
Abstract
Introduction:
Stroke is a leading cause of mortality and morbidity in China. Of the different subtypes of ischemic stroke, cardioembolic stroke is of particular importance because it is potentially preventable. This study aimed to evaluate the usefulness of measuring N-terminal pro-brain natriuretic peptide in the emergency department in early recognition of patients with cardioembolic stroke.
Methods:
This was a multicenter prospective cohort study conducted from 1 June 2015 to 30 June 2016 in four emergency departments. Adult patients with acute ischemic stroke were recruited. Plasma N-terminal pro-brain natriuretic peptide was measured in the emergency department. Discharge diagnosis was determined by neurologists according to the Trial of ORG 10172 in Acute Stroke Treatment criteria. The diagnostic performance of N-terminal pro-brain natriuretic peptide was assessed by measuring the sensitivity, specificity, receiver operating characteristic curve, and the area under curve.
Results:
In all, 258 patients were analyzed. Of them, 17.9% were diagnosed with cardioembolic stroke. The optimal cut-off concentration, sensitivity, specificity, and the area under the curve of the plasma N-terminal pro-brain natriuretic peptide concentration suitable to distinguish cardioembolic stroke from other subtypes of stroke were 501.2 pg/mL, 82.6%, 80.2%, and 0.87 (95% confidence interval: 0.83–0.92), respectively.
Conclusion:
Emergency physicians should strongly consider cardioembolic stroke in patients presented with acute ischemic stroke with an N-terminal pro-brain natriuretic peptide level over 501.2 pg/mL. However, it must be considered in context with clinical assessment and judgment before making treatment decisions.
Introduction
Stroke is the leading cause of death and disability in China. Approximately 3.5 million people suffer a new or recurrent stroke annually in China.1,2 Once the diagnosis of acute ischemic stroke has been made, etiologic classification should be done as soon as possible to discern the best secondary prevention treatment.3–5 The American Heart Association (AHA) and American Stroke Association (ASA) guidelines recommend that acute ischemic stroke patients be classified into five subtypes according to the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) criteria: large artery atherosclerosis (LAA), cardioembolism (CE), small artery occlusion (SAO), stroke of other determined etiology (SOE), or stroke of other underdetermined etiology (SUE).3–5 Particular focus should be on the CE stroke subtype due to its high recurrence rate and poor outcome including death.6–13
The recurrence of CE stroke is largely preventable by early recognition and implementation of anticoagulant therapy.14–16 A set of diagnostic tests including transcranial doppler (TCD), electrocardiogram (ECG), long-term cardiac monitoring, transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), ultrasound cardiogram (UCG), magnetic resonance angiography (MRA), digital subtraction angiography (DSA), and/or computed tomographic angiography (CTA) are selected to identify the TOAST subtype.3–6 Early identification of CE subtype can allow physicians to consider early initiation of anticoagulation and thus probably better patient outcome. However, some tests are unavailable in the emergency departments (EDs) and may be delayed until after admission. Some tests are expensive and invasive which are not recommended for the initial or routine use.
It has been shown that brain natriuretic peptide (BNP)/N-terminal pro-B-type natriuretic peptide (NT-proBNP) level is significantly higher in CE patients than in other TOAST subtypes.17–24 Our previous study had set up a new algorithm for suspected stroke patient management with a B-type natriuretic peptide point-of-care testing (POCT) platform in the ED. It showed that CE subtype of stroke should be strongly considered with a plasma BNP level greater than 66.50 pg/mL.12,24 However, the performance of this algorithm for suspected stroke patients with a NT-proBNP POCT platform and the optimal cut-off value of NT-proBNP concentration for preliminary recognition of CE stroke patients in the ED is unknown among the Chinese population. Therefore, we conducted a prospective and multicenter study to measure the optimal cut-off value of NT-proBNP to differentiate the CE subtype from the other TOAST subtypes and share our experience with using a BNP/NT-proBNP POCT platform on suspected ischemic stroke patients in the ED.
Methods
Setting
A multicenter prospective cohort study was conducted in the EDs in Guangdong General Hospital, Qingyuan Municipal People’s Hospital (QMPH), Foshan Hospital of Traditional Chinese Medicine (FSTCM), and Zhongshan People’s Hospital from 1 June 2015 to 30 June 2016. These are tertiary-care teaching hospitals located in Guangdong Province, South China. Each ED has a stroke unit. The study was approved by the local ethics committees.
