
Abstract
Traumatic rupture of the posterior tibialis tendon is an extremely infrequent condition, which mostly occurred due to a traumatic mechanism of pronation and external rotation, less commonly in direct trauma on the medial side of the ankle. This lesion is overlooked preoperatively most of the time because of the limitation of physical examination owing to acute pain and swelling secondary to a medial malleolar fracture. Early diagnosis and treatment of this injury are very important to prevent the complications like acquired flatfoot deformity. Few cases have been described in the literature for the posterior tibialis tendon rupture associated with a closed ankle fracture. Here we report an acute rupture of the posterior tibialis tendon associated with a closed medial malleolar fracture after a high-energy trauma in a healthy 33-year-old man. We fixed the medial malleolar fracture with two screws and repaired the tendon with a direct end-to-end suture. We hope that our study can be helpful for other colleagues to consider this lesion in similar circumstances.
Introduction
Posterior tibialis tendon (PTT) rupture with an ankle fracture is an infrequent condition, which is reported in only a few cases.1,2 High-energy direct trauma is the fundamental mechanism in medial malleolus isolated fractures.2,3 The main mechanism of traumatic rupture of the PTT is pronation with external rotation of the ankle, in which the medial compartment of the ankle is involved.1,3 Conditions such as direct trauma 3 and forced dorsiflexion with inversion can also cause traumatic damage to this tendon rarely. 2
Due to the acute pain and edema caused by an ankle fracture, the possibility of clinical examinations is very limited, so, in most cases, the rupture of the PTT is misdiagnosed before surgery. 4 Park 4 has reported one case in which a partial rupture of posterior tibialis tendon was misdiagnosed for about 5 months. In his case, the patient had experienced an isolated transverse fracture of the medial malleolus with minimal displacement after a car accident. Park 4 observed that 5 months after the surgery, the patient was referred with complaints of mild swelling and obscure pain around the posterior aspect of the medial malleolus. This time they diagnosed the partial rupture of the PTT with the help of magnetic resonance imaging (MRI).
This lesion is usually diagnosed intraoperatively. 3 Unconsciousness about diagnosis and early treatment of PTT rupture can cause several complications for the patient such as long-term disability and planovalgus deformity.4,5 The PTT is responsible for supporting the medial longitudinal arch of the foot, so, the lack of support of the medial longitudinal arch is also a complication of not treating the rupture of this tendon. 2
Early surgical repair is necessary to prevent complications of PTT rupture and recover tendon function.6–8 Here we report a case of PTT rupture, which occurred after a car accident in a young male.
Case presentation
A 33-year-old man was admitted to the emergency department after a high-speed car accident with a painful and swollen right ankle. The patient was the driver himself and was not able to remember the exact mechanism of the injury. He did not report any significant disease and previous surgery.
On physical examination, the right ankle revealed notably swollen with echymosis and pain especially in the area of the medial malleolus. His active and passive movements were very limited and painful. There was no skin lesion at the injury area and neurologic deficit. Both posterior tibialis artery and dorsalis pedis artery were palpable.
An oblique fracture of the medial malleolus with minimal displacement was noted on the anteroposterior and internal oblique radiographs of the ankle (Figure 1).

An oblique fracture of the medial malleolus.
The patient was hospitalized with a diagnosis of close medial malleolar fracture and was a candidate for internal fixation surgery.
Three days after the accident, edema decreased and surgery was performed. Patient was positioned supine under spinal anesthesia. An anteromedial incision of distal tibia with protection of saphenous vein was performed, and an oblique fracture of the medial malleolus was observed. Incidentally, complete rupture of the PTT, 2 cm proximal to the apex of the medial malleolus, was detected intraoperatively (Figure 2). The tendon was not interposed into the fracture. The rupture end was flimsy and did not appear to be cut through the sharp edge of the bone.
