
Abstract
Introduction
The probability of surviving a cardiac arrest remains low. International resuscitation guidelines state that extracorporeal cardiopulmonary resuscitation (ECPR) may have a role in selected patients suffering refractory cardiac arrest. Identifying these patients is challenging. This project systematically reviewed the evidence comparing the outcomes of ECPR over conventional-CPR (CCPR), before examining resuscitation-specific parameters to assess which patients might benefit from ECPR.
Method
Literature searches of studies comparing ECPR to CCPR and the clinical parameters of survivors of ECPR were performed. The primary outcome examined was survival at hospital discharge or 30 days. A secondary analysis examined the resuscitation parameters that may be associated with survival in patients who receive ECPR (no-flow and low-flow intervals, bystander-CPR, initial shockable cardiac rhythm, and witnessed cardiac arrest).
Results
Seventeen of 948 examined studies were included. ECPR demonstrated improved survival (OR 0.40 (0.27–0.60)) and a better neurological outcome (OR 0.10 (0.04–0.27)) over CCPR during literature review and meta-analysis. Characteristics that were associated with improved survival in patients receiving ECPR included an initial shockable rhythm and a shorter low-flow time. Shorter no-flow, the presence of bystander-CPR and witnessed arrests were not characteristics that were associated with improved survival following meta-analysis, although the quality of input data was low. All data were non-randomised, and hence the potential for bias is high.
Conclusion
ECPR is a sophisticated treatment option which may improve outcomes in a selected patient population in refractory cardiac arrest. Further comparative research is needed clarify the role of this potential resuscitative therapy.
Keywords
Introduction
In the last five years, the survival rate for out-of-hospital cardiac arrests (OHCA) in the UK has increased marginally from 7.7% to 8.3%. 1 A similar improvement can be seen for in-hospital cardiac arrest (IHCA) patients (35.4% to 39.7%). 2 Many survivors have persistent neurological impairment. These low rates of neurologically intact survival reveal a significant healthcare need to improve outcomes for these patients.
Extracorporeal membrane oxygenation (ECMO) is a method of supporting patients with potentially reversible respiratory and/or cardiac failure. A patient's blood is pumped through an artificial lung (membrane oxygenator) which both oxygenates blood and removes carbon dioxide (decarboxylation). There are two main configurations of an ECMO circuit: veno-venous (VV) and veno-arterial (VA). In VV-ECMO, blood is pumped from the venous system and returned to the venous system; thus, oxygenation and decarboxylation of blood occur in the venous system in a pre-pulmonary position, supporting patients with severe lung failure. By contrast, VA-ECMO pumps blood from the venous system, oxygenates and decarboxylates it before returning it at such a rate to the arterial system that the arterial system is pressurised and blood flows across the patient's vital organs. Hence, VA-ECMO provides both cardiac and respiratory support.
Extracorporeal cardiopulmonary resuscitation (ECPR) is the use of VA-ECMO in patients with refractory cardiac arrest to ‘buy time’ – temporarily replacing the pumping function of the heart and maintaining perfusion of vital organs, while the heart recovers or definitive therapy such as primary percutaneous coronary intervention is performed. It is typically instituted by draining blood through a cannula in the femoral vein and returning it to the femoral artery.
Previous studies have indicated that a predictor of a good outcome in ECPR patients is a shorter duration of ‘low-flow’,3–6 the period in which the patient is in cardiac arrest but CCPR is being performed. A physiological explanation for this is that chest compressions in CCPR only produce 25–30% of a normal cardiac output. 7 The longer this ‘low-flow’ state is present, the less the chance of adequate coronary perfusion pressure and return of spontaneous circulation, but also the greater the chance of irreversible multi-organ failure including hypoxic brain injury. A recent systemic review and meta-analysis of out-of-hospital cardiac arrest patients treated with ECPR confirmed better outcomes associated with low-flow time and also the presence of a shockable rhythm. 8 Aside from this, there is paucity in the data regarding which patients might benefit from receiving ECPR in comparison to CCPR resuscitation techniques.
There are no published randomised trials comparing ECPR to CCPR, but there are growing numbers of cohort studies. This paper aims to review the evidence of any superiority of ECPR over CCPR in adult patients of cardiac-origin cardiac arrest looking at survival and neurological outcome, and secondarily to assess which parameters predict survival in patients undergoing ECPR.
Methods
This project was derived from work undertaken as part of the Intercalated Bachelor of Science degree in Pre-hospital medicine (which is a collaboration between The Institute of Pre-Hospital Care at London's Air Ambulance, and Barts and The London School of Medicine at Queen Mary University of London). It was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.
9
To coordinate the search strategy, two research questions were devised, one of them fitting a PICOST format:
‘In adult patients of cardiac-origin cardiac arrest (P), does extracorporeal-CPR (I), compared to conventional-CPR (C), improve survival and neurological outcome (O) as illustrated by cohort studies (S) published in the years 2011–2017 (T)?’ ‘In adult patients of cardiac-origin cardiac arrest who have undergone extracorporeal-CPR (P), which parameters lead to increased survival as illustrated by cohort studies (S) published in the years 2011–2017 (T)?’
Search strategy
A systematic literature search was undertaken on 2 January 2017 followed by a supplementary search on 20 August 2018. The search included EMBASE, Medline and PubMed databases from 1 January 2011 onwards. Medical Subject Headings were combined with non-indexed relevant search terms to create a comprehensive search strategy. Although numerous synonyms were used, the basic premise of the search was ‘Cardiac arrest’ AND ‘Extracorporeal CardioPulmonary Resuscitation’ (see Supplementary Data for full search criteria). Search filters were added to refine the publication date range and participants (human and ≥17 years old). Secondly, a systematic search of the grey literature was conducted in line with the Luxembourg Definition of grey literature. 10 Similar search criteria were used for Web of Science along with a search of the conference proceedings of the Society of Critical Care Medicine, European Society of Intensive Care Medicine, European Extracorporeal Life Support Organisation, and Social Media and Critical Care for the same period. Finally, the references of included papers were screened for additional material not found in the initial literature search.
