
Abstract
Purpose
Extracorporeal membrane oxygenation use may predispose patients to developing conditions that require either consultation with a general surgeon or a general surgical procedure. We aimed to evaluate the incidence and outcomes of adult extracorporeal membrane oxygenation patients who underwent general surgical procedure.
Methods
This was a single institution retrospective study of adult extracorporeal membrane oxygenation patients from 2012 to 2015. Outcomes were compared between patients who underwent general surgical procedure with those that did not.
Results
Of the 115 patients, 54 (46.9%) required a general surgeon while 42 (36.5%) required a general surgical procedure. No significant differences were observed in mortality (35.7% vs. 46.6%; p = 0.256) and extracorporeal membrane oxygenation-related complications (45.7% vs. 32.5%; p = 0.175). Patients with general surgical procedure had longer extracorporeal membrane oxygenation duration (13 vs. 5 days; p < 0.0001), longer length of stay (36 vs. 15 days; p = 0.0005), more wound infections (19.05% vs. 5.5%; p = 0.029), more urinary tract infections (38.1% vs. 10.96%; p = 0.0006), and more pulmonary emboli (19.05% vs. 5.48%; p = 0.029). In general surgical procedure patients, no difference in bleeding complications was observed regardless of anti-coagulation status (29.4% vs. 16%; p = 0.44).
Conclusion
Common general surgical procedures are safe and feasible in adult extracorporeal membrane oxygenation patients. Duration of extracorporeal membrane oxygenation was longer for patients requiring general surgical procedure. Despite the common use of anticoagulants, there was no increase in bleeding events in general surgical procedure patients.
Introduction
Extracorporeal membrane oxygenation (ECMO) is a life support device for patients with severe cardiac and/or respiratory failure. Theoretical advantage of using ECMO as a life support device rests in its ability to provide artificial cardiopulmonary support while allowing the heart and/or lungs to recover. 1 ECMO is being increasingly used in adult patients owing to recent advances in technology combined with increasing experience and availability of data.1–3 Some of the complications associated with ECMO use may predispose patients to developing conditions that require either consultation with a general surgeon or a general surgical procedure (GSP).
There remains a paucity of literature on this topic, leaving much to be learned. Recent experiences with performing GSPs on adult ECMO patients have demonstrated that about 39% require a GSP; abdominal exploration, tracheostomy, and/or bowel resection are some of the most commonly performed procedures.2,4 Adult ECMO patients who require a GSP have been noted to have higher incidence of hospital length of stay, wound infections, and bleeding complications along with increasing trend toward mortality.2,4,5
At our institution, adult patients who are put on ECMO are generally managed by critical care intensivists and cardiac surgeons. General surgeons are consulted when (1) the patient develops signs and symptoms consistent with a general surgical disease entity such as cholecystitis or abdominal compartment syndrome or (2) the patient requires a GSP such as tracheostomy or gastrostomy. In this retrospective review of our institution’s ECMO database, we evaluated the role of general surgeons in managing adult ECMO patients to determine the incidence, type, and outcomes of GSPs performed on adult ECMO patients.
Methods
After approval from our organization’s institutional review board, this retrospective study was conducted at a large academic, tertiary care health network in southeastern Pennsylvania. We examined data from January 2012 through July 2015 from the institution’s ECMO database for patients, aged 18 years or older, initiated with venovenous (VV) or venoarterial ECMO during their hospital stay.
General surgical procedures
Of this patient cohort, records were evaluated, using the International Classification of Disease (ICD-9) diagnosis codes, to determine whether the patients underwent any of the following types of GSPs: percutaneous or open cholecystostomy; laparoscopic or open cholecystectomy; percutaneous, endoscopic, laparoscopic, or open gastrostomy; percutaneous, endoscopic, laparoscopic, or open jejunostomy; percutaneous or surgical tracheostomy; open or laparoscopic splenectomy abdominal exploration; diagnostic laparoscopy; bowel resection; decompressive laparotomy; drainage of intra-abdominal abscess; wound debridement; and fasciotomy. Patients were excluded if ECMO was initiated after a GSP or if they underwent a GSP after being de-cannulated from ECMO. The resulting patient population was then compared to adult patients on ECMO who did not require a GSP.