Participants
Patients who were older than 18 years and presented to the 4 ED with clinical features of acute ischemic stroke within 72 h of symptom onset were included. Exclusion criteria included the following: (1) age <18 years; (2) transient ischemic attack (TIA) was suspected; (3) cerebral hemorrhage was suspected or diagnosed on arrival; (4) history of recent head trauma or surgery; (5) history of previous stroke with neurologic deficits; (6) pregnancy, dialysis, cancer, severe psychiatric illness, or alcoholism; (7) obvious signs of cardiac, renal, hepatic failure, severe infection, or dyspnea on arrival; (8) current or recent myocardial infarction or cardiogenic shock; or (9) leave against medical advice.
The algorithm
This algorithm for suspected stroke patient management is based on the AHA and ASA stroke guidelines (Figure 1).3–5 At the third step of the algorithm, intravenous access was obtained and the patient’s blood samples were collected from a peripheral vein and put into tubes containing aprotinin and ethylenediaminetetraacetic acid (EDTA). The first blood sample was measured immediately using a NT-proBNP POCT platform. It was measured by the Roche Cobas h 232 POCT platform (Roche diagnostics GmbH, Mannheim, Germany). The test strips (CARDIAC proBNP+) contain monoclonal and polyclonal antibodies against epitopes of the NT-proBNP molecule of which one is gold-labelled and the other biotinylated. The system is automatically calibrated when a test strip is inserted. Each lot of the Roche CARDIAC proBNP+ test strips is calibrated against the Elecsys proBNP test. The measurement range is 60–9000 pg/mL. The concentration of plasma NT-proBNP can be quantified within 12–15 min.12,24,25 Stroke was defined according to the World Health Organization as “rapidly developing clinical signs of focal/global disturbance of cerebral function, with no apparent cause other than that of vascular origin.’’1–5 Cerebral infarction was confirmed on CT and/or the diffusion weighted magnetic resonance imaging (MRI). When a diagnosis of acute ischemic stroke was confirmed and the plasma NT-proBNP concentration was greater than the reference index, the emergency physician would communicate with the neurologists so that further workup for CE stroke could be implemented as early as possible.12,24–26 Further examinations included continuous ECG monitoring, 24-h Holter ECG, duplex carotid and cardiac ultrasound, TCD, TEE, MRI or MRA, and conventional cerebral angiography and were determined by neurologists in the stroke unit.12,24 The discharge diagnosis and TOAST subtypes were confirmed by a group