermia, subgroup analysis was performed. They were divided into two groups depending on whether they had major adverse outcome as their ED results. Comparison between the two groups is summarized in Table 3. Results of comparison showed that hypothermic patients with major adverse outcome were hypotensive with lower level of consciousness at initial presentation compared to patients without major adverse outcome. Lesser proportion of patients with major adverse outcome consumed alcohol at the time of cold exposure (18.2% vs 75.0%, p < 0.01) and were wearing coats at the time of cold exposure (9.1% vs 58.3%, p < 0.01).
Comparison of patient with hypothermia according to ED results.
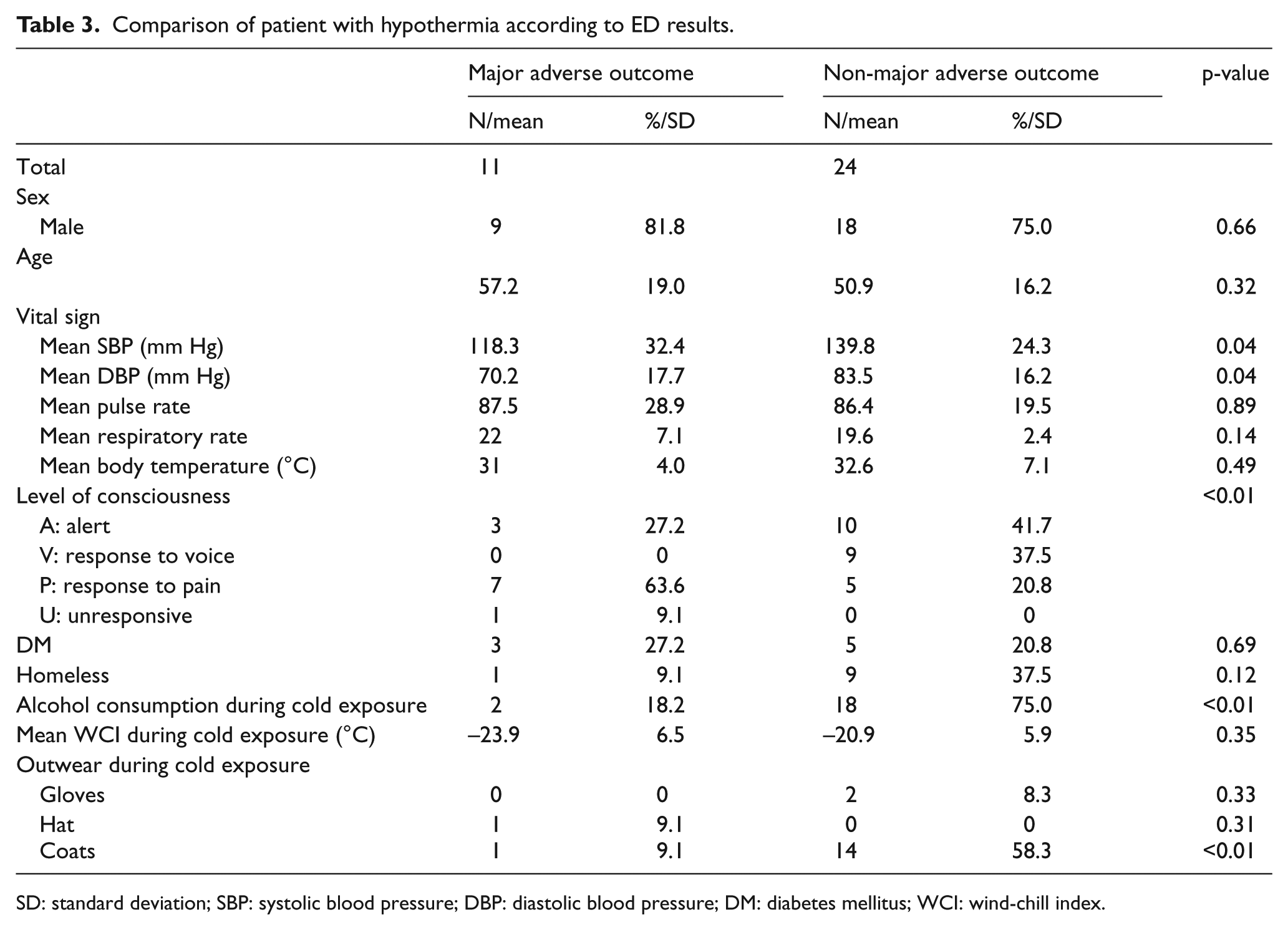
SD: standard deviation; SBP: systolic blood pressure; DBP: diastolic blood pressure; DM: diabetes mellitus; WCI: wind-chill index.