Study identification
Inclusion and exclusion criteria.
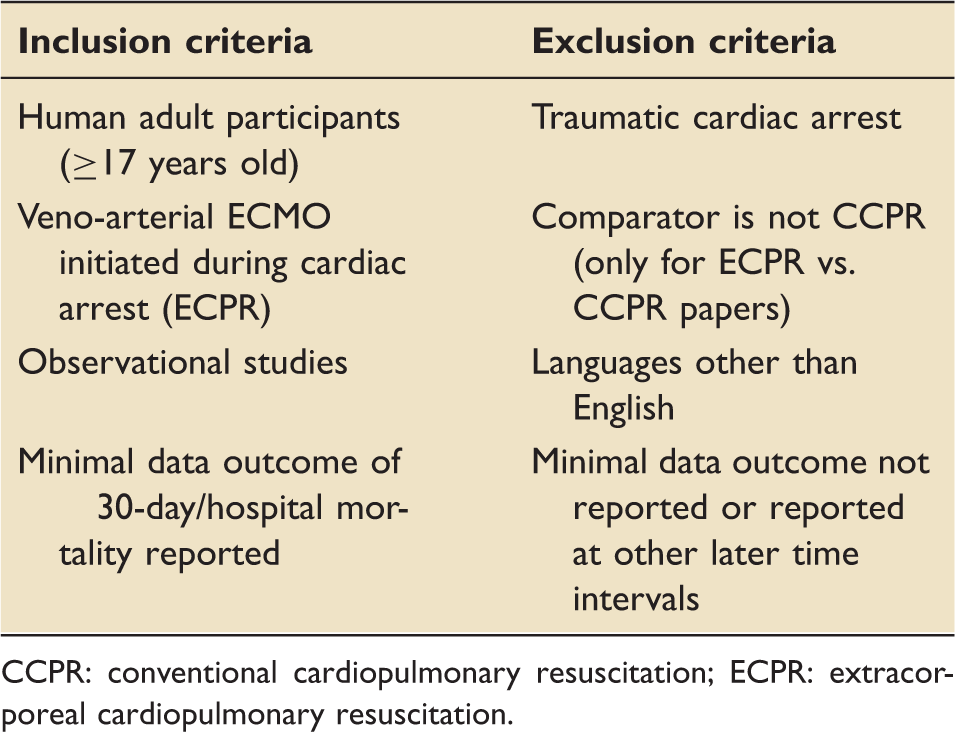
CCPR: conventional cardiopulmonary resuscitation; ECPR: extracorporeal cardiopulmonary resuscitation.
Data extraction
Data extraction focused on identifying population demographics (country, enrolment period, participant numbers, sex and age), clinical parameters throughout the resuscitation period (witnessed arrest, no-flow duration, bystander-CPR, initial shockable cardiac rhythm and arrest-to-ECPR interval) and final outcomes (survival and neurologically intact survival). If propensity score matching had been undertaken, then matched data were extracted rather than the whole data set. Extracted data were placed into a data extraction spreadsheet (Excel 15.3.2, Microsoft Corporation) independently (CT).
During data extraction, papers were divided into two groups: papers that compared ECPR with CCPR and papers that looked at the clinical parameters of survivors versus non-survivors in patients undergoing ECPR.
The arrest-to-ECPR interval was examined in this study rather than the setting of ECPR, as this former value was deemed to be more appropriate for the outcomes of the study.
Low-flow duration was assumed to be comparable to the arrest-to-ECPR interval when this former variable was not reported.
Risk of bias
The Risk of Bias Assessment Tool for Non-randomised Studies of Interventions (ROBINS-I) was used to assess risk of bias in the included studies. 11 The assessment for bias was performed across seven domains: confounding variables, participant selection, classification of interventions, deviation from intervention, incomplete outcome data, blinding of outcome assessment and selective reporting.
An attempt at assessing publication bias was made using funnel plot techniques, Begg's rank test and Egger's regression test, as appropriate given the known limitations of these methods.
Meta-analysis
Study details were entered into Review Manager (v5.3, The Cochrane Collaboration) to facilitate the production of forest plot analyses. Odds ratios (OR) or mean differences (MDs) were reported for dichotomous and continuous variables, respectively. Random effects models were used in meta-analysis, and I2 was reported to assess consistency. Where data were not reported as mean ± standard deviation, these were estimated using the median and IQR/range using formulae 3, 14, 6 and 16 from Wan et al. 12 .
The results were deemed statistically significant when p values of 0.05 or less were reported.
Outcome measures
The primary outcome was defined as survival at hospital discharge or 30 days. The secondary outcome of neurological function in survivors was dichotomised into favourable or unfavourable based on either the cerebral performance category (CPC) scale (1–2 was defined as favourable) or Glasgow outcome scale (5–4 was defined as favourable). The definitions used in this paper are consistent with those of the Utstein Cardiac Arrest and Cardiopulmonary Resuscitation Outcome definitions. 13
Results
Study selection
The search strategy detailed above was performed which initially identified 1935 papers. After the removal of duplicate papers and abstract screening, 181 remained. Following full-text screen, 36 papers remained; the full breakdown for these can be seen in Figure 1. Following this, data extraction was undertaken on these papers. A further 19 articles were excluded due to having insufficient outcome data. Hence, 17 articles were deemed eligible for the systematic literature review.