Variables of interest
We collected variables including age, gender, race, type of ECMO, indication for ECMO, indications for initial admission, obesity (body mass index > 40), diabetes (documented type I or II), heart disease (documented coronary artery disease, pulmonary hypertension, previous myocardial infarction, coronary artery bypass graft, peripheral vascular disease, or congestive heart failure), lung disease (documented chronic obstructive pulmonary disease, emphysema, bronchitis, or asthma), hypertension (documented), renal failure (defined as glomerular filtration rate <60), autoimmune disease (documented diabetes type I, Crohn’s disease, ulcerative colitis, rheumatoid arthritis, multiple sclerosis, sarcoidosis, and lupus), and malignancy (defined as active malignancy within the past 5 years).
Illness severity of each patient was determined according to the Sequential Organ Failure Assessment score, which has been used to predict prognoses of critically ill patients. 6 Outcomes determined included total length of stay, duration of ECMO support, complications, and survival. ICD-9 diagnosis codes were used to identify complications, including pneumonia, wound infection, urinary tract infection, acute renal failure, bleeding complications, deep venous thrombosis/pulmonary embolism, myocardial infarction, stroke, abdominal compartment syndrome, sepsis, and death.
Bleeding complications
We collected data on the anticoagulation status of patients who underwent GSPs: either fully anti-coagulated, as identified by therapeutic partial thromboplastin time (PTT, defined as >60 s) or therapeutic international normalized ratio (INR, defined as >1.5) or not fully anti-coagulated, as identified by