
Abstract
Introduction:
Traumatic rupture of posterior tibialis tendon in association with medial malleolus fracture is extremely rare.
Case Presentation:
We demonstrate our experience in the management of a complete posterior tibialis tendon (PTT) rupture and anterior talofibular ligament avulsion fracture from the talus in association with medial malleolus fracture in a 30-year-old male motorcyclist without any open wounds.
Discussion:
We believe this to be the first reported injury of this type in the literature. Closed ankle fractures may obscure surrounding tendon rupture and the clinician may be tempted to focus on the osseous injuries rather than the significance of associated soft tissue injures.
Conclusion:
This particular case demonstrates the importance of assessing for PTT injury in situations where high velocity impact to the ankle results in malleolar fracture.
Introduction
Ankle fractures are the most common trauma-related injuries of the foot and ankle. 1 Associated soft-tissue injuries with osseous fractures are common in ankle injuries. Due to severe pain after fracture, careful clinical examination is not possible even if the surgeon is concerned about the possibility of these concomitant injuries. While there is support for functional rehabilitation of soft-tissue injuries to the ankle, 2 high-grade injuries to the ankle that are not diagnosed and treated with appropriate surgical or rehabilitative principles can lead to poor outcomes and permanent disabilities.
Soft-tissue injuries most commonly involve the ligamentous structures about the ankle. Among all ligaments in the foot and ankle, injury to the lateral ligament complex and in particular the anterior talofibular ligament (ATFL) is the most common. Most frequently, it is an isolated injury; however, Broström in 1964 found that in approximately 20% of the patients, a combination of calcaneofibular and talofibular ligaments injury is also present. In addition, the posterior talofibular ligament is usually not injured unless there is a frank subluxation or dislocation of the ankle.3,4 ATFL injury may be associated with bone avulsion. Avulsion is more common at the fibular site than the talar end of the ligament. 5 Diagnosis of avulsion fracture of ATFL at the talar attachment is very difficult on routine ankle radiographs. 6
Complete posterior tibialis tendon (PTT) rupture is rarely reported in association with ankle fracture, however represents a potentially devastating concomitant injury. The adverse clinical effects of dysfunctional PTT on stability and the kinematics of the foot and ankle have been thoroughly explained. PTT rupture without repair can ultimately lead to severe pes planovalgus deformity followed by possible degenerative changes to surrounding joints and pain.7,8
While to the best of our knowledge, there have been a few case reports describing complete PTT rupture in association with closed ankle fracture,9–21 we could not find any reports of a triad of simultaneous closed medial malleolus fracture, ATFL avulsion from the talus, and PTT tendon rupture. So we think that it would be worthy to report this case after obtaining written informed consent for his anonymized information to be published in this article.
Case report
A healthy 30-year-old male motorcyclist presented to the emergency department with a painful and swollen right ankle after collision with a car. Physical examination demonstrated swelling and wide area of ecchymosis generally about the ankle joint with superficial skin abrasions overlying the medial malleolus. He was unable to weight bear; examination following Ottawa rules was highly suggestive of fracture. Neurovascular indices of the foot and ankle were normal. Plain radiographs revealed comminuted displaced small fragments from the tip of medial malleolus and a bone fragment in the lateral gutter of the ankle joint (Figure 1(a) and (b)). As per our institutional guidelines and resources, computed tomography (CT) was requested to define more accurately the size, number, and exact size of bone avulsed fragments to assist surgical planning. The CT scan confirmed single flake avulsion fracture at the talar attachment of ATFL in association with comminuted fracture at the tip of medial malleolus (Figure 2(a) and (b)). We did not think about possible tendon rupture; so no magnetic resonance imaging (MRI) was taken preoperatively. Surgical reduction of the fracture with removal of loose intraarticular bone fragment and soft-tissue repair was recommended based on the imaging results.
