
Abstract
Here, we report a case of successful treatment for a patient with abdominal compartment syndrome who was on venoarterial extracorporeal life support. A 33-year-old man visited the emergency room with cardiac arrest. Extracorporeal cardiopulmonary resuscitation was performed, and massive volume infusion was needed to maintain adequate perfusion pressure. After 6 h, his abdomen was distended, and venous drain was decreased. His bladder pressure was more than 25 mm Hg. Abdominal compartment syndrome was suspected, and prompt decompressive laparotomy was performed to restore venous drain, resulting in stabilization hemodynamically. The patient made a full recovery. He was discharged after implantation of internal cardiac defibrillator.
Introduction
Extracorporeal life support improves the survival and outcome of refractory cardiogenic shock including cardiac arrest. Various complications of extracorporeal life support have been reported in previous studies. Abdominal compartment syndrome during extracorporeal life support has been previously described in pediatric population. However, it is very rare in adult patients. Risk factors for the development of intra-abdominal hypertension and abdominal compartment syndrome are large volume resuscitation, massive transfusion, management with an open body cavity, core hypothermia, coagulopathy, severe sepsis or septic shock, cirrhosis or other liver failure with ascites and mechanical ventilation. 1 Massive fluid resuscitation for patient on extracorporeal life support might lead to ascites and interstitial oedema that can compromise venous flow of extracorporeal circuit and perfusion of intra-abdominal organs. 2 Here, we report the first survival case of abdominal compartment syndrome in an adult patient induced by venoarterial extracorporeal life support due to cardiogenic shock.
Case Report
A 33-year-old male patient was transferred to our emergency room with cardiac arrest. He had a tiny atrial septal defect. He was followed up annually. Recent echocardiography demonstrated normal cardiac function without pulmonary hypertension or arrhythmia. At scene, ventricular fibrillation was confirmed. Cardioversion was done by paramedics. His initial rhythm on arrival at hospital was ventricular fibrillation that was refractory without being converted to normal sinus rhythm by cardioversion. Therefore, extracorporeal cardiopulmonary resuscitation was initiated. Right common femoral artery and vein were cannulated percutaneously. For venous drain, 21-French venous cannula (Bio-Medicus™ Multi-Stage Femoral Venous Cannula; Medtronic, Minneapolis, MN, USA) was used. A 17 French arterial cannula was placed in right external iliac artery by the percutaneous cannulation of right common femoral artery. Quadrox oxygenator and rotaflow pump (Maquet, Hirrlingen, Germany) were connected to extracorporeal circuit. After extracorporeal circulation, his cardiac rhythm was recovered. His systolic blood pressure was less than 70 mm Hg. Transthoracic echocardiography revealed severe left ventricular dysfunction (ejection fraction< 20%) due to stress-induced cardiomyopathy. Therapeutic hypothermia was initiated by internal cooling method with catheter. At 2h after from extracorporeal circulation, chatter of extracorporeal circuit was observed. Central venous pressure was 4cmH2O and right atrium was collapsed on transthoracic echocardiography. On chest X-ray, the tip of venous cannula was positioned at the junction of superior vena cava and right atrium. There was no evidence of haemorrhagic complication including cannulation site bleeding. Those levels of haemoglobin and haematocrit showed normal range as represented to be 13.4 g/dl and 35% respectively. Intravascular volume depletion resulted from post cardiac arrest syndrome was suspected and massive crystalloid solution (> 3000 cc) was infused to maintain adequate perfusion pressure during 50min. After infusion of large volume, blood flow by extracorporeal circulation could be kept up to 3.5 L/min. At 6 h after the start of extracorporeal circulation, his abdomen was distended. It became hard and firm. Hourly urine output was decreased to < 20 cc/h. His systolic blood pressure was dropped to 40 mm Hg without responding to infusion of colloid solution or vasopressor. Venous drain from the right atrium was decreased. The flow of extracorporeal circulation was also decreased from 4 to 1 L/min (4000 r/min). Bladder pressure measured with Foley catheter was more than 25 mm Hg. Transabdominal ultrasonography revealed no abnormal fluid collection. Abdominal compartment syndrome was presumed, and emergency decompressive laparotomy was proceeded at intensive care unit. After median laparotomy, distended stomach with small and large bowel without definite ischemia from hypoperfusion was protruded from abdominal cavity. There were only small amounts of ascites (less than 200 cc). Bowel was covered with sterile plastic bag. Meticulous haemostasis process including pinpoint electrocautery, thrombin spray or other topical haemostats was needed to perform to prevent bleeding by anticoagulation with heparin. While intravenous heparin therapy was maintained, target activated clotting time was maintained to be 160–200sec. After the procedure, flow of extracorporeal circulation was increased to 4.5 L/min (4000 r/min), and he was stabilized haemodynamically. After 3 days of the procedure, the distended bowel was normalized. In operating room, ischemic segment of small bowel was resected, and double-barreled enterostomy was performed. Previous laparotomy wound was approximated (Figure 1). His cardiac function was recovered at 5 days after extracorporeal resuscitation (left ventricular ejection fraction > 45%). Holter monitoring for 24 h revealed frequent ventricular arrhythmia. Therefore, internal cardiac defibrillator (ICD) was implanted. Extracorporeal life support could be weaned at 1 day after the implantation of ICD. Mechanical ventilator support was needed for 12 days due to aspiration pneumonia. Enterostomy was reversed, and the patient was discharged at 21 days after the secondary operation without complications such as cognitive dysfunction.