less than therapeutic levels of PTT or INR. Operative bleeding complication rates were compared between these two groups. To explore the incidence of bleeding complications, we searched the database for episodes of major bleeding both by examining ICD-9 codes for major hemorrhage during surgery and by deciphering operative reports, hospital summaries, and daily progress notes. Additionally, for patients with major hemorrhage, we collected information about the bleeding location: the ECMO cannula site, surgical site, oropharyngeal site, or other invasive device site(s). The amount of blood products—packed red blood cells (PRBC), platelets (PLT), and fresh frozen plasma (FFP)—transfused between the two groups during surgery and 48 h post-operatively were quantified and compared as well.
Statistical analyses
Univariate analysis was performed to assess the relationship between patients with and without a GSP while on ECMO. A two-sample t-test was used to compare means for continuous variables with normal distributions, or a Mann Whitney U test was used for continuous variables found to be not normally distributed. Two-sided χ2 test or Fisher’s exact test was used to compare proportions. Patients were then regrouped into fully/not fully anti-coagulated and tests were redone. For all analyses, statistical significance was set at p < 0.05 and all were conducted two-tailed. All statistical analyses were performed using Statistical Analysis System (SAS) software, version 9.3 (SAS Institute, Inc., Cary, NC).
Results
Incidence and type of GSP
Baseline patient characteristics. a
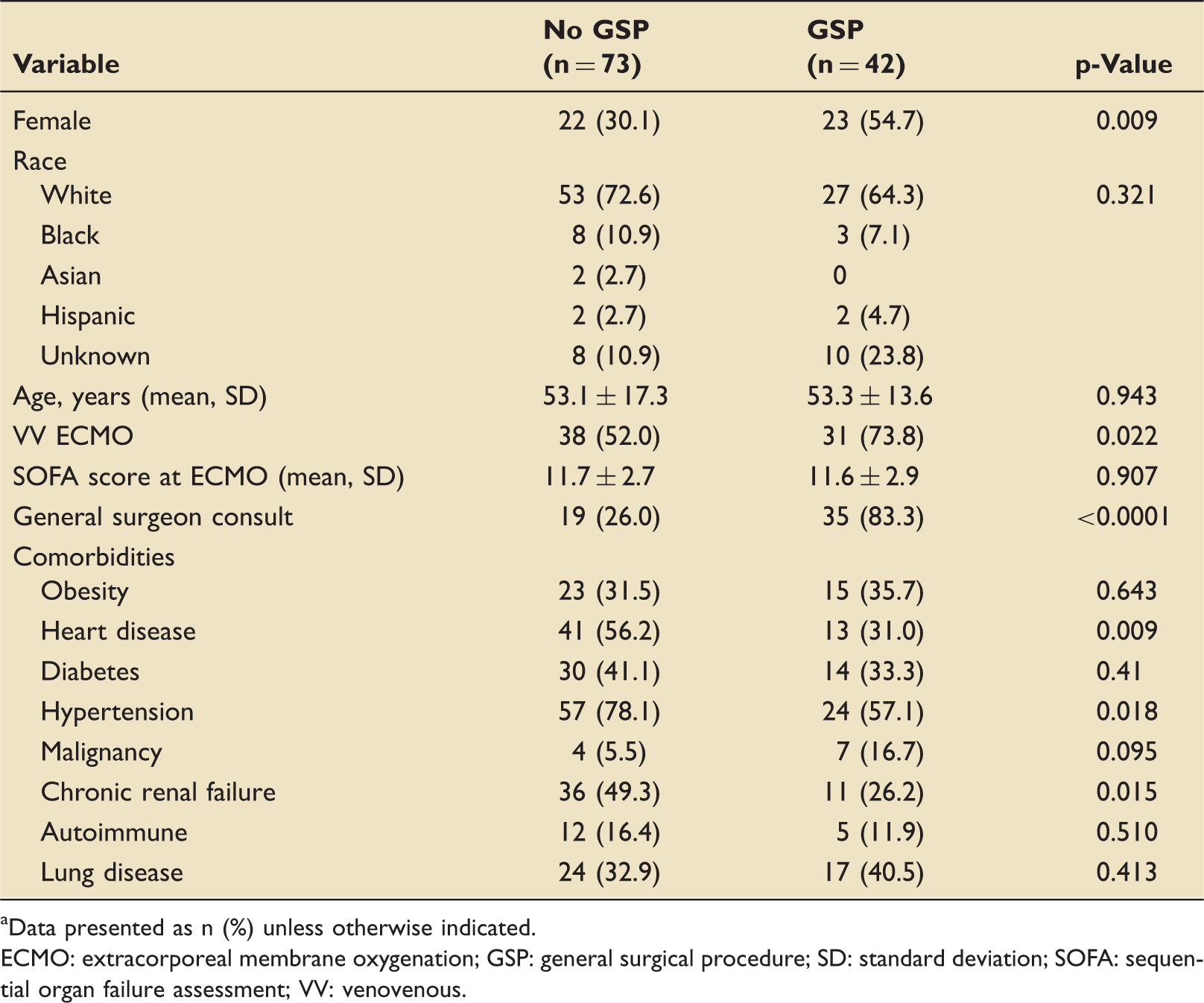