Flowchart of study identification.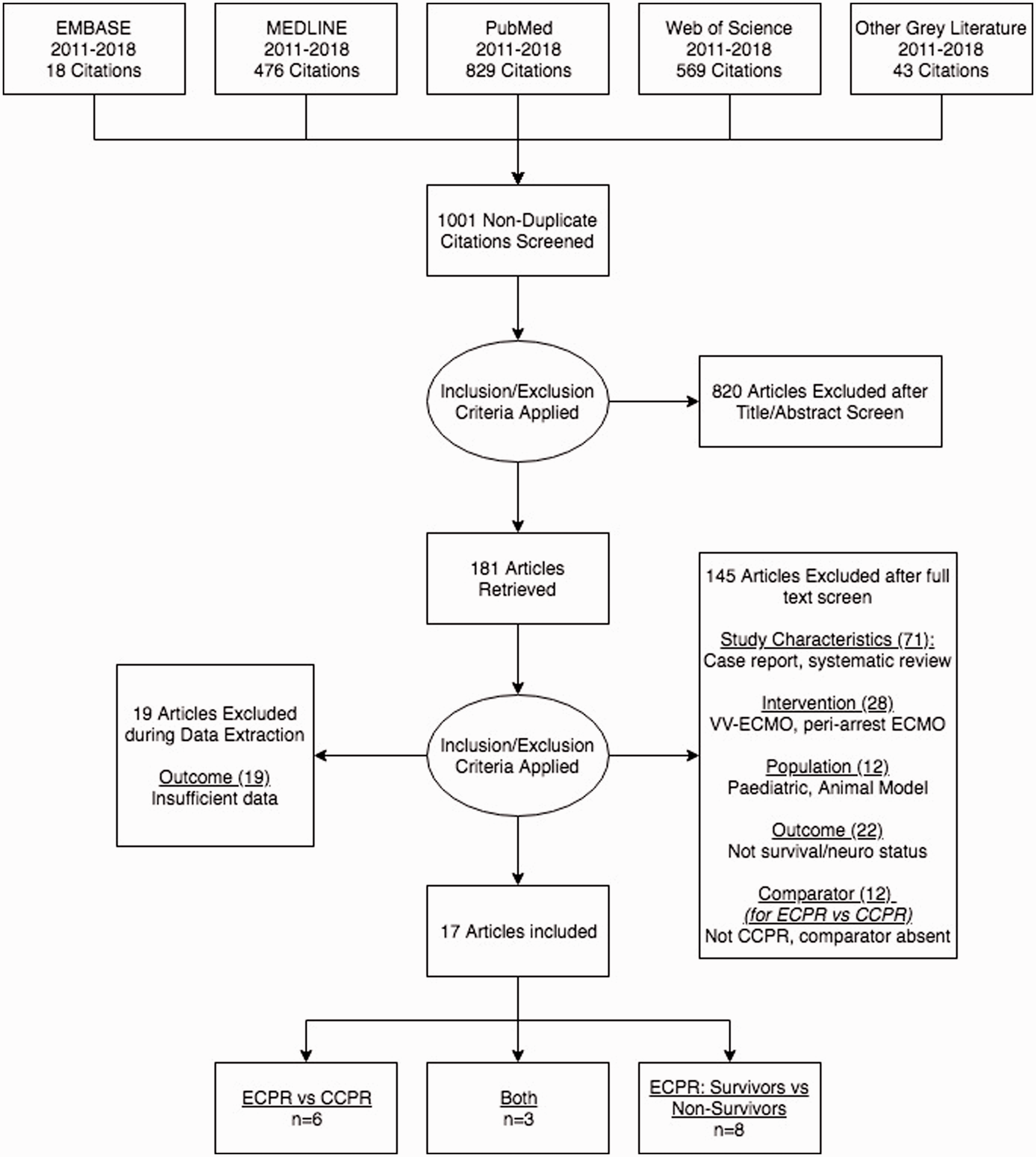
Study characteristics and quality
Six papers only examined the use of ECPR in comparison to CCPR. Eight papers only looked at the parameters of patients that survived ECPR and those that did not. Three papers addressed both areas.
Eleven papers were graded as being at moderate risk of bias,3,14–21 three as serious risk of bias4,22,23 and three as critical risk of bias24–26 (Figure 2).
Risk of bias assessment.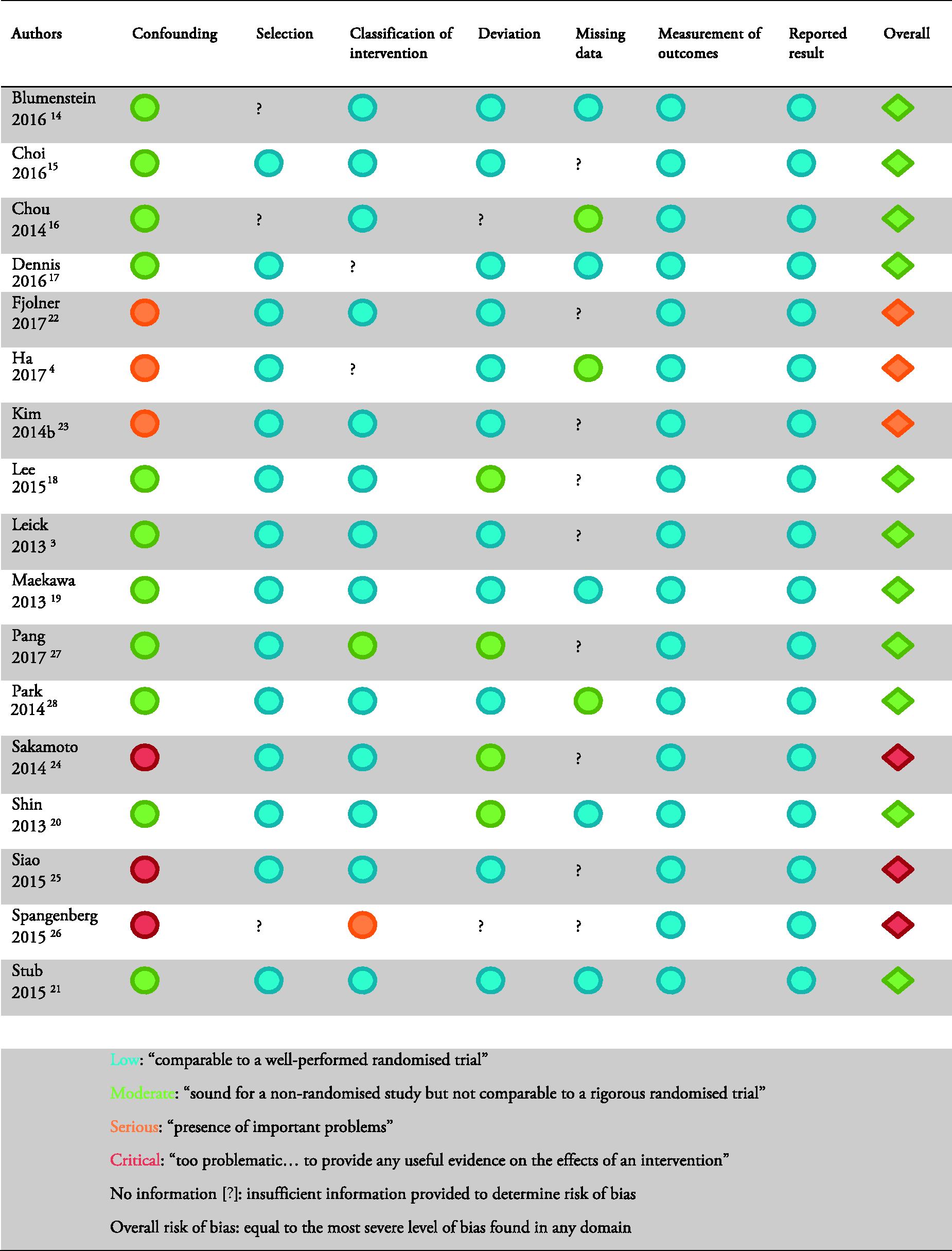