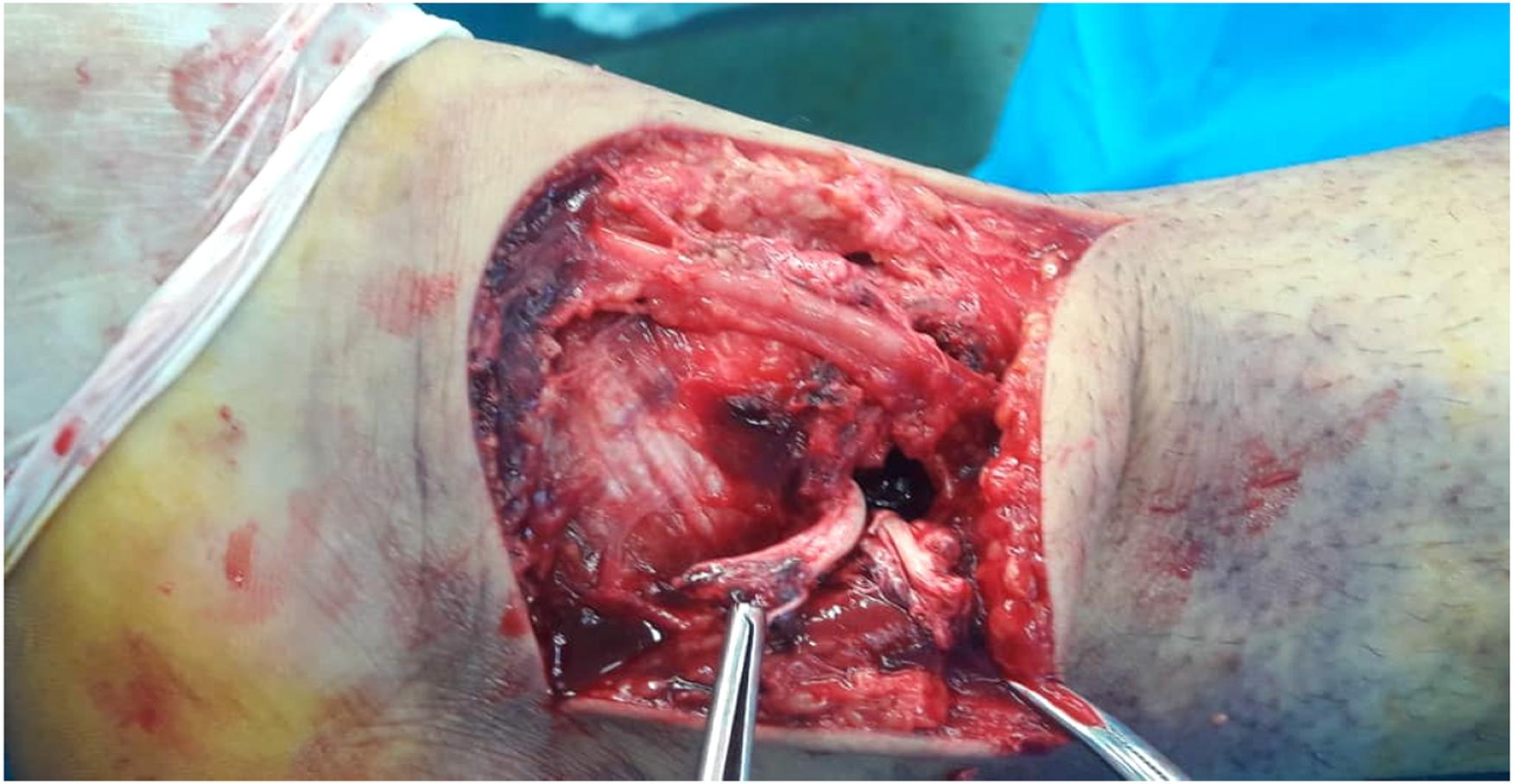
Intraoperative view of the ruptured posterior tibialis tendon.
We first fixed the medial malleolus with two screws (Figure 3). As there were no obvious signs of a degenerative tendinopathy, or calcification, a direct end-to-end modified Kessler tendon repair with non-absorbable monofilament sutures was performed.

Internal fixation with two screws.
The patient was discharged two days after the surgery, with instructions to be non-weight-bearing and fitted with a splint. Anticoagulant and oral antibiotic were also prescribed.
After 2 weeks, stitches were removed. After 3 weeks, the splint was removed and a removable brace was utilized for the patient. From the fourth week after surgery, partial weight bearing was allowed combined with gentle passive motion. Radiographs were obtained at 6 and 12 weeks postoperatively (Figure 4). Three months after the operation, the fracture was completely healed, the patient was asymptomatic and had a normal ankle range of motion, the function and strength of the tibialis posterior tendon were normal. The appearance and posture of the foot were normal and there was no deformity like a flat foot.

Twelve weeks postoperatively radiography.
