
Abstract
Background:
Occupational burnout syndrome generally develops in individuals of helping professions and is considered to result from long-standing stress. Burnout syndrome is characterized by loss of interest, fatigue, or frustration, the negative consequences of which affect the individual’s performance, thus being a major factor that influences the quality of work.
Objectives:
The aim of the study was to assess the existence of burnout syndrome in medical staff working at hospital emergency department.
Methods:
The study included 120 subjects working at emergency departments. The following two questionnaires were used: Copenhagen Burnout Inventory and Copenhagen Psychosocial Questionnaire. Likert scale was employed on scoring the answers offered in the questionnaires. Statistical analysis was performed using the exploratory factor analysis, analysis of variance, Bonferroni test, and Pearson correlation coefficient. The level of statistical significance was set at p < 0.05.
Results:
Study results revealed that the subjects suffer mostly from the symptoms of fatigue due to occupational burnout and exhaustion at the end of the day. The prevalence of burnout syndrome was highest among subjects with 11–15 years work in emergency department, while lower risk was recorded in those nurses and physicians who reported a higher level of social support, sense of community, and feedback information.
Conclusion:
Results of the study confirmed the existence of burnout syndrome in medical staff working at hospital emergency department, with the highest prevalence recorded in those working at this department for more than 11 years. The main burnout symptoms reported by study subjects were fatigue, exhaustion at the end of the day, and feeling that they were giving more than they were receiving in return. Burnout syndrome was found to be less common among those nurses and physicians who reported a higher level of social support, sense of community, and feedback information.
Introduction
By definition, burnout syndrome is a state of mental, physical, and emotional exhaustion caused by excessive and prolonged stress, 1 that is, a condition presenting with emotional exhaustion, depersonalization, and feeling of low personal achievement, 2 actually representing a delayed response to various chronic stressful events. Burnout syndrome is characterized by loss of interest, fatigue, and frustration, the negative consequences of which reflect on the individual’s performance and lead to reduced productivity at work. The syndrome generally develops in working environments characterized by workplace uncertainty, lack of proper work control, and occupational safety measures, thus requiring frequent emergency activities, as well as the need to work overtime without week rest and/or annual leave.3,4 Studies have shown the burnout syndrome to occur most frequently in professions that involve social contacts, high level of responsibility, and strenuous work, that is, in helping professions. Healthcare ranks high due to the high medical staff exposure to emotional exhaustion because of the demanding nature of their workplace and low autonomy. Burnout syndrome was first observed in healthcare personnel working in intensive care units (ICUs), surgeons, and psychiatrists, later also in other medical professions.5–9 The occurrence of burnout syndrome in emergency department (ED) personnel poses a special problem. Literature data point to the high prevalence of burnout syndrome in ED personnel.9,10 Physicians working in ED are at a threefold greater exposure to burnout syndrome as compared to other physicians or any other employee working in medical profession or elsewhere. A study that included 7288 physicians revealed more than 65% of those working in ED to suffer from burnout syndrome versus 55% of internists and 27.8% of the general population of employees working in other services. 9 In Croatia, burnout syndrome has also been recorded in ICU personnel 6 and in those working with dying patients, 11 whereas there are no published data on the issue in ED personnel. In 2008, the government of the Republic of Croatia launched a project of the national emergency medicine service (EMS) restructuring, supported by the World Health Organization loan, whereby integrated hospital EDs have been established instead of previous specialty-based EDs, thus generating a new group of health personnel exposed to a high risk of developing burnout syndrome due to workplace change and taking over a number of new activities and responsibilities.
The aim of the study was to assess the presence of burnout syndrome in healthcare personnel working in the newly established hospital EDs.