Regarding confounding variables, one paper was prospective in design, 21 six papers undertook propensity score matching14,15,19,20,23,27 and 10 papers completed logistic multivariate regression analysis.3,14–20,27,28
Publication bias was not assessed, as there were inadequate numbers of included trials to properly assess a funnel plot or more advanced regression-based assessments.
Comparison of ECPR and CCPR
Demographic details for ECPR versus CCPR studies.
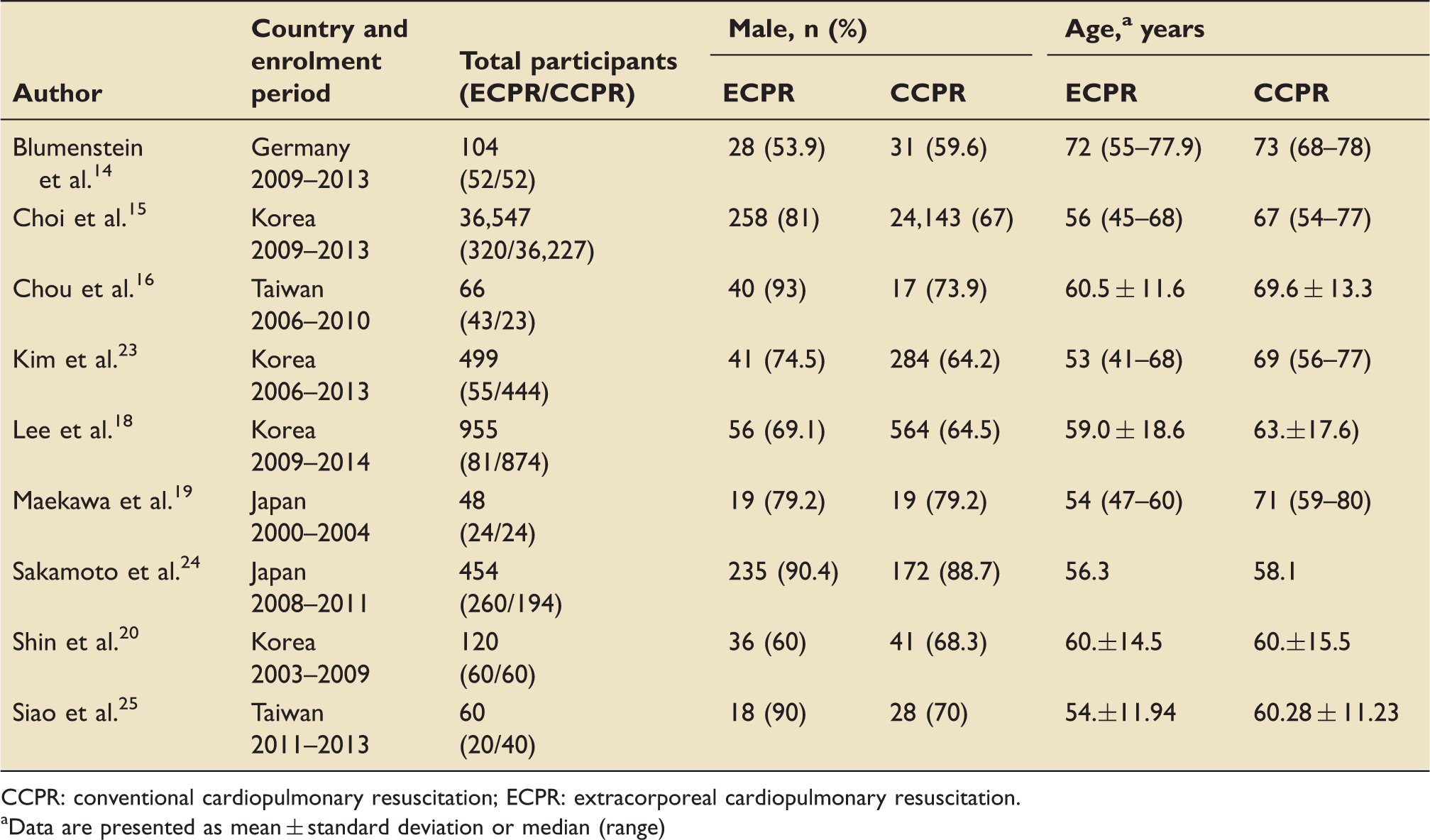
CCPR: conventional cardiopulmonary resuscitation; ECPR: extracorporeal cardiopulmonary resuscitation.