of senior neurologists at FSTCM according to the AHA & ASA and Chinese stroke guidelines.1–6 The following variables were assessed: age, sex, previous cerebral and cardiac disease history, chronic renal failure, vascular risk factors, blood pressure on arrival, the results of blood samples and brain imaging findings, Scandinavian Stroke Scale (SSS) score on arrival, etiologic subtype of stroke, and functional outcome at hospital discharge using the modified Rankin Scale (mRS).12,24 Atrial fibrillation (AF) was diagnosed by 12-lead ECG, continuous ECG monitoring, 24-h Holter ECG, or TEE according to the Chinese Society Of Neurology’s criteria.1,2 The SSS score on admission was categorized as severe (SSS score ≤25) and non-severe (SSS score: mild 43–58, moderate 26–42). Poor outcome was defined as mRS greater than or equal to 3 or death. 27
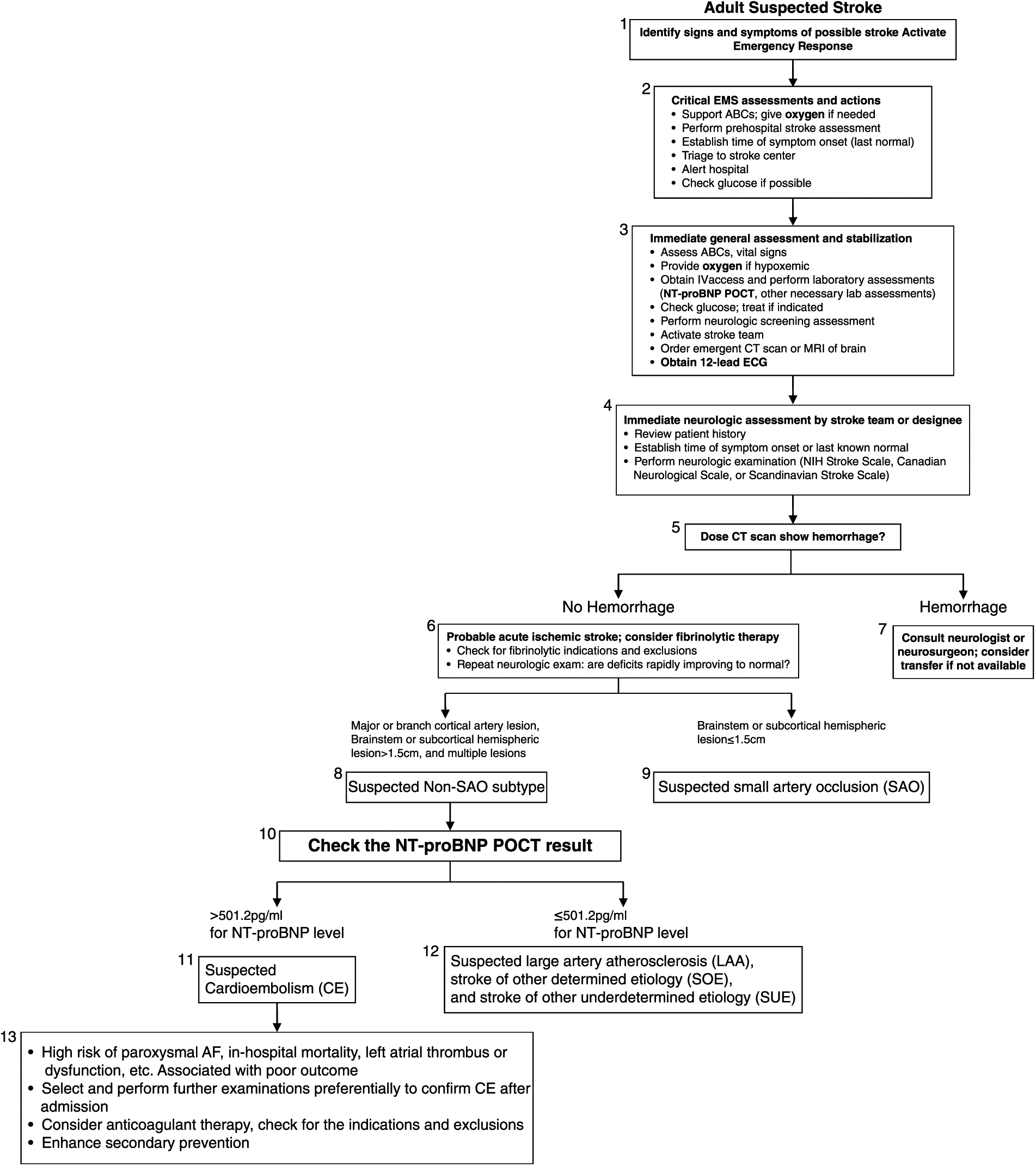
The algorithm for suspected stroke patient management with NT-proBNP POCT platform in the ED.
Statistical analysis
Data were entered into a Microsoft Excel database and analyzed using SPSS 21.0 (IBM SPSS Statistics, version 21, USA). Descriptive statistics were used to describe the patients. Differences in the clinical characteristics, including NT-proBNP level, between TOAST subtypes were analyzed by one-way analysis of variance for quantitative variables with normal distribution, the Kruskal–Wallis test for quantitative variables with skewed distribution, and the Pearson χ2 test for qualitative variables.
Any two TOAST subtypes were compared and analyzed by the Bonferroni test. The Mann–Whitney U test or the Student’s t-test was used to examine patients’ sex, risk factors, and previous diseases associated with plasma NT-proBNP level as appropriate. The optimal cut-off points of plasma NT-proBNP concentration to discriminate the stroke etiologic subtypes from each other were obtained by receiver operating characteristic (ROC) curves using Youden’s J statistic. Differences were considered statistically significant at a level of p < 0.05. A multi-variable logistic regression model was used to determine whether NT-proBNP concentration was an independent predictive factor of cardioembolic stroke.
Results
In all, 258 patients with acute ischemic stroke were eligible for analysis (mean age = 68.5 ± 11.8 years; range 33–97 years; 133 (51.6%) females). The average interval from symptom of stroke onset to ED arrival was 6.0 h (range: 1–72 h). The median length of hospital stay was 14.0 days (range: 3–35 days). Table 1 shows the baseline characteristics of patients enrolled in this study.
Baseline characteristics.