Subjects and methods
We have surveyed a total of 127 emergency medical workers with Copenhagen Burnout Inventory (CBI) and Copenhagen Psychosocial Questionnaire (COPSOQ II) instrument receiving 120 valid surveys (94.48% response). The study included 120 subjects, that is, 59 nurses/medical technicians and 61 physicians, working in three hospital EDs in Croatia (Emergency Department, Sveti Duh University Hospital, Zagreb; Emergency Department, Sestre milosrdnice University Hospital Center, Zagreb; and Emergency Department, Karlovac General Hospital, Karlovac). The study was conducted using anonymous questionnaires, with voluntary participation of the study subjects. The study was approved by the respective hospital Ethics Committees and was performed in line with ethical principles and human rights in research. Study subjects were administered two questionnaires: CBI and COPSOQ II. The former questionnaire on burnout at workplace (CBI) is a specific instrument developed by the National Institute of Occupational Health from Copenhagen in 2005, 12 intended for assessment of personal and occupational burnout, as well as burnout caused by working with patients. The questionnaire consists of 18 questions with five to seven possible answers distributed in three sections related to personal burnout (5 questions), occupational burnout (7 questions), and burnout caused by working with patients (6 questions). The personal burnout defines the burnout level of an individual according to his or her job and work overload including exhaustion and decrease in emotional energy. The occupational burnout assesses the degree to which an individual responds emotionally to works, and burnout caused by working with patients assesses the degree of physical and psychological exhaustion which is perceived by the person as related to work with patients. The reliability coefficients of the CBI (internal consistency coefficient, Cronbach alpha values) were calculated and found that was excellent for the entire questionnaire (0.931), as well as for individual factors of personal and occupational burnout (0.921) and of burnout in work with patients (0.866).
The COPSOQ II is used as a tool for assessment of psychosocial conditions related to work, health, and well-being. The questionnaire was developed by the Danish National Research Centre for the Working Environment from Copenhagen in 2000 and revised in 2005. 13 It contains assessment of social support (two questions), social inclusiveness (three questions), and feedback at workplace (three questions).
Participants were asked to rate the frequency of experiencing each stressor. Each stressor was written as a question such as “Do you feel exhausted at end of the day?” or “Are you tired of working with patients?” The question is answered in terms of how often the respondents experience these feelings and scored on Likert scale according to answer category as follows: always—100, frequently—75, occasionally—50, rarely—25, and never/almost never—0. Data collection process took approximately 30 days from questionnaire distribution to collection. A high overall score denotes a considerable level of burnout syndrome.
The data obtained were expressed as percentage in case of categorical variables and as arithmetic mean and standard deviation in case of continuous variables. The exploratory factor analysis using the principal component technique was done to assess factor structure of the questionnaires employed (CBI and COPSOQ II). Difference in the level of burnout syndrome according to years of service and years of work in hospital ED was calculated using analysis of variance; in case of a significant F ratio, post hoc Bonferroni test was employed to identify statistically significant between-group differences. Pearson coefficient of correlation was used to assess the association of burnout syndrome with interpersonal relations and relations with superiors at workplace.
Results
The study included 120 subjects, that is, 59 (49.2%) nurses/medical technicians and 61 (50.8%) physicians. Demographic data revealed the greatest number of study subjects to be in the 26–35 age group (n = 57), followed by the 36–45 age group (n = 36), and the least number of those in the 18–25 and 56–65 age groups (n = 12 both) (Table 1). In all, 50 of 59 nurses/medical technicians had high school education, 8 had univ. bacc. nursing/med. techn. degree, and 1 had MS degree in nursing; 28 of 61 physicians were specialists and 33 were residents. Due to the small number of subjects with 16–20 and >20 years of work in ED, on further data processing, this variable was re-coded to the group with >16 years of service, yielding 24 subjects.
Demographic characteristics of study subjects.