aData presented as n (%) unless otherwise indicated. ECMO: extracorporeal membrane oxygenation; GSP: general surgical procedure; SD: standard deviation; SOFA: sequential organ failure assessment; VV: venovenous.
Types and frequency of GSPs performed.
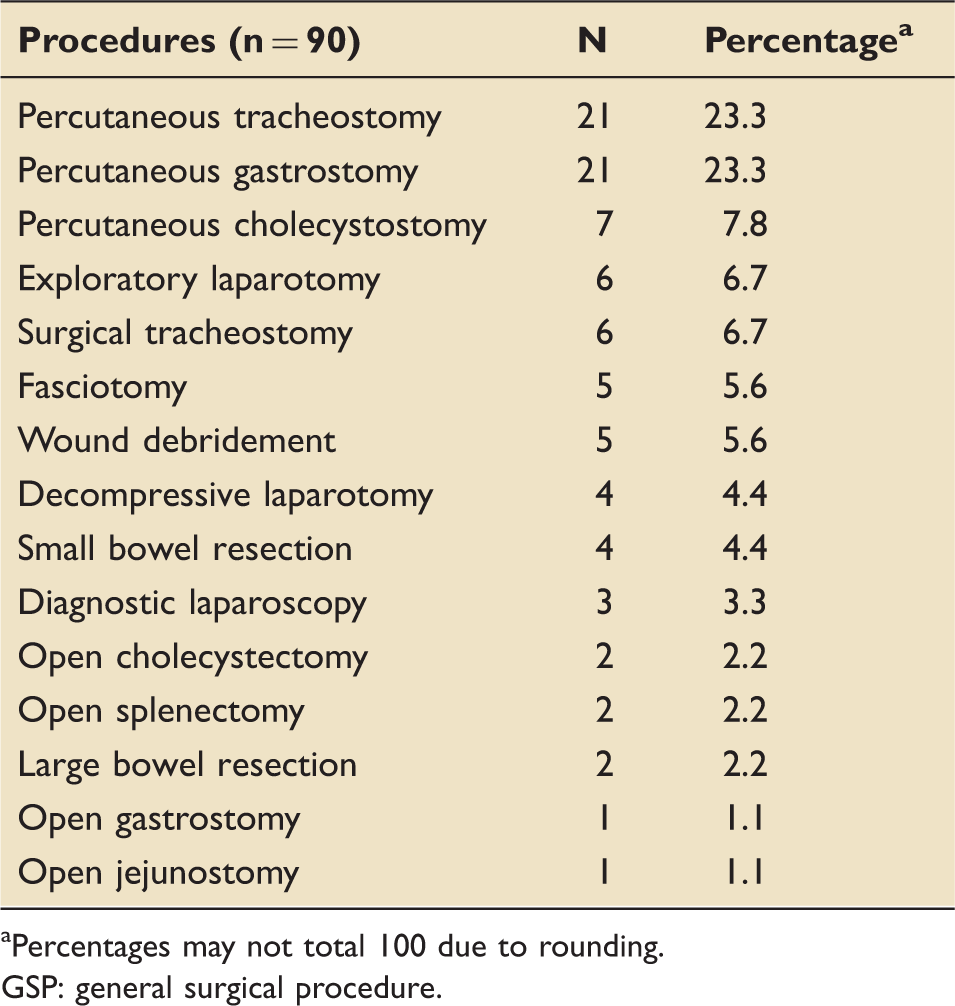
aPercentages may not total 100 due to rounding. GSP: general surgical procedure.
Baseline characteristics
Outcomes.
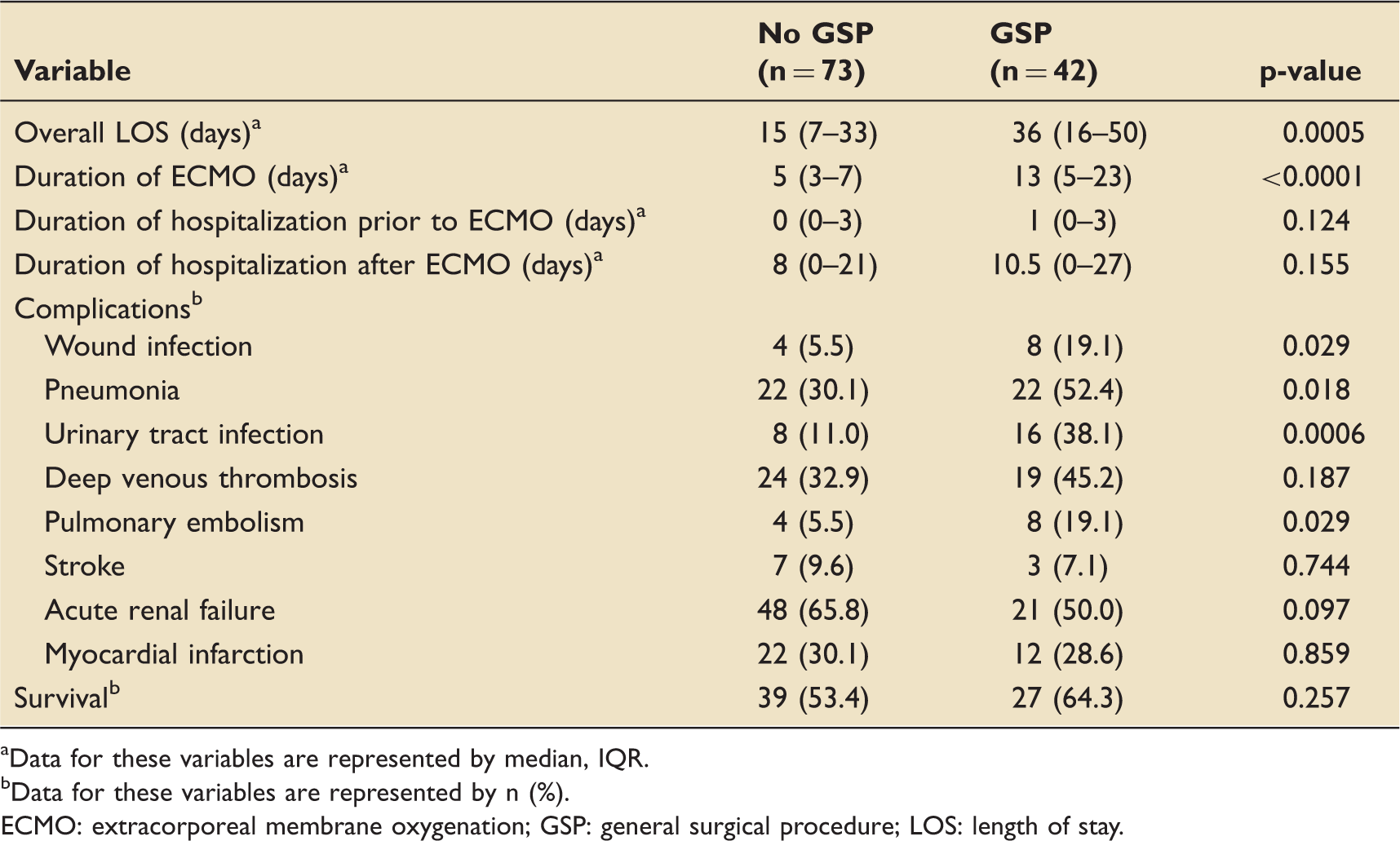
Data for these variables are represented by median, IQR.
Data for these variables are represented by n (%).
ECMO: extracorporeal membrane oxygenation; GSP: general surgical procedure; LOS: length of stay.
Outcomes
Table 3 outlines the overall outcomes. Undergoing a GSP while on ECMO was associated with longer overall length of stay, but had no statistically significant effect on survival. The GSP cohort had increased incidence of wound infections, pneumonia, urinary tract infections, and pulmonary embolism compared to cohort who did not have a GSP. Duration of stay after ECMO was discontinued was not significantly different between the two groups.
We categorized complications into either ECMO-related (oxygenator failure, cannula issues, or circuit changes) or patient-related (wound infection, sepsis, urinary tract infection, myocardial infarction, stroke, acute renal failure, deep vein thrombosis, pulmonary embolism, and pneumonia) and found no statistically significant association between having a complication and undergoing a GSP (ECMO-related, 38.1 vs. 26%, p = 0.176; patient-related, 97.6 vs. 91.8%, p = 0.420). On further sub-analysis, we removed all the patients with an admitting diagnosis of respiratory conditions because the majority of these patients are admitted with community acquired bacterial, viral, or fungal pneumonia. After adjusting for this confounding variable, there was no longer a statistically significant association between undergoing a GSP and contracting nosocomial pneumonia (40 vs. 26.1%, p = 0.258).