Wind-chill index during the entire surveillance period and the number of total reported cases of accidental hypothermia or cold-related local injuries plotted in Figure 2. In Poisson regression analysis, association between daily wind-chill index and reported patient number of accidental hypothermia or cold-related local injuries was shown. IRR for total cold-related comorbidities per 1°C decrease in wind-chill index was 1.086 (95% CI: 1.038–1.135) and IRR for accidental hypothermia per 1°C decrease in wind-chill index was 1.078 (95% CI: 1.020–1.138). IRR for each of cold-related local injuries and accidental hypothermia are shown in Table 4.
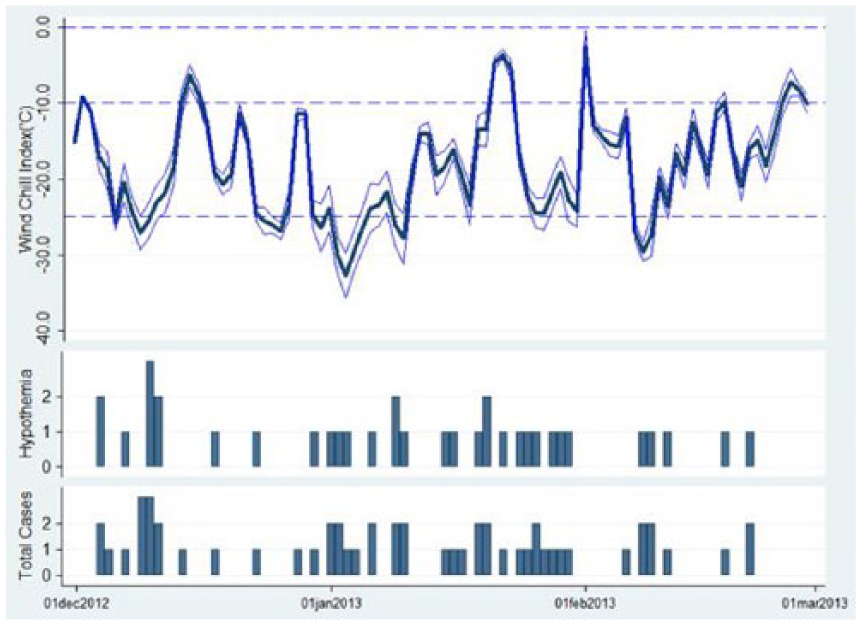
Wind-chill index and the number of reported cases during the study period.
Incidence rate ratio of cold-related illness per 1°C decrease in wind-chill index (Poisson regression analysis).
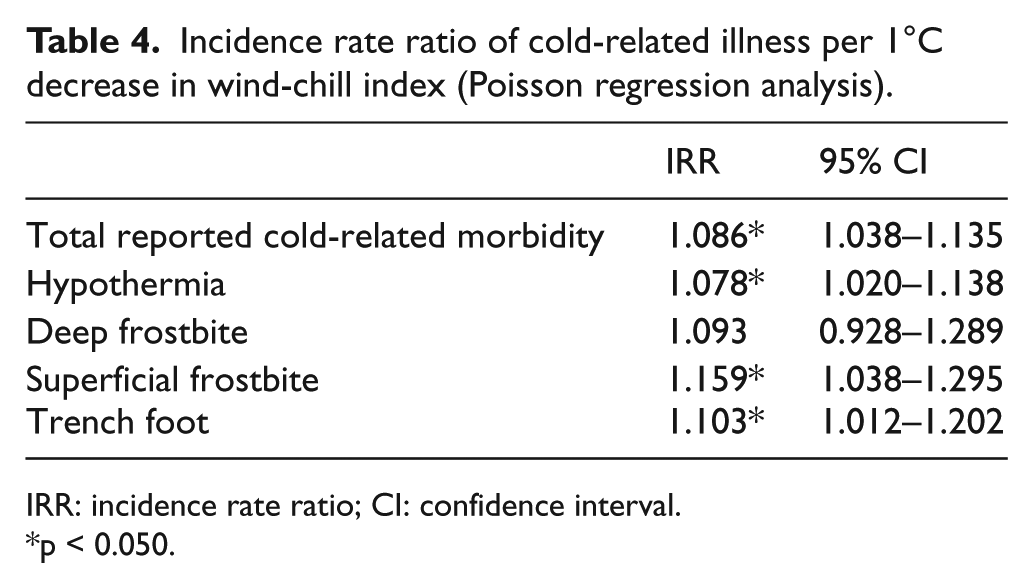
IRR: incidence rate ratio; CI: confidence interval.
p < 0.050.