Discussion
The largest and anterior most tendon on the medial aspect of the ankle is the PTT, which arises from the posterior interosseous membrane, and the surface of the proximal tibia and fibula.9,10 This tendon descends between the flexor digitorum longus and the flexor hallucis longus, in the deep posterior compartment of the leg. 9 It continues downward on superficial deltoid ligament and then deep to the plantar calcaneonavicular ligament in the hindfoot. 2 The PTT ended with an almost 90° shift in the direction around the medial malleolus, at the level of the ankle. 9 The plantar insertion of the PTT is so complicated: there are multiple insertions on navicular tuberosity on one side; on the other side, except the talus, the main tendon has insertions on all of the tarsal bones. Finally, it has insertions with fan-shaped fascicles on the second, third, and fourth metatarsals bones. 2
The PTT has a role in plantarflexion of the ankle and supination of the foot. 1 This tendon, along with the calcaneonovicular ligament, produces a powerful support for the medial arch of the foot. 9
Spontaneous rupture of a healthy tendon is rare, whereas it may occur in the context of chronic tendinopathy, rheumatoid arthritis and non-specific tenosynovitis.2,11,12 The most common pathology that affects the PTT is chronic tendinopathy 13 and the progressive “chewing gum” lesion in a setting of chronic tendinopathy,1,9 which occurs mostly in overweight women above 50 years of age who have valgus flat foot. 14
Comorbidities such as aging, diabetes, corticosteroid therapy, obesity, rheumatoid arthritis, connective tissue disease and hypertension can be risk factors for rupture and long-term insufficiency.15–17.
Acute rupture of the PTT is less common than chronic and most happened in athletes who have had repeated sprains. 9 Pronation and external rotation of the ankle, with direct blunt trauma to the medial area of the ankle, are most common mechanisms of the acute rupture of this tendon. 18
The main artery that supplies the PTT is posterior tibial artery. Based on the work of Petersen et al. 19 blood vessels enter the posterior tibial tendon paratenon through the mesotenon and vessels formed by a “web-like” network. Then they penetrate the tendon tissue and form an anastomosis with the intratendinous arterial network. In the region where the tendon changed direction to the back and distal of the medial malleolus (retro malleolar region) intratendinous vascular network was interrupted and the tendon was placed in an avascular zone. It is the most frequent area of ruptures especially the distal portion. 11 Also this region is the primary zone that encounters with degeneration of chronic tendinopathy. 14 The most common site of rupture is 2 cm above the fracture. 20 Anyway, the rupture can occur anywhere along the tendon. 2 The rupture site of our case was also 2 cm above the fracture.
Traumatic mechanisms of pronation and external rotation, redundant edema on the medial side of the ankle, the irreducibility of the dislocation or fracture, and the appearance of “bone flakes” separated from the distal medial metaphysis of the tibia are suspicious clinical signs that should be considered for PTT lesions.1,2,9,11,18,21,22
Due to the limitations of clinical examinations, the use of MRI and preoperative ultrasound can be helpful in diagnosing this lesion. 23 Because these techniques are not always available, careful examination of the tendon rupture should be performed during surgery. 23
Misdiagnosed complete or partial rupture of the PTT has many painful consequences, such as lack of supporting medial longitudinal arch of foot and planovalgus deformity. 1 Acquired flatfoot deformity secondary to untreated PTT rupture was described by Mueller 24 and Kupcha and shah. 25
Direct suture or tenodesis on the flexor digitorum longus tendon are the treatment of choice. 18
In the literature, we found only limited articles that reported complete posterior tibialis rupture associated with a closed ankle fracture.1–3,5,7,8,11,12,16,18,20–23,26–35 Giblin et al. 31 first described the PTT rupture associated with a closed medial malleolar fracture in 1980. Most of the articles reported complete rupture of the PTT with medial malleolus involvement. Monto et al. 33 reported a complete rupture of PTT without medial malleolar fracture. Most papers report a trauma in pronation, and external rotation of the ankle, overcoming the strength of the tibialis posterior tendon fibers. All studies that have been published so far have reported acceptable results in an average 6-month examination and in the long-term return of patients to previous activity after primary repair. Based on the work of Formica et al. 2 some studies have reported successful results with tenodesis on flexor digitorum longus tendon.
In our case, the patient had no history of previous surgery, comorbidities, or corticosteroid therapy, thus, the only possible mechanism that we could consider was pronation and external rotation with direct trauma by pedal. Diagnosis of the PTT rupture was intraoperative. The rupture was 2 cm above the fracture and we did not find any interposition of the PTT into the fracture. An end-to-end tendon repair was performed. He had a good outcome at the 3-month follow-up examination.