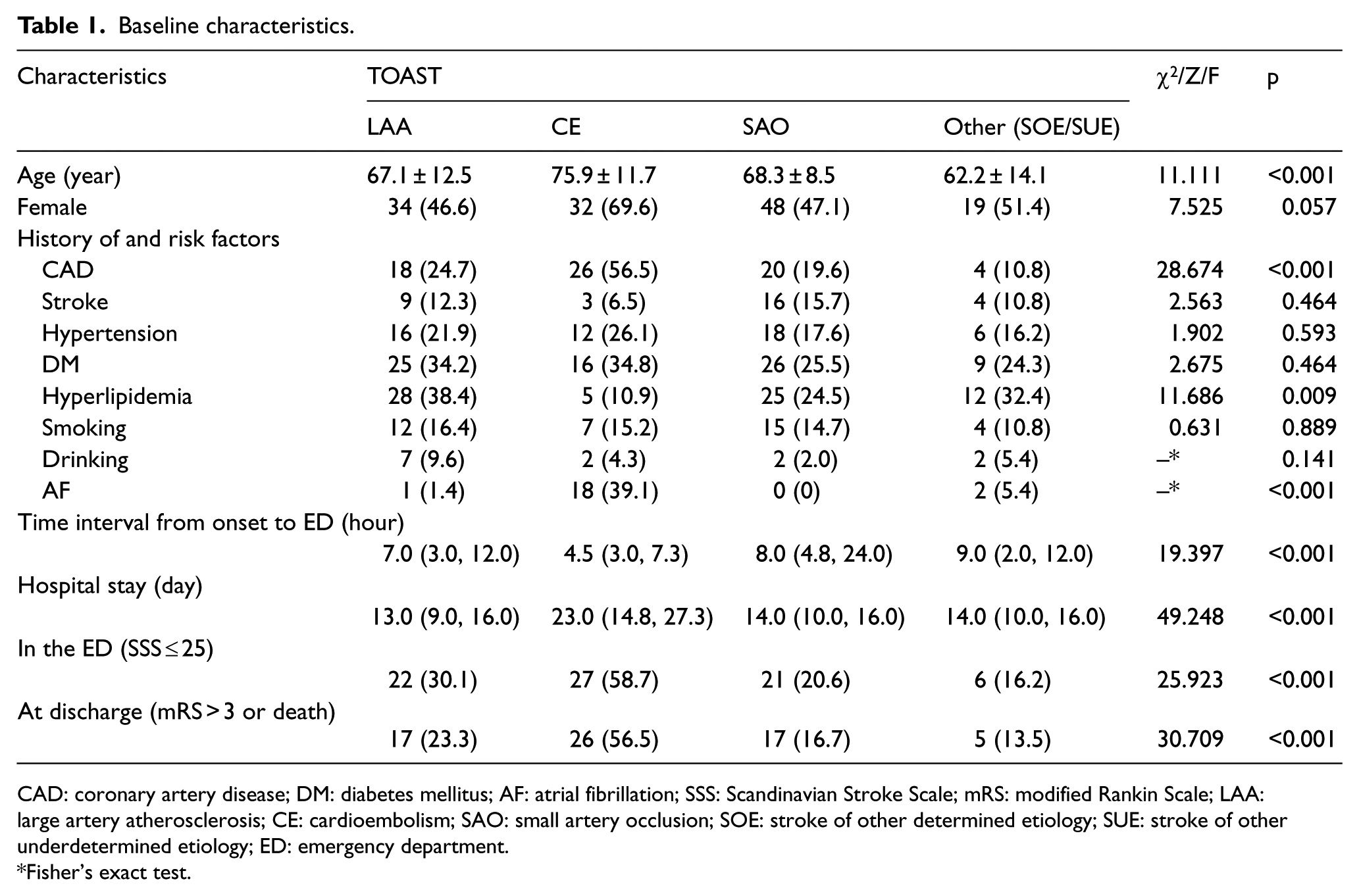
CAD: coronary artery disease; DM: diabetes mellitus; AF: atrial fibrillation; SSS: Scandinavian Stroke Scale; mRS: modified Rankin Scale; LAA: large artery atherosclerosis; CE: cardioembolism; SAO: small artery occlusion; SOE: stroke of other determined etiology; SUE: stroke of other underdetermined etiology; ED: emergency department.
Fisher’s exact test.