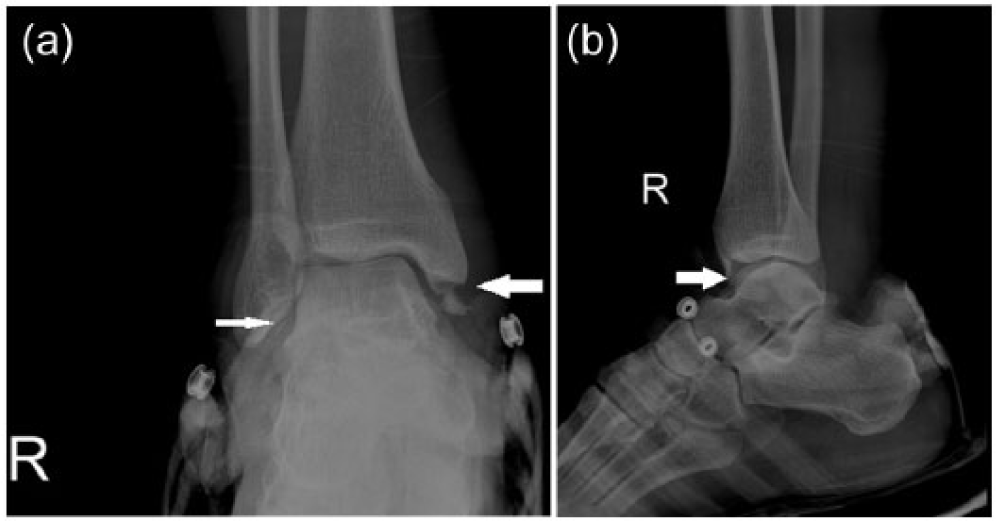
(a) Anteroposterior radiograph on arrival of the patient shows tip medial malleolus fracture and a questionable flake of bone in lateral gutter of the ankle joint and (b) lateral x-ray reveals fracture of medial malleolus, as shown by arrow.
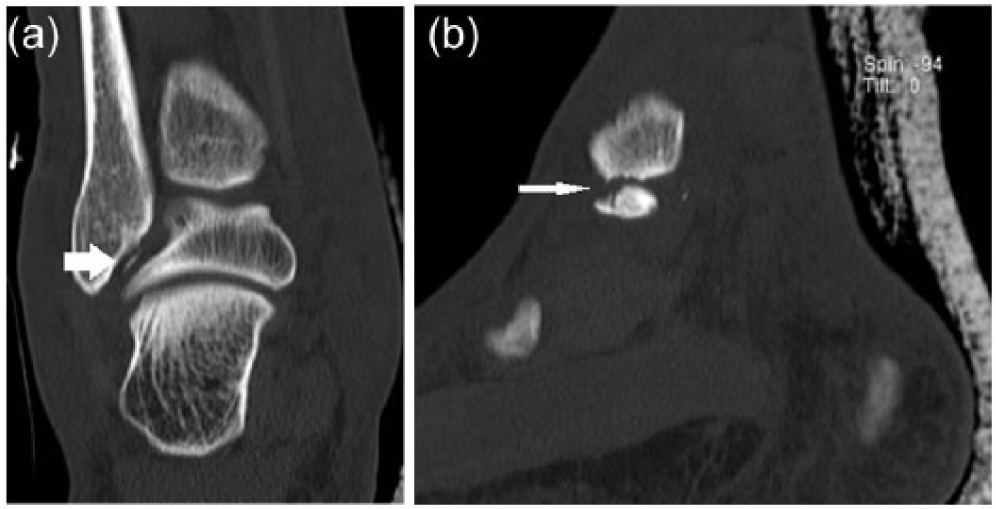
(a) Coronal CT scan cut displays an avulsed bone in lateral gutter of the ankle joint and (b) sagittal cut shows comminuted medial malleolus fracture.
In the operating room, through a direct approach to expose the medial malleolus fracture, exploration confirmed comminuted small osseocartilaginous fragments at the distal tip of the medial malleolus attached to the deltoid ligament. After removal of tiny fragments and while preparing to reattach the deltoid ligament with suture anchor, PTT was observed to be ruptured (Figure 3). PTT was repaired using modified Kessler technique with nylon 3-0 sutures. The tendon was anatomically repositioned, and the retinaculum was repaired using 2-0 Vicryl. Then, the deltoid ligament and a bone fragment were reattached to the medial malleolus utilizing a suture anchor (Aim Tec Titane 6.5 mm, Advance Ortho system). Prior to the closure on the medial side, lateral ankle joint arthrotomy was performed through an incision on lateral gutter of the ankle (Figure 4). The small flake fracture and attached ATFL were secured to the talus by a suture anchor (Aim Tec Mini Titane 3 mm, Advance Ortho system) anatomically. The ankle was tested functionally and radiologically which confirmed adequate reduction and stability.