We have briefly described some of the previous reports in Table 1. In conclusion, PTT rupture associated with an ankle fracture is a rare condition, which is not routinely explored in ankle fracture surgery. Unfortunately, this lesion is often misdiagnosed and has painful consequences as flatfoot deformity that involves pain and disability for the patient. We recommend that in cases of ankle fractures that occur following a direct high-energy trauma or traumatic mechanism of pronation and external rotation that are accompanied by excessive displacement, swelling of the medial region of the foot, we consider the PTT rupture. In such cases, it is better to explore this tendon during surgery so that if the tendon is damaged, we can repair it at the appropriate time and prevent severe and painful consequences. Intraoperatively, we should examine the tendon carefully and pay attention to its tension. Loss of tension can refer to the PTT rupture.
Summary of published observations.
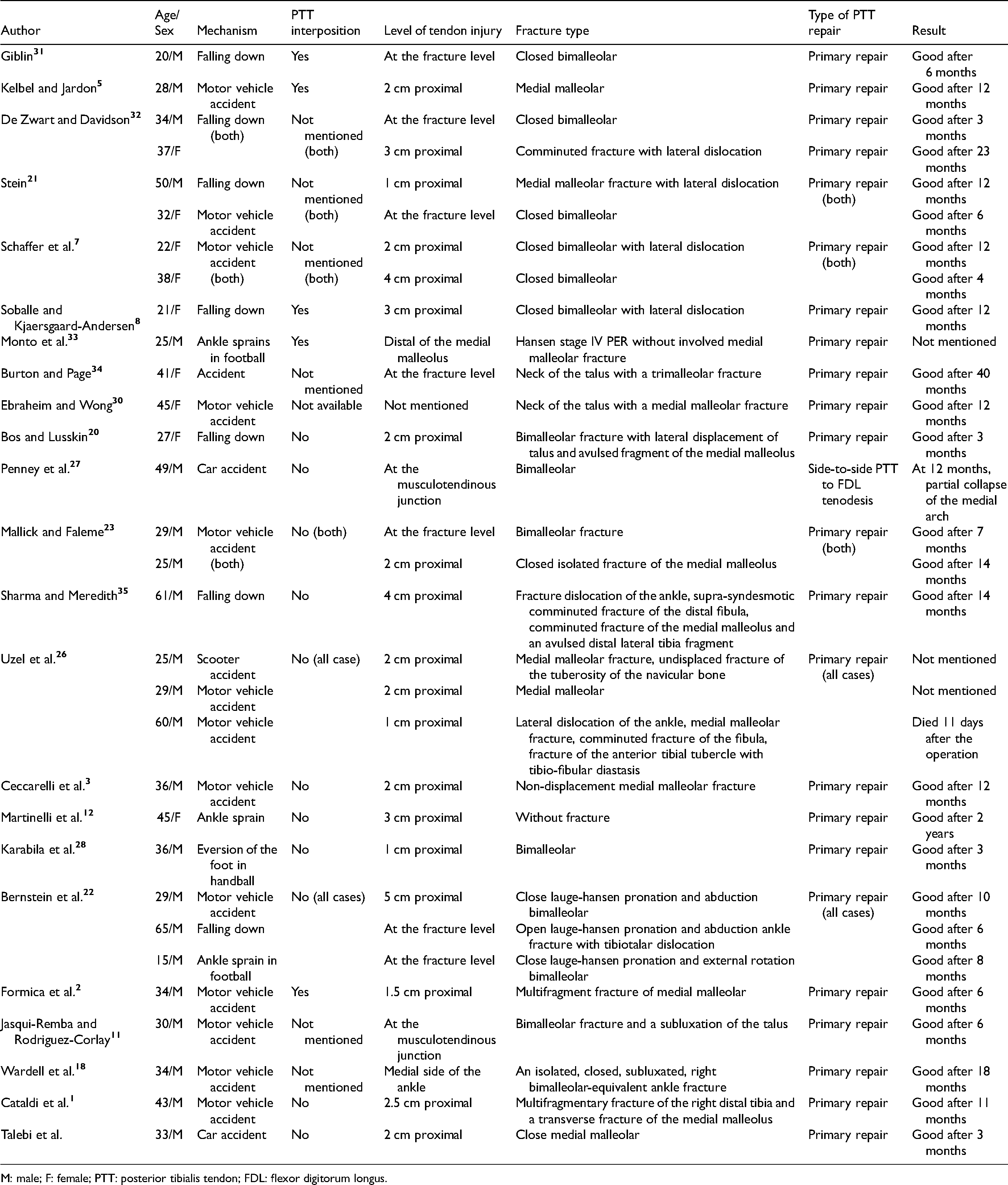
M: male; F: female; PTT: posterior tibialis tendon; FDL: flexor digitorum longus.
We hope that our report, be a helpful guide for physicians who face these conditions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.