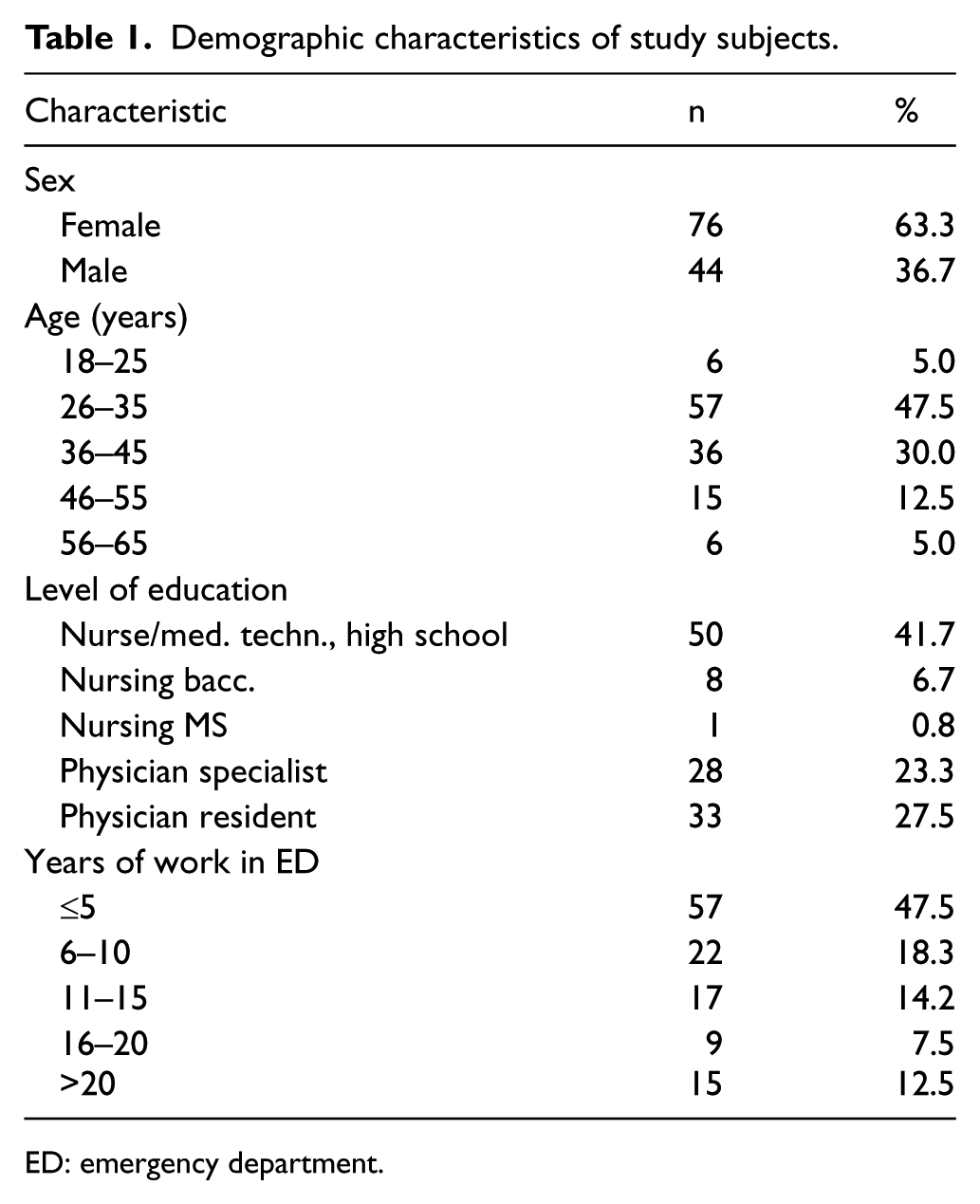
ED: emergency department.
Table 2 shows answers related to occupational burnout, unifying personal and occupational burnout, as well as burnout consequential to work with patients. In the group of questions related to personal burnout, the majority of subjects answered they frequently felt tired (50%) and physically exhausted (45.8%). In the group of questions related to emotional exhaustion, the majority of subjects answered that they felt exhausted occasionally or frequently (70%), whereas 41 (34.2%) subjects stated that they occasionally could not stand emotional exhaustion. Answers in the group of questions related to occupational burnout revealed that the majority of study subjects (42.5%) frequently felt emotionally exhausted. Most of them (43.3%) felt exhausted at the end of the day, whereas morning exhaustion was reported by 58 subjects. In the group of questions on burnout related to work with patients, 51.7% of study subjects considered that it was difficult to work with patients occasionally. Most subjects (40.8%) stated that they were occasionally frustrated by working with patients, and fatigue was reported by 65 (54.2%) subjects. About 43 (35.8%) subjects felt that they were occasionally giving more than receiving in return.
Analysis of the questionnaire on occupational burnout.