Patients in a total of 9 ECMO runs experienced an episode of major bleeding. Of this group, 29.4% experienced major bleeding while fully anti-coagulated compared to 16.0% who were not fully anti-coagulated. The frequency of GSP patients who required blood products transfusion intra-operatively was 35% PRBC, 40% PLT, and 26% FFP. Median amount of individual blood products transfused intra-operatively for GSP patients were 4 U PRBC, 1 U PLT, and 4 U FFP. Frequency of GSP patients who required blood products transfusion post-operatively (48 h) was 47.6% PRBC, 38.1% PLT, and 23.8% FFP. Median amount of individual blood products transfused post-operatively for GSP patients were: 4.5 U PRBC and 1.5 U PLT. Mean number of FFP units transfused post-operatively for GSP patients were 7.4 (SD 5.8). Those who were not transfused any blood product were more likely to survive than those who had transfusions (100% vs. 57.1%, p = 0.038).
Discussion
As ECMO use continues to increase in adult patients, the role of general surgeons and GSPs will continue to grow proportionally. In this study, we reviewed our institution’s experience since the beginning of the adult ECMO program in 2012 and found no statistically significant difference in overall mortality between adult ECMO patients who underwent GSP and those who did not need GSP. We found that adult patients who require GSP spend longer time on ECMO and in the hospital with higher incidence of wound infections, urinary tract infections, pulmonary embolism, and bleeding complications.