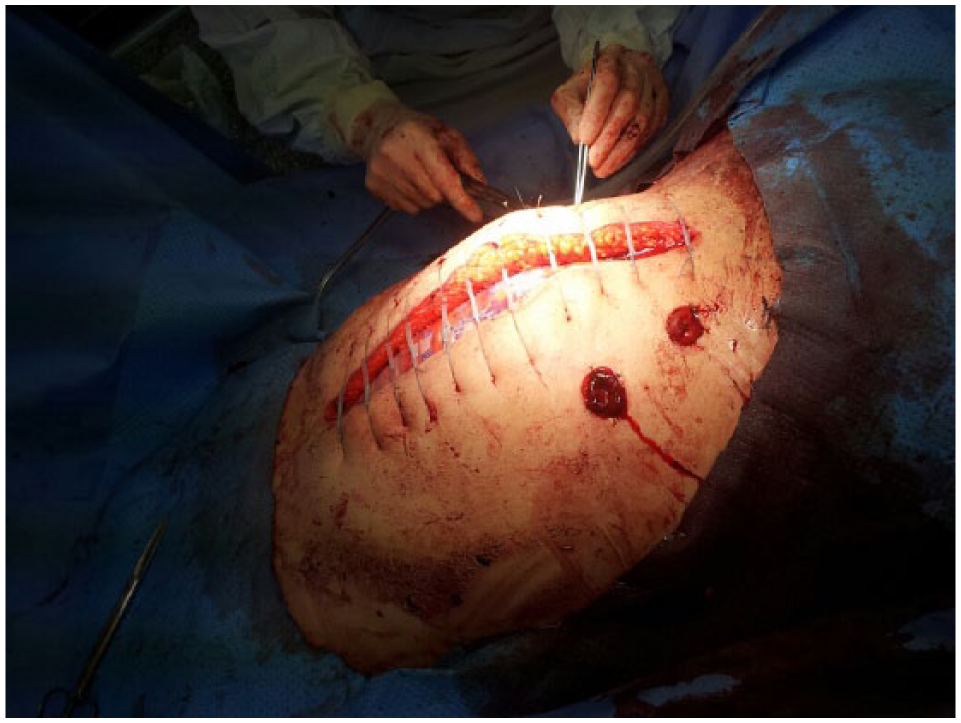
Double-barreled enterostomy and approximation of laparotomy wound at 3 days after decompressive laparotomy.
Discussion
Abdominal compartment syndrome is an important and potentially correctable cause of death in critically ill patient. The incidence of abdominal compartment syndrome is very low. However, it might not be recognized or reported. Increased intra-abdominal pressure, secondary end-organ dysfunction, and improvement with decompression are typical features of this syndrome. 3 Intra-abdominal hypertension in adult patients is defined as bladder pressure measured at more than 12 mm Hg. Abdominal compartment syndrome with bladder pressure > 20 mm Hg can cause renal, pulmonary, and cardiovascular dysfunction.4,5
Intra-abdominal hypertension and abdominal compartment syndrome can occur during extracorporeal life support. They can cause extracorporeal circulation failure, resulting in deterioration of haemodynamic status of patient. Massive fluid overload can cause ascites and contribute to abdominal compartment syndrome. 6 Elevation of intra-abdominal pressure can decrease venous return to the right atrium, thus compromising extracorporeal blood flow. It can also increase vascular resistance in the splanchnic beds, compromising end-organ perfusion. Because inadequate venous return to the extracorporeal circuit can result from volume depletion and improper position of venous cannula, these conditions must be ruled out before abdominal decompression. 7
Some medical treatments have been recommended by the World Society of Abdominal Compartment Syndrome. Maximal sedation using neuromuscular blockade and supine positioning can improve abdominal wall compliance. Intraluminal contents can be evacuated by nasogastric decompression, rectal decompression, and the use of gastrointestinal prokinetic agents. Fluid restriction and the use of diuretics, colloids, and haemodialysis can also correct the positive fluid balance. 8 If ultrasound is immediately available with a large amount of ascites demonstrated on ultrasound, catheter drainage alone may be effective. However, for most patients with abdominal compartment syndrome, intra-abdominal hypertension is often secondary to bowel distension, bowel wall oedema, and retroperitoneal oedema which could not be relieved by catheter drainage alone. 9 For unstable and anticoagulated patient with abdominal compartment syndrome on extracorporeal life support, the benefit of decompressive laparotomy remains controversial. Prompt decompressive laparotomy could restore venous drain and result in haemodynamic stabilization. However, survival after decompressive laparotomy has been very rare. The cause of death includes intra-abdominal bleeding, multiple organ failure, sepsis, and neurologic dysfunction. 2 In newborn and children population, only three survivors of abdominal compartment syndrome on extracorporeal life support have been reported. These survivors were treated with peritoneal drainage for abdominal decompression.5,10 Only three cases of adult patients on extracorporeal life support with abdominal compartment syndrome caused by massive fluid overload have been reported previously. Multiple organ failure, sepsis, and anoxic brain damage inevitably led to two deaths after urgent decompressive laparotomy. The other patient died before decompressive laparotomy.6,11
Our case of abdominal compartment syndrome was induced by venoarterial extracorporeal life support for cardiogenic shock. He needed massive fluid overload to maintain appropriate flow rate. Urgent decompressive laparotomy dramatically improved his haemodynamic status. His abdominal compartment syndrome was subsequently confirmed. Intra-abdominal contamination and sepsis could be avoided by wrapping bowel with sterile method and performing early resection of ischemic bowel. This is the first survival case among adult patients with abdominal compartment syndrome during venoarterial extracorporeal life support. Here, we report this case with the literature review.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was partially supported by Soonchunhyang University research fund.
Informed consent
Written informed consent was obtained from the patient for publication of this manuscript and any accompanying image.