Data are presented as mean ± standard deviation or median (range)
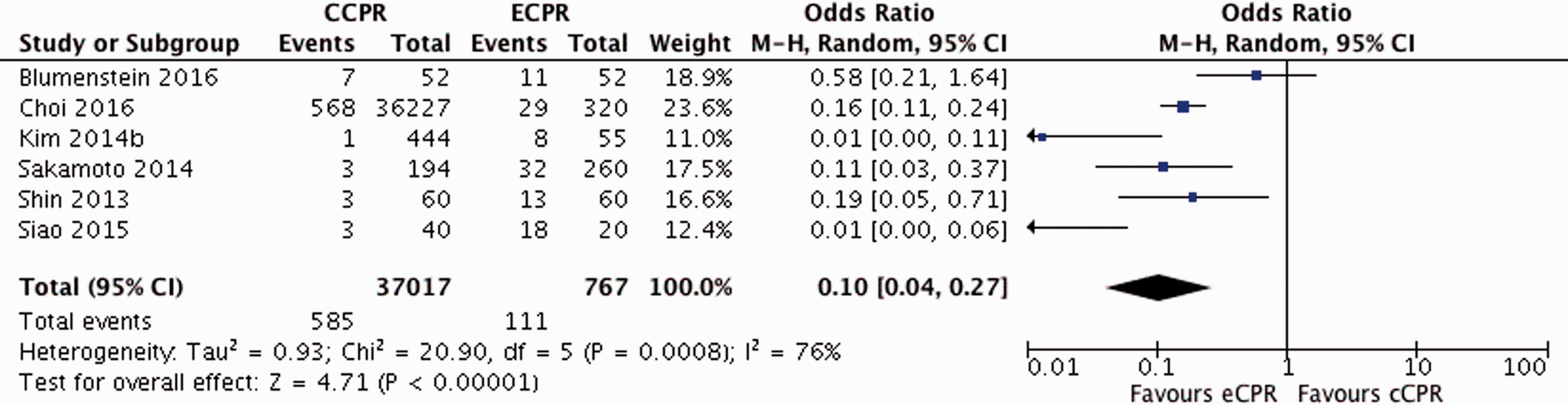
Figure 3 shows the forest plot for the 30-day/discharge survival for ECPR versus CCPR, while Figure 4 shows the forest plot for patients neurologically intact at this time interval.
Forest plot for survival at 30-day/discharge for ECPR versus CCPR. All data presented are non-randomised. Forest plot for neurologically intact survival at 30-day/discharge for ECPR versus CCPR. All data presented are non-randomised.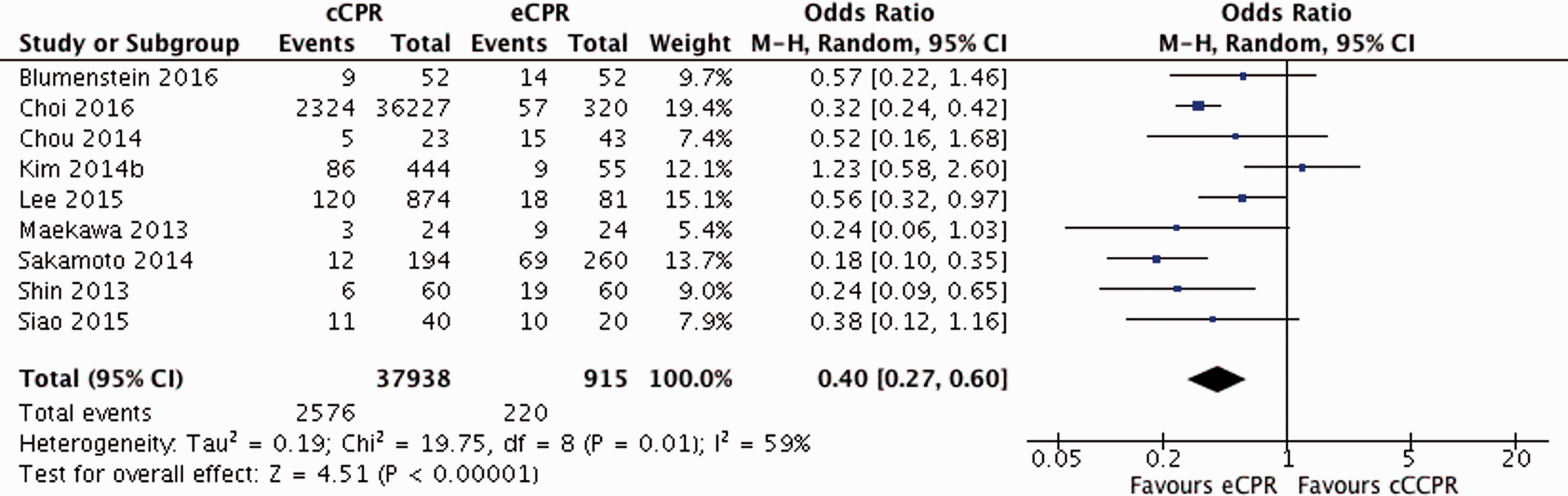
Survival
ECPR was associated with increased survival over CCPR at 30-day/discharge (OR 0.40, 95% CI 0.27–0.60) with moderate heterogeneity between studies (I2 59%) (Figure 3).