Taghavi et al. 2 sampled approximately 20% of non-federal United States hospitals and found that 39% of adult ECMO patients required a GSP, with abdominal exploration and/or bowel resection being performed approximately 46% of the time. Similarly, approximately 36% of all adult ECMO patients at our institution required at least one GSP. The most common procedure performed was open or percutaneous tracheostomy. Second and third most common procedures performed were open or percutaneous gastrostomy and exploratory or decompressive laparotomy.
Tracheostomy is one of the most common procedures performed on ECMO patients.2,4 In fact, approximately 70% of adult ECMO centers globally perform tracheostomy. 7 At our institution, general surgeons typically perform tracheostomies infrequently; cardiothoracic surgeons perform them as well.
Early enteral feedings in adult ECMO patients are preferred and safe.8,9 For patients who are expected to remain either intubated or switched to a tracheostomy tube, enteral feeding via gastrostomy feeding tube is ideal. Our study findings reflected this best practice: we performed percutaneous or open gastrostomy on approximately 52% (22/42) of adult ECMO patients.
At our institution, tracheostomy and gastrostomy are frequently performed together for those patients deemed to require long-term (>7 days) respiratory and/or nutrition support. In this study, all patients in the GSP group who had a gastrostomy (22, 52%) also had a tracheostomy performed simultaneously.
ECMO patients are at increased risk for developing abdominal compartment syndrome due to massive fluid resuscitation requirements, capillary leak due to cardiac and/or pulmonary failure, and systemic inflammatory response induced by underlying disease process.10–12 In a case series of five pediatric patients on ECMO who developed abdominal compartment syndrome, two required decompressive laparotomies. 11 In addition, in a case series of two adult ECMO patients who developed abdominal compartment syndrome, one required decompressive laparotomy although both were candidates for the procedure. 10 Our experience demonstrates that laparotomy performed to explore, diagnose, and treat intra-abdominal pathologies including abdominal compartment syndrome, intestinal necrosis, or visceral bleeding is not uncommon. Clinicians caring for these complex and critically ill ECMO patients should not hesitate to consult a general surgeon in order to avoid catastrophic intra-abdominal processes. General surgeons, in turn, must maintain vigilance to search for and exclude these intra-abdominal processes.
The development of cholestasis and subsequent risk of cholecystitis, requiring surgical procedure for neonates and infants on ECMO, has been described in the literature.13–15 Increased hemolysis, either due to membrane oxygenator or due to anticoagulation, predisposes ECMO patients to development of hyperbilirubinemia which may ultimately lead to cholecystitis.14,15 There has also been evidence of ischemic biliary injury following ECMO use in an adult patient. 16 In our patient population, 10% of GSPs performed were either cholecystostomy tube placement or cholecystectomy for presumed diagnosis of cholecystitis.
Adult ECMO patients who require a GSP have been noted to have higher incidences of hospital length of stay, wound infections, and bleeding complications.2,5 Chestovich et al. 4 noted a trend toward increased mortality in their adult ECMO patients who required GSP. Our findings confirm that adult ECMO patients who require GSP spend a significantly longer time—almost 18 days—in the hospital. We also confirm the previously reported finding of respiratory failure as indication for ECMO being associated with requiring GSP. 2 One of the novel findings of this study is the association of ECMO duration with requirement of a GSP. Further studies in this particular area are needed to draw strong conclusions, however.
Previously reported higher incidence of wound infections 2 are confirmed by this study, with the GSP cohort experiencing four times as many wound infections as the non-GSP cohort. This finding is expected: patients with surgical incisions are naturally prone to developing wound infection. It must be emphasized that those patients in the non-GSP cohort who experienced wound infections in this study also had non-GSPs performed (cardiac, thoracic, or vascular procedures).
Major bleeding, one of the more common complications for adult ECMO patients, 1 is often noted in patients requiring a GSP.2,4,5,7 Patients placed on ECMO generally require anticoagulation to keep the catheters, circuits, and oxygenators from being clotted, which dampens the devices’ desired effects. It is important, therefore, to determine the rate of bleeding complications in these patients and assess how it might affect outcomes of ECMO patients who require a GSP. In this study, patients experienced episodes of major bleeding in only nine ECMO runs, perhaps too small a sample size to draw any definite conclusions on the rate of bleeding complications and its effect on outcomes. Regardless, we found that almost twice as many patients experienced an episode of major bleeding while fully anti-coagulated compared to those who were less than fully anti-coagulated.