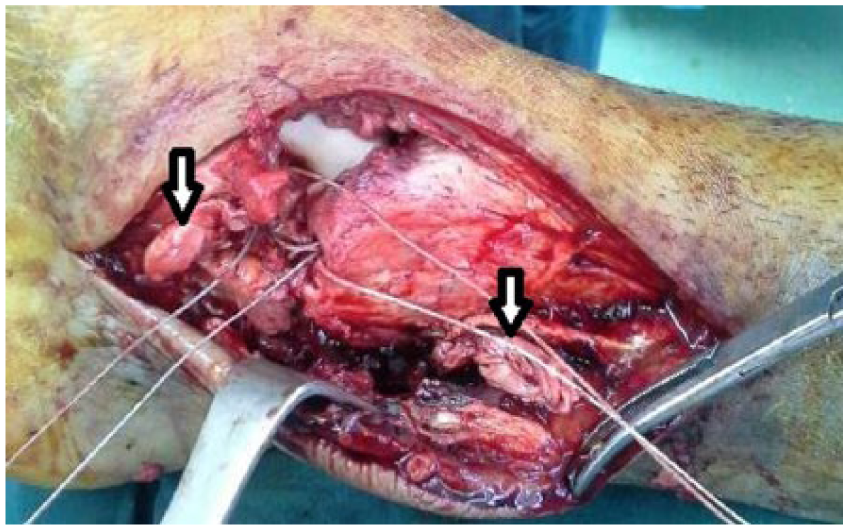
Ruptured PTT ends (arrows) during fixation of tip medial malleolus with suture anchor.

Site of avulsion of ATFL from talus (black arrow) and avulsed fragment (white arrow).
As per our institutional protocol, postoperatively a non-weight bearing short leg cast was applied for 6 weeks. This was converted to a short leg non-weight bearing slab in order to open kinetic chain range of motion exercises at the ankle. After 4 weeks in the back slab, closed kinetic chain strengthening exercises were begun. At 12 months postoperatively, full return to function was noted—pain free and with normal foot posture (Figure 5).
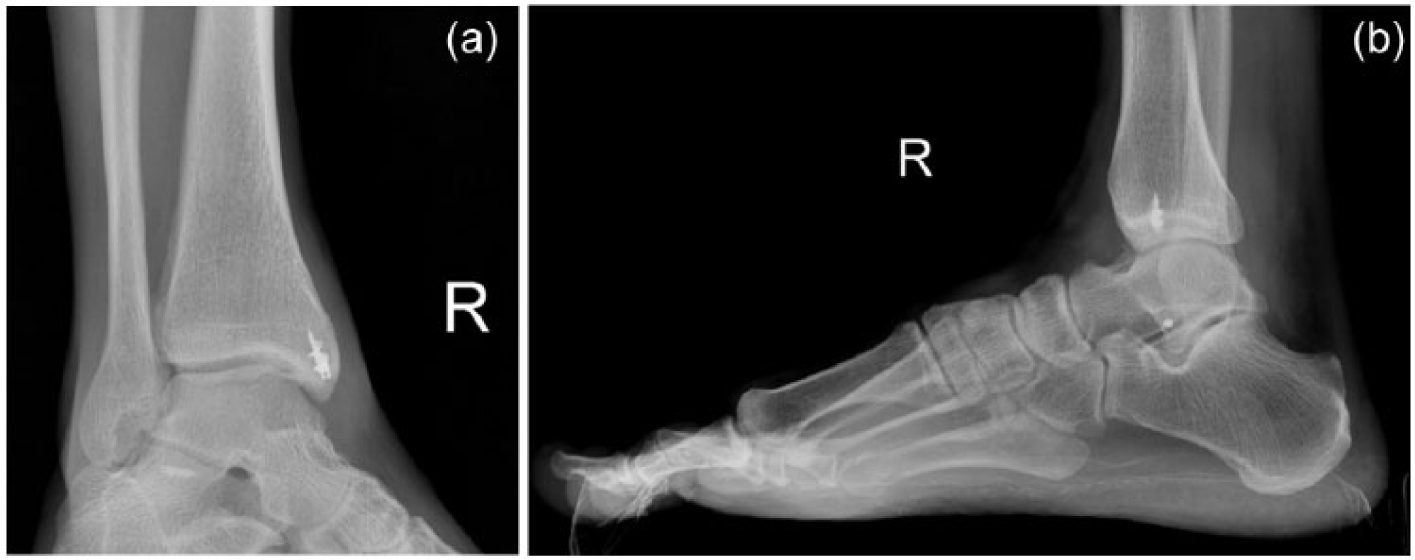
(a) Mortise and (b) lateral standing radiographs of the patient at 12 months following surgery.