Discussion
To our knowledge, this is the first report from a prospective ED-based surveillance system targeting patients with cold-related local injuries and accidental hypothermia in South Korea. ED-based syndromic surveillance system have been proposed and built in many communities to monitor and detect public health alert in response to environmental and man-made chemical and biological threats.6,16–21
Results of our surveillance showed accidental hypothermia and cold-related local injuries were associated with wind-chill index. Major adverse outcome could be expected in hypothermic patients with unstable initial vital signs and without proper out protective outwear at exposure of cold. In a retrospective review of cases with fatal hypothermia, 11 inappropriate clothing with lack of protection against wetting and insufficient insulation and resistance to wind penetration was shown as a frequent findings of fatal hypothermia. In our study, insufficient protective outwear such as absence of coat was proven to show a significant risk association with major adverse outcome. Focusing on clothing issue might be an efficient strategy in preventing hypothermia in extreme cold weather.
Homelessness and alcohol consumption are known risk factors in other studies.7–10 Although 28.6% and 50.0% of patients with accidental hypothermia and deep frostbite were homeless in our results, homeless was not associated with major adverse outcome in subgroup analysis. Also in our result, proportion of patients with alcohol consumption at cold exposure was lower in major adverse outcome group (Table 3) unlike previous reports. We think reason for the difference in results in our study is first due to different characteristics of our community from communities where previous reports were originated. Second, our surveillance included only patients who succeeded to present to ED by ambulance or walk, therefore death on arrival and other fatal cases with obvious sign of death from severe complication accidental hypothermia with alcohol intoxication might not have been included in our surveillance but included in previous autopsy reviews of fatal cases.
Positive relationship between meteorological factors such as wind-chill index and incidence of cold-related morbidities had been studies in previous studies.13–15,22 However the degree of correlation had not been well studied. In our study, lower wind-chill index was associated with increased risk of total incidence of cold-related morbidities. And, 8.6% increase in incidence could be expected as 1° of wind-chill index decreases. It might be useful for stakeholders to estimating cold-related morbidities in local society using meteorological factors in terms of emergency preparedness and response to extreme weather.
Learning the characteristics of victims of cold-related local injuries and hypothermia is important in terms of building proper prevention and treatment strategies. Since climate factors and socio-economical factors are different according to communities, each community needs to evaluate the characteristics based on their own population. In designing our surveillance system, we decided to collect patients’ data from network of EDs considering that target population vulnerable to accidental hypothermia and cold-related local injuries might have low social-economic status and poor accessibility to medical care and therefore EDs would be the main entrance of medical care for this kind of population. Many syndromic surveillance systems have been designed based on ED because of this reason.
Limitations
Our study had a few limitations. First, admission criteria and treatment protocols for cold-related morbidities varied among EDs in the surveillance system. Since the level of EDs in surveillance system varied, the facilities and human resources also varied between hospitals. Therefore, decision of admitting patients with similar severity might be different between EDs. EDs had various spectrum of active or passive rewarming device. Some EDs were only capable of passive warming by warm blankets. However, some EDs were facilitated with cutting-edge active warming device. Further study is needed to evaluate outcomes of cold-related morbidities with controlled protocol of treatment of cold-related morbidities. Second, in our surveillance system, only patients properly registered to each hospital with full name and valid social security number could be enrolled. Therefore, our surveillance system could not include patients who absconded before registering process or frequent fliers who refused to register or whose registration were refused by hospital registration for variable reasons. If these candidates were also included in the surveillance system, more detailed analysis would have been obtained.
Conclusion
Patients with cold-related morbidities were successfully monitored with ED-based surveillance system in high risk area. Absence of coat at cold exposure was associated with major adverse outcomes in patient with accidental hypothermia. Lower wind-chill index was associated with higher incidence of cold-related comorbidities.
Footnotes
Acknowledgements
The authors thank and acknowledge the contributions of the Research Program funded by the Korea Centers for Disease Control and Prevention. T.H.K. and S.C.L. wrote manuscript and full access to all of the data and take responsibility for the integrity of the data and the accuracy of the data analysis. S.C.L., K.J.S., and K.J.H. helped conceptualization and design of study. T.H.K., S.C.L., S.W.S., J.S.S., and Y.J.L. collected and analyzed data. Final draft of manuscript was reviewed and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was financially supported by the Korea Centers for Disease Control and Prevention (CDC) (2012–2013). This work was supported by the Dongguk University Research Fund of 2017. This work was supported by the Dongguk University Research Fund of 2017.
Availability of data and materials
Informed consent
Our study was not a clinical study that involves clinical intervention. We only retrospectively reviewed with data collected in the surveillance system.
Ethical approval
This study was approved by the institutional review boards of the Dongguk University llsan Hospital (IRB number: 2017–29).
Human rights
Our study was not a clinical study that involves clinical intervention. We only retrospectively reviewed with data collected in the surveillance system.