Among these 258 patients, 73 (28.3%) were diagnosed with LAA at discharge, 46 (17.9%) with CE, 102 (39.5%) with SAO, and 37 (14.3%) with SOE and SUE (Figure 2). Because there were few cases of patients with SOE and SUE subtypes, we merged them together and labeled it as “OTHER (SOE/SUE)” group. The mean ± standard deviation (SD) of NT-proBNP concentration was 446.6 ± 209.8 pg/mL among the 258 patients. The mean ± SD of NT-proBNP concentration was 690.5 ± 218.3 pg/mL in the CE group, 400.2 ± 167.0 pg/mL in the LAA group, 391.7 ± 181.2 pg/mL in the SAO group, and 386.1 ± 119.2 pg/mL in the other group (Figure 3). The mean NT-proBNP concentration was significantly higher in the CE group than in the other three stroke groups (F = 35.415, p < 0.01). However, there was no statistical significance between the other three groups (Bonferroni test: LAA vs SAO, p = 1.000; LAA vs Other, p = 1.000; SAO vs Other, p = 1.000).
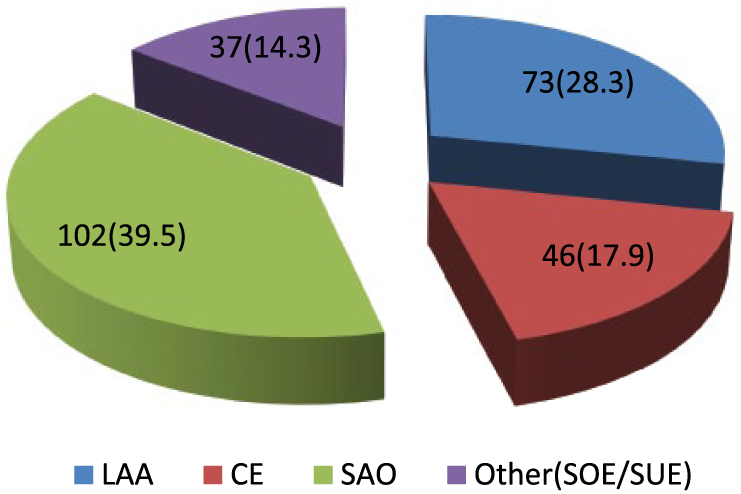
The proportion of the TOAST subtypes in this study (n (%)).
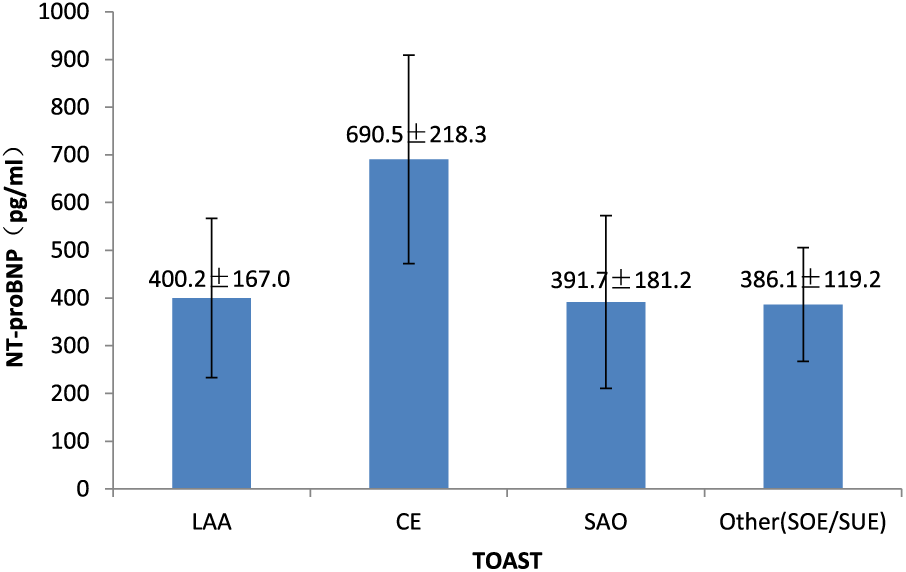
Plasma NT-proBNP levels and the TOAST subtypes.
Age, length of hospital stay, SSS score on arrival less than or equal to 25, and mRS greater than or equal to 3 or death at discharge were all significantly higher in the CE subtype compared to other TOAST subtypes (p < 0.05). In addition, frequency of hyperlipidemia was significantly higher in the LAA patients (χ2 = 11.686; p = 0.009). Frequency of coronary artery disease was significantly higher in the CE patients (χ2 = 28.674; p < 0.01). However, there was no statistical significance for previous stroke, diabetes mellitus, smoking habit, or alcohol use between these four groups (χ2 = 2.563, p = 0.464; χ2 = 2.675, p = 0.444; χ2 = 0.631, p = 0.889 and p = 0.141). AF was diagnosed among 15 (32.6%) of 46 patients with CE (Table 1).