Discussion
Rupture of PTT presents in different ways. Degeneration and dysfunction of PTT is common especially in obese middle-aged women and patients with risk factors of systemic inflammatory diseases, hypertension, diabetes, oral intake or injection of corticosteroids, and chronic overuse. Moreover, passing of PTT below the medial malleolus with acute angulation and hypovascularity of the tendon could result in subacute ruptures. 22
Acute traumatic rupture of PTT is very rare but has been reported in association with closed ankle fracture,9–21 open ankle fracture,23,24 distal tibial fracture, 25 and even without any fracture. 26 Primary repair of the tendon was advocated by these authors. The combination of acute traumatic rupture of PTT and isolated closed medial malleolus fracture has been reported in a few articles.9,11–13,15 This combination is usually seen after a high-energy direct trauma as the underlying mechanism. 9 However, combination of acute closed traumatic rupture of PTT and bimalleolar fractures have been explained by others after a pronation external rotation mechanism of injury.10,14,15,19 The presented case is unique because of the associated ATFL avulsion fracture from talus. The supposed mechanism of injury in this case was of a sudden anterior tibiotalar joint subluxation with spontaneous reduction after a high-energy blunt direct trauma. The line of force, predisposed to the injuries we encountered, was promulgating from a posteromedial direction and exiting anterior laterally.
Undiagnosed PTT rupture could result in dysfunction and disability with foot and ankle pain. In any traumatic episode affecting the ankle, the chance of possible PTT rupture should be considered. Associated PTT ruptures may become apparent only at surgery for the medial malleolus fracture since severe pain hinders careful clinical examination. This case report has highlighted to us that consideration to use of imaging techniques such as MRI and ultrasonography prior to initiation of therapy would be useful. Depending on circumstance however such imaging techniques are not always available, or practical. Irrespective of the advisability and availability of such imaging, evidence from modalities such as CT and plain x-ray suggested surgical reduction is warranted careful examination, and exploration during surgery should always be undertaken so as not to miss simultaneous PTT rupture. In the presented case, PTT rupture was not diagnosed before surgery but was fortunately recognized at the time of open reduction.
In conclusion, we recommend that medial malleolus fracture, especially when it is in association with other extraordinary injuries to the ankle joint and particularly with high-impact posterior medial injury, could raise a suspicion of occult PTT rupture. Meticulous exploration during surgery could prevent indistinct PTT ruptures.
Footnotes
Acknowledgements
A.R.V. and M.A.E. designed the report; K.M. collected the patient’s clinical data; A.R.V., H.R., and K.M. participated in drafting the article; and M.G. critically reviewed the manuscript. All authors approved the final manuscript as submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was undertaken in the Bone and Joint Diseases Research Center, Department of Orthopedic Surgery, Chamran Hospital, Shiraz University of Medical Sciences, Shiraz (71948-15644).
Availability of data and materials
The files of the case with more pictures, as deleted by editor, are available.
Informed consent
Informed consent obtained.
Ethical approval
Ethical approval was needed because it is a case report with taking signed written informed consent.
Human rights
The patient knows about reporting his injury in a foreign medical journal.