Neurological status
ECPR was associated with improved neurological outcomes in survivors over CCPR at 30-day/discharge (OR 0.10, 95% CI 0.04–0.27), although the heterogeneity between studies was high (I2 76%) (Figure 4).
Comparison of survivors and non-survivors in patients selected for ECPR
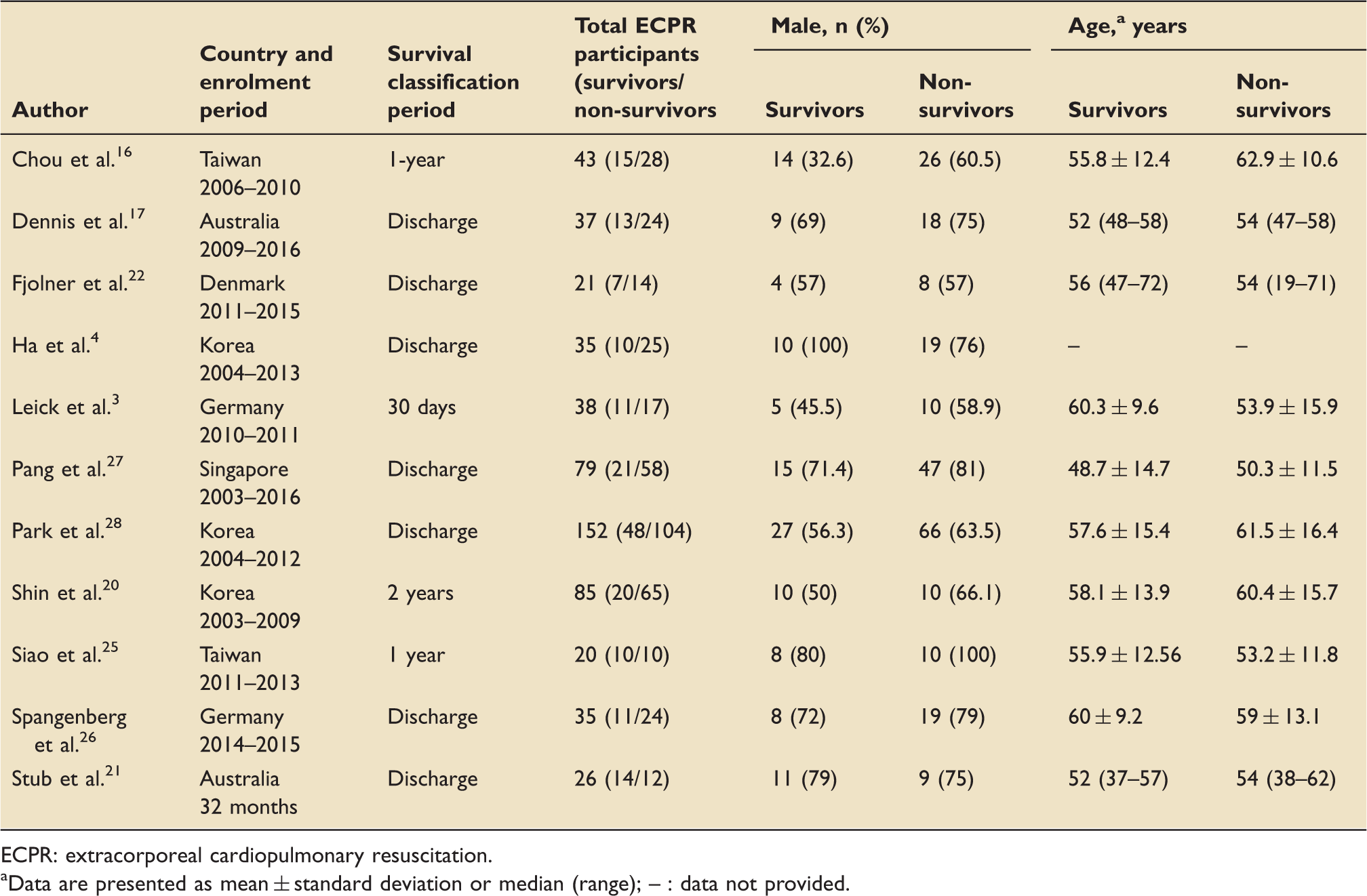
Table 3 shows the demographic details of the studies included in the comparison of surviving and non-surviving patients who received ECPR. Eleven studies were included overall. All but one
19
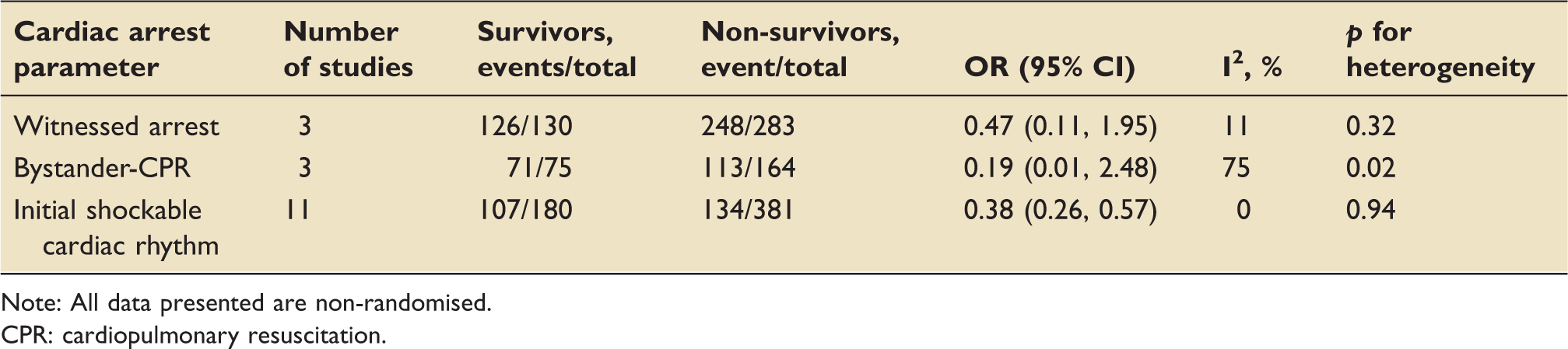
of the studies were retrospective observational. Table 4 shows the meta-analysis details for three of the cardiac arrest parameters analysed. A fourth parameter, arrest-to-ECPR interval, is shown in Figure 5.