The optimal cut-off values, accuracy, sensitivity, specificity, and the area under the curve (AUC) of the plasma NT-proBNP concentration suitable to distinguish CE from non-CE was as follows: 501.2 pg/mL, 80.6%, 82.6%, 80.2%, and 0.87 (95% confidence interval (CI): 0.83–0.92) in the CE group, respectively (p < 0.001, Figure 4). After adjusting for age, sex, coronary artery disease history, AF history, renal function, and D-dimer concentration, NT-proBNP was found to be independently associated with cardioembolic stroke (p < 0.001). The multi-variable logistic regression model is shown in Table 2.
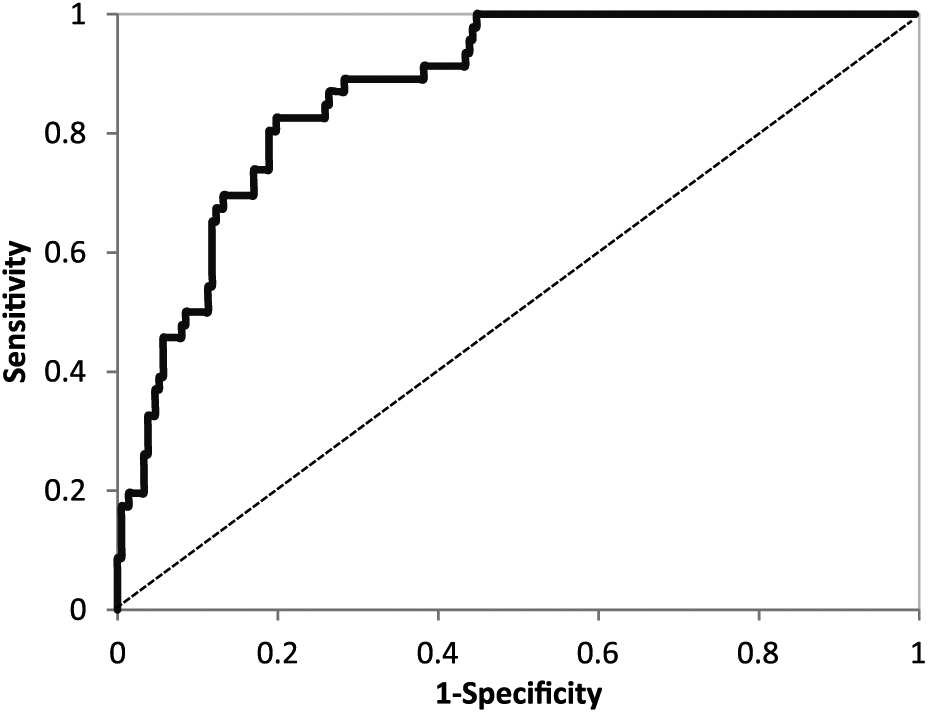
ROC curves of NT-proBNP to distinguish cardioembolism group from the other TOAST subtypes.
Multi-variable predictors of cardioembolic stroke.
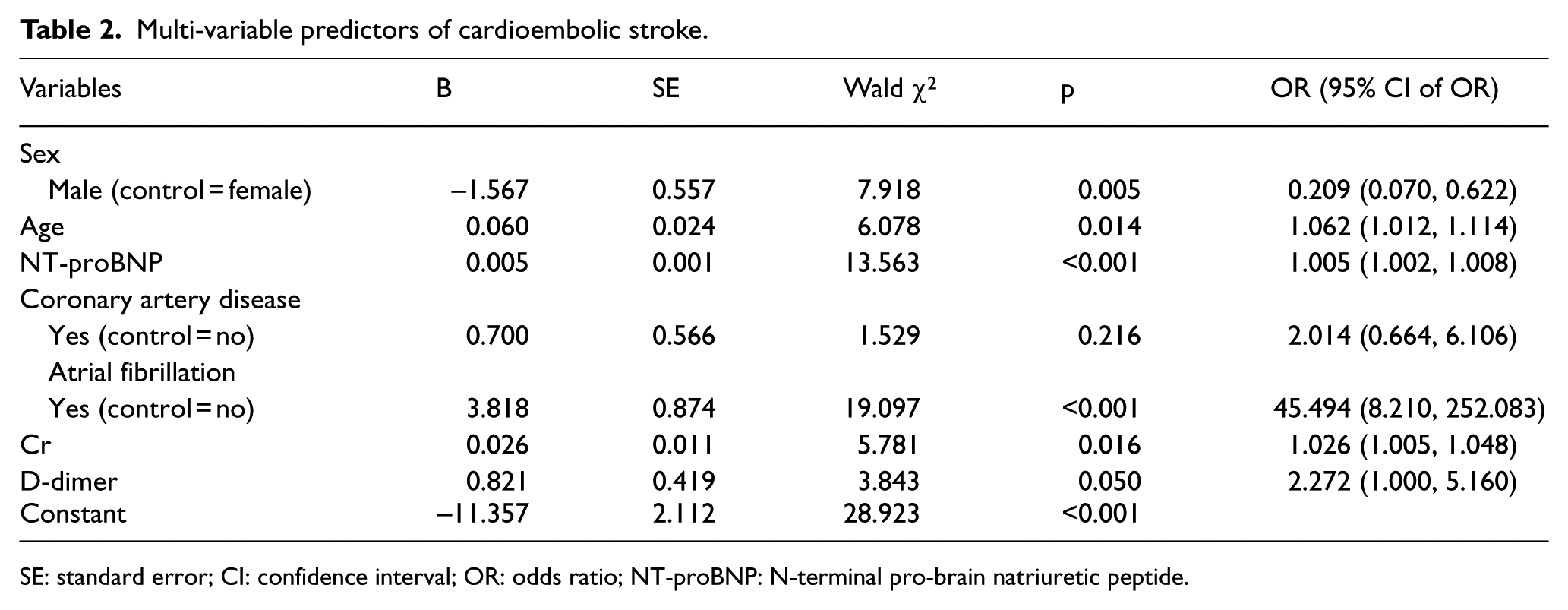
SE: standard error; CI: confidence interval; OR: odds ratio; NT-proBNP: N-terminal pro-brain natriuretic peptide.
Discussion
Acute ischemic stroke is a time-sensitive disease and needs to be evaluated and treated immediately. We already know that an elevated BNP/NT-proBNP level is an independent biomarker for cardioembolic stroke and is associated with unfavorable outcome.7–13,17–24 At present, the use of plasma biomarkers with a POCT platform is increasingly popular in the ED. Emergency physicians can perform a NT-proBNP measurement and obtain the results within 12 min using a POCT platform. To ensure effective and rapid assessment, we set up a new algorithm for suspected stroke patient management with a BNP/NT-proBNP POCT platform in the ED according to the AHA and ASA guidelines.3–5,12,24,25 Based on our clinical experience, initial assessment of the suspected stroke patient can be completed and efficient treatment can occur without delay using this algorithm in the ED.25,26 In our previous study, we found that using Biosite Triage® BNP POCT platform (Triage BNP; Biostie, Inc, San Diego, CA), emergency physicians should strongly consider CE subtype with a plasma BNP level of over 66.50 pg/ml (Se 75.0%; Sp 88.7%) in our ED in Foshan City. 12 This BNP concentration reference index has been validated as having good diagnostic performance in another study. 24 To the best of our knowledge, this is the first study to determine the suitable cut-off value of the NT-proBNP level to distinguish cardioembolic stroke from other TOAST subtypes in a Chinese population.