Blood transfusion and survival in ECMO patients requiring a GSP.
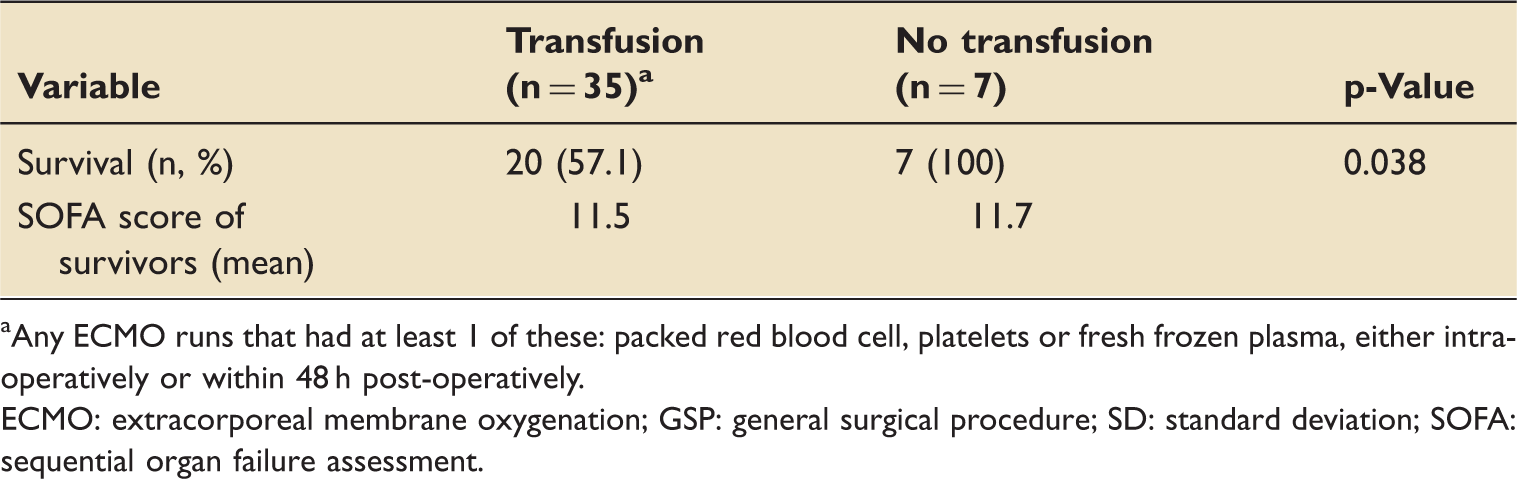
Any ECMO runs that had at least 1 of these: packed red blood cell, platelets or fresh frozen plasma, either intra-operatively or within 48 h post-operatively.
ECMO: extracorporeal membrane oxygenation; GSP: general surgical procedure; SD: standard deviation; SOFA: sequential organ failure assessment.
This study has inherent limitations due to its retrospective, single-institution nature. Also, several of the sub-sample sizes were too small to draw definite conclusions, as in the relationship of anticoagulation to major bleeding episodes. There also appears to be selection bias in terms of patients with lower incidence of co-morbidities (such as heart disease, hypertension, and chronic renal failure) underwent GSP. It is feasible that these patients were selected for an operation since they are considered “low-risk.” However, our results have shed some light on the incidence of GSPs and associated outcomes for patients in an adult ECMO population.
Conclusions
In this novel single-institution retrospective study of a large patient population, we demonstrate that performing GSPs on adult ECMO patients has no effect on overall mortality. Novel findings include the association of ECMO duration with requirement of a GSP and increased incidence of wound infection, urinary tract infection, and pulmonary embolism. The results of this study underscore the importance of excellent surgical technique, tissue handling, and conservative blood transfusion for this patient population. Controlled prospective, multi-center trials are needed to further explore outcomes of adult ECMO patients who require surgical procedures.
Footnotes
Acknowledgements
The authors thank Jane S Trumbauer, Surgical Scholar Specialist, for logistical support in preparation for the study. They also express appreciation to Jacqueline Grove, medical editor, for assistance with editing and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.