Arrest-to-ECPR (min) forest plot analysis for ECPR survivors versus non-survivors. All data presented are non-randomised. Demographic details for ECPR survivors versus non-survivors. ECPR: extracorporeal cardiopulmonary resuscitation. Data are presented as mean ± standard deviation or median (range); – : data not provided. Cardiac arrest parameters for ECPR survivor versus non-survivor studies. Note: All data presented are non-randomised. CPR: cardiopulmonary resuscitation.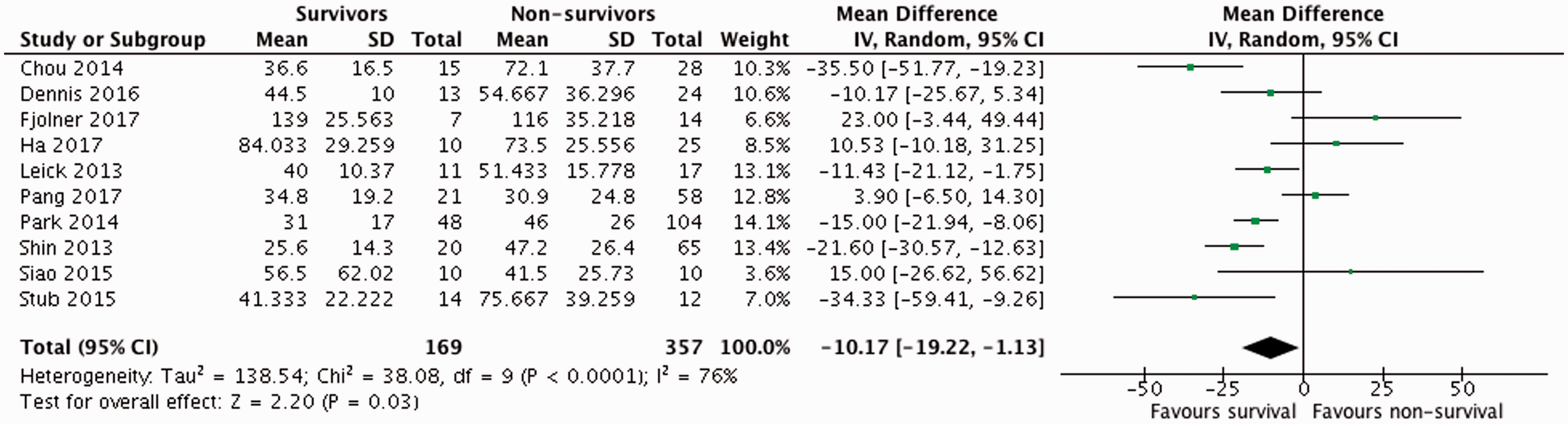
Demographics
There were not any significant differences between the sex or age of the survivors and non-survivors of ECPR in the studies examined.
Witnessed arrest
Eight studies reported the incidence of a witnessed arrest among survivors and non-survivors.3,4,17,20,22,25,26,28 In five of the studies, it was 100% in both groups.3,20,22,26,28 In two studies,4,25 survival was seen to be associated with having a witnessed cardiac arrest. One study reported a statistically significant difference. 4 A meta-analysis did not demonstrate any significant difference (OR 0.47, 95% CI 0.11–1.95).
No-flow duration
Two studies reported the no-flow duration for the participants of their studies; however, neither provided complete data. One study reported the ranges of time only and stated that there was a non-statistically significant difference between these. 25 In the other study, patients were dichotomised into groups where the no-flow duration was greater or less than 5 min and did not provide p values for these data. 17 No comparison was made, and hence meta-analysis could not be performed.
Bystander-CPR
Six studies reported the incidence of bystander-CPR among survivors and non-survivors of ECPR.4,17,20–22,26 In three studies, bystander-CPR was universal in both groups.20–22 In two studies, bystander-CPR was associated with survival and this was statistically significant.4,26 A meta-analysis of bystander-CPR was inconclusive (OR 0.19, 95% CI 0.01–2.48).
Initial shockable cardiac rhythm
All 11 studies reported the incidence of initial shockable cardiac rhythms among survivors and non-survivors of ECPR.3,4,16,17,20–22,25–28 In Siao et al., 25 this was a criterion for inclusion; hence, rates were 100% in both groups. Nine studies reported greater survival rates with an initial shockable cardiac rhythm,4,16,17,20–22,26–28 although this was only statistically significant in one. 28 Meta-analysis showed the presence of an initial shockable cardiac rhythm to be associated with survival (OR 0.38, 95% CI 0.26–0.57).
Arrest-to-ECPR time
Ten studies reported the arrest-to-ECPR time for their participants.3,4,16,17,20–22,25,27,28 Four reported increased survival with a longer arrest-to-ECPR period than the non-survivors.4,22,25,27 By contrast, six reported greater survival with a shorter arrest-to-ECPR period3,16,17,20,21,28; this was statistically significant in three studies.16,21,28 A meta-analysis showed a shorter arrest-to-ECPR interval to be associated with survival (MD of −10.17 min, 95% CI −19.22, −1.13), although again, heterogeneity between studies was high (I2 76%). Two papers included unwitnessed cardiac arrests in the arrest-to-eCPR analysis, but this was only 11 patients compared to an analysis total of 526, so the effect of the questionable inclusion of these patients is negligible at best.4,17
Discussion
Benefit over CCPR
Although there is potential for bias in the results, the data in this systematic literature review suggest that, when compared to CCPR, ECPR produces more survivors at 30-day/discharge15,19,20 and of those survivors, more are neurologically intact.15,19,24,25
ECPR can be used as a bridge to a definitive therapy, 16 such as primary percutaneous coronary intervention or as a tool to ‘buy time’, while the heart recovers in the presence of myocardial stunning. A potential explanation for why CCPR patients have worse outcomes compared to ECPR patients, despite both receiving definitive therapy, is that ECPR maintains organ perfusion from the moment it is initiated, preventing the multi-organ failure of a prolonged low-flow time with CCPR.