The results of our study confirm that differences in plasma NT-proBNP might be useful to distinguish cardioembolic stroke from other stroke subtypes. It is sensitive, specific, easy, rapidly processed, inexpensive, and widely available, suggesting that the plasma NT-BNP could be a good stroke biomarker for emergency physicians’ use. In this study, a NT-proBNP concentration of over 501.2 pg/mL can be used to distinguish CE from non-CE in Chinese patients using the Roche Cobas h 232 POCT platform in our EDs (sensitivity 82.6%; specificity 80.2%).
Based on recent published articles and our experience, patient’s clinical grounds, neuroimaging, NT-proBNP level, and other emergency tests are reviewed by an emergency physician and a neurologist together. The suspected cardioembolic stroke patient and the patient with a high risk for paroxysmal AF, poor functional outcome, and in-hospital mortality can be recognized early in the ED.12,21,24,28–30 In addition, several factors correlate with increased NT-proBNP levels, such as left atrial thrombus, heart failure, left atrial dysfunction, angina pectoris, cardiomyopathy, myocardial infarction, pulmonary embolism, and chronic renal failure.12,21,24,28–30 Therefore, if the plasma NT-proBNP level is much higher in the ED, such conditions should be carefully considered, and the related examinations could be preferentially performed after admission. In this study, we found that hyperlipidemia was significantly more common in the LAA patients, while coronary artery disease was significantly more common in the CE patients. However, there was no statistical significance for previous cerebral disease history, diabetes mellitus, smoking habit, or alcohol use between TOAST subtypes which was consistent with our previous studies.12,24 Through this new algorithm for suspected stroke patient management in the ED, emergency physicians are able to improve and accelerate the “stroke chain of survival,” provide more important clinical information for neurologists to rapidly start optimal secondary prevention, and recognize the patient with a high risk of in-hospital mortality.
The optimal cut-off value of the NT-proBNP level to distinguish cardioembolic stroke from other TOAST subtypes varies greatly in recently published studies.17,18,20 There are two main reasons: first, the interval from stroke onset to blood sample collection and testing were significantly different in these studies. Second, the proportion of TOAST subtypes is significantly different among territories due to the difference in regional patient age, nationality, area, race, and traditional diet habit. Hence, further larger multicenter studies including various ethnic groups are required to analyze the suitable levels of NT-proBNP to predict the TOAST subtypes and outcome in stroke management.
The reasons for NT-proBNP elevation in acute stroke patients, particularly in the CE subtype, are still unclear. First, clinical and experimental evidence suggests that stroke is associated with an increase in the plasma catecholamine levels, myocardial damage, and sudden death. Cardiac causes account for most of the deaths in patients with ischemic stroke. Particularly, sympathetic activation is known to cause serious adverse effects on myocardial functions, and in turn, myocardial dysfunction increases the risk of death. Elevated NT-proBNP is indicative of increased sympathetic and renin–angiotensin–aldosterone system (RAAS) activity. Therefore, the use of NT-proBNP level on assessment of cardiovascular function is important in stroke patients. Second, stroke patients have already suffered a congestive heart failure prior to stroke onset, and therefore, NT-proBNP secretion can reflect cardiac dysfunction. Finally, abnormally high NT-proBNP levels might be related to AF, one of the strongest risk factors for ischemic stroke and a known cause of NT-proBNP elevation.31–35
Although both BNP and NT-proBNP levels are thought to be inversely related to renal function, BNP is further cleared by neutral endopeptidases and the natriuretic peptide C receptor. 36 However, several studies have also shown that BNP and NT-proBNP levels are similarly affected in patients with mild and moderate renal dysfunction. 37 In addition, the half-life of NT-proBNP is significantly longer than that of BNP. 38 These differences may contribute to the higher circulating NT-proBNP levels observed in many physiologic and pathologic states. Despite these differences, compared to our previous studies, we found that both BNP and NT-proBNP had similar diagnostic performance in distinguishing the CE subtype from other TOAST subtypes which is consistent with a pooled data meta-analysis.12,18 However, the single BNP/NT-proBNP POCT platform cannot be used to identify the CE subtype as a diagnosis and must be considered in context with clinical assessment and judgment before making treatment decisions in the ED.
Limitations
Despite this being a multicenter study, it was limited by its small size. The classification of stroke subtype according to the TOAST criteria does not have a criterion standard and may be a bias in this study.39,40 We might have missed some patients without signs and symptoms of a stroke. In addition, 12-lead ECG, continuous ECG, and 24-h Holter ECG might have failed to diagnose AF in a small number of patients, and therefore, we may have missed AF in some patients. 24 Further larger multicenter studies including various ethnic groups and different intervals from symptom of stroke onset to ED arrival are required to analyze the optimal levels of NT-proBNP to predict the TOAST subtypes and outcome in stroke management.
Conclusion
NT-proBNP is independently associated with cardioembolic stroke. Through this new algorithm for suspected stroke patient management in the ED using the Roche Cobas h 232 POCT platform, emergency physicians should strongly consider the CE subtype with an NT-proBNP level of over 501.2 pg/mL. However, the single NT-proBNP POCT platform cannot be used to identify CE subtype as a diagnosis and must be considered in context with clinical assessment and judgment before making treatment decisions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the Internal Grants from Science and Technology Foundation of Foshan City, China (no. 2014AB00328, no. 2014AG10002, and no. 2015AB00354), Guangdong Province Science and Technology Foundation (no. 2014A020212002) and the Municipal Clinical Key Specialty Construction Project Funds of Foshan City (No. Fspy2-2015004 and FSGSPZD135016,No.FSGSPZD135018). Pilot project of Guangzhou Clinical Medical Research and Translational Medicine Center (No. 201508020005), the Science and Technology Project of Guangzhou (No.155700027) and the National Clinical Key Specialty Construction Project Funds (No.2012-649).