ECPR is a relatively old concept, 16 yet there is a lack of published evidence, and the majority of this is very limited for many reasons. Numerous studies lack a defined protocol for ECPR, possibly due to its relatively infrequent use.15,16,18 There is no unified and standardised data reporting in studies concerning its use. These render comparisons problematic. Without a strong evidence base, the use of ECPR is sporadic and often as part of an aggressive resuscitation approach, so that ECPR is often used in combination with other novel interventions such as therapeutic hypothermia and mechanical-CPR which may be confounding factors.15,21 Due to the lack of randomised controlled trials, propensity score matching has been used to balance confounding factors, but residuals from unmeasured covariates are likely to remain. 15 Due to the difficulties associated with propensity score matching and the relatively small numbers of patients undergoing ECPR, this results in the matched arms of each study having even smaller numbers of patients in each arm. To compound this, most of the data presented are single-centre experiences and hence cannot be easily generalised to different organisations or healthcare systems.14,16,18–20,23,25
Predictors of survival
If ECPR is better than CCPR, which patients are most likely to benefit? Prior studies have attempted to provide evidence for the former statement, but made little attempt to prove or disprove the latter. 29 Witnessed cardiac arrests,4,30 bystander CPR and arrests with short no-flow intervals are considered by most as important inter-related characteristics defining patients suitable for ECPR. This was not reflected in the literature reviewed and meta-analysis. This may be due to the low number of patients, the fact that cohort had already been chosen to receive ECPR and was not reflective of the entire population of patients and the low quality of the included studies. Indeed, there are few data about no-flow times and such data are difficult to capture in OHCA. Currently, the Utstein data templates do not include ECPR parameters.
The presence of an initial shockable cardiac rhythm in patients that received ECPR was found to be predictive of survival in this review and meta-analysis,22,28 fitting with previous research. 30 In cardiac arrests, generally, an initial shockable cardiac rhythm is associated with higher rates of survival. 31 By contrast, the duration of non-sufficient circulation has been demonstrated to be less important for survival and neurological outcome than the initial cardiac rhythm. 32 Hence, having an initial shockable cardiac rhythm may be a physiological indicator of the status of the heart in cardiac arrest, regardless of the various arbitrary time intervals that have passed. However, this observation was only made in patients that had a presumed cardiac aetiology for their arrest, which in itself is associated with greater survival from CCPR. 32
The low-flow time and the similar, arrest-to-ECPR time, are the most widely documented predictors of a good outcome in patients undergoing ECPR.3,20,21,26,28 CCPR only delivers 25–30% of cardiac output, 7 whereas ECPR produces effective coronary and organ perfusion. 17 Various other studies have looked at the difference in ECPR survival between IHCA and OHCA. 33 Historically, patients undergoing ECPR after IHCA have had better outcomes than OHCA patients, 33 although this may be in part due to different delays in starting ECPR. 33 Unlike other meta-analyses, 8 by not discriminating on the setting of ECPR in our meta-analysis, this has facilitated the comparison of pertinent variables such as the low-flow time across these different settings, allowing for more generalisable comparisons.
Limitations
This study has several limitations. Firstly, all the included studies were non-randomised retrospective observational studies at risk of bias and in particular confounding and selection bias. Although some employed propensity score matching to counter this, unmeasured confounders in small studies of heterogeneous study populations mean that selection bias is likely to remain. Furthermore, there was high heterogeneity between the studies used in the meta-analyses, which limits the conclusions that can be made from these. Secondly, multiple confounders were present including the non-standardised post-resuscitation care, the quality of CPR provided prior to ECPR and the operator experience of using ECMO at the various institutions. Thirdly, numerous studies reported the CPC of the study populations, but quality of life or physiologic status was not reported. Finally, due to a lack of homogeneity among papers and a lack of standardised reporting, the breadth of data collected from each study varied, making comparisons difficult. The methodology of this review is also subject to bias with a single assessor for risk of bias assessment and highly heterogeneous included studies.
Conclusions
Despite the advances in medical technology and knowledge, the treatment of OHCA remains a challenge, with persistently poor survival to discharge with a good neurological status. While acknowledging the risks of bias, both in the methodology and individual papers, the data presented in this review suggest that ECPR in selected patients could be associated with higher rates of survival to discharge with a higher number of neurologically intact survivors in this group. Patient characteristics that are associated with survival include those with have an initial shockable cardiac rhythm and a reduced low-flow time.
However, there is still no high-quality evidence supporting the use of ECPR. Many clinical trials are ongoing, which will hopefully provide some much needed answers in this potential adjunct to resuscitation.
Supplemental Material
Supplemental material for A systematic literature review and meta-analysis of the effectiveness of extracorporeal-CPR versus conventional-CPR for adult patients in cardiac arrest
Supplemental Material for A systematic literature review and meta-analysis of the effectiveness of extracorporeal-CPR versus conventional-CPR for adult patients in cardiac arrest by Callum J Twohig, Ben Singer, Gareth Grier and Simon J Finney in Journal of the Intensive Care Society
Footnotes
Acknowledgments
The authors would like to thank the library staff from Barts Health NHS Trust for assistance with producing the search strategy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.