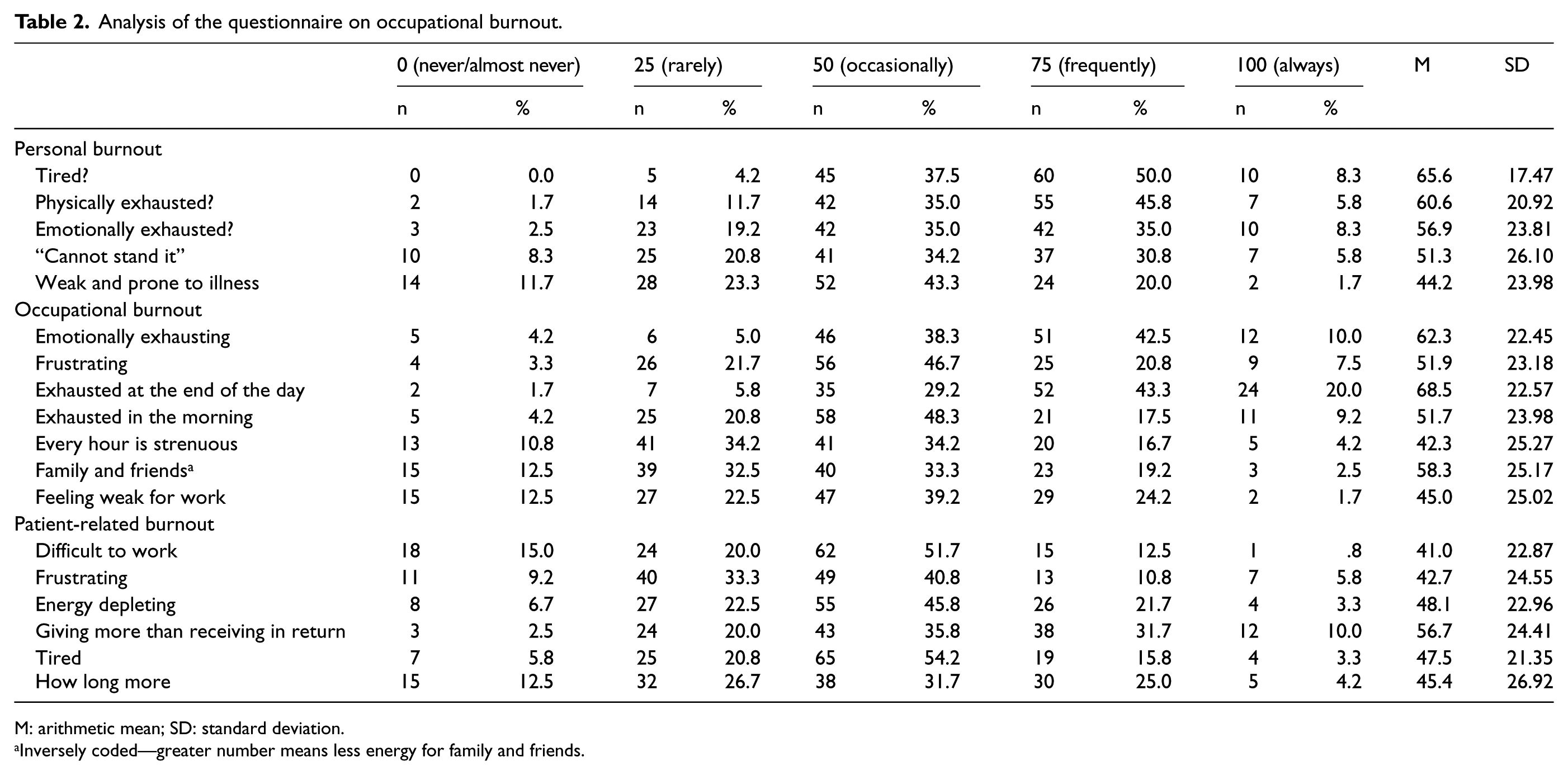
M: arithmetic mean; SD: standard deviation.
Inversely coded—greater number means less energy for family and friends.
As shown in Table 2, arithmetic means of answers recorded in the questionnaire on personal and occupational burnout and those in the questionnaire on the relationship with patients yielded a score greater than 40 for all types of burnout. Study subjects mostly stated that they felt tired (65.6) and exhausted at the end of the day (68.5). Considering their relationship with patients, the highest score referred to their feeling of giving more than receiving in return (56.7).
Data presented in Table 3 illustrate analysis of differences in personal and occupational burnout according to age, sex, workplace, and years of work in ED. The level of burnout differed only according to the years of work in ED (p = 0.001). Bonferroni test yielded a statistically significant difference between the subjects with ≤5 years of work in ED and those with 11–15 years (p = 0.009) and >16 years (p = 0.006) of work in ED. The subjects with ≤5 years of work in ED manifested a lower level of burnout than those with >11 years of work in ED.
Analysis of differences in personal and occupational burnout according to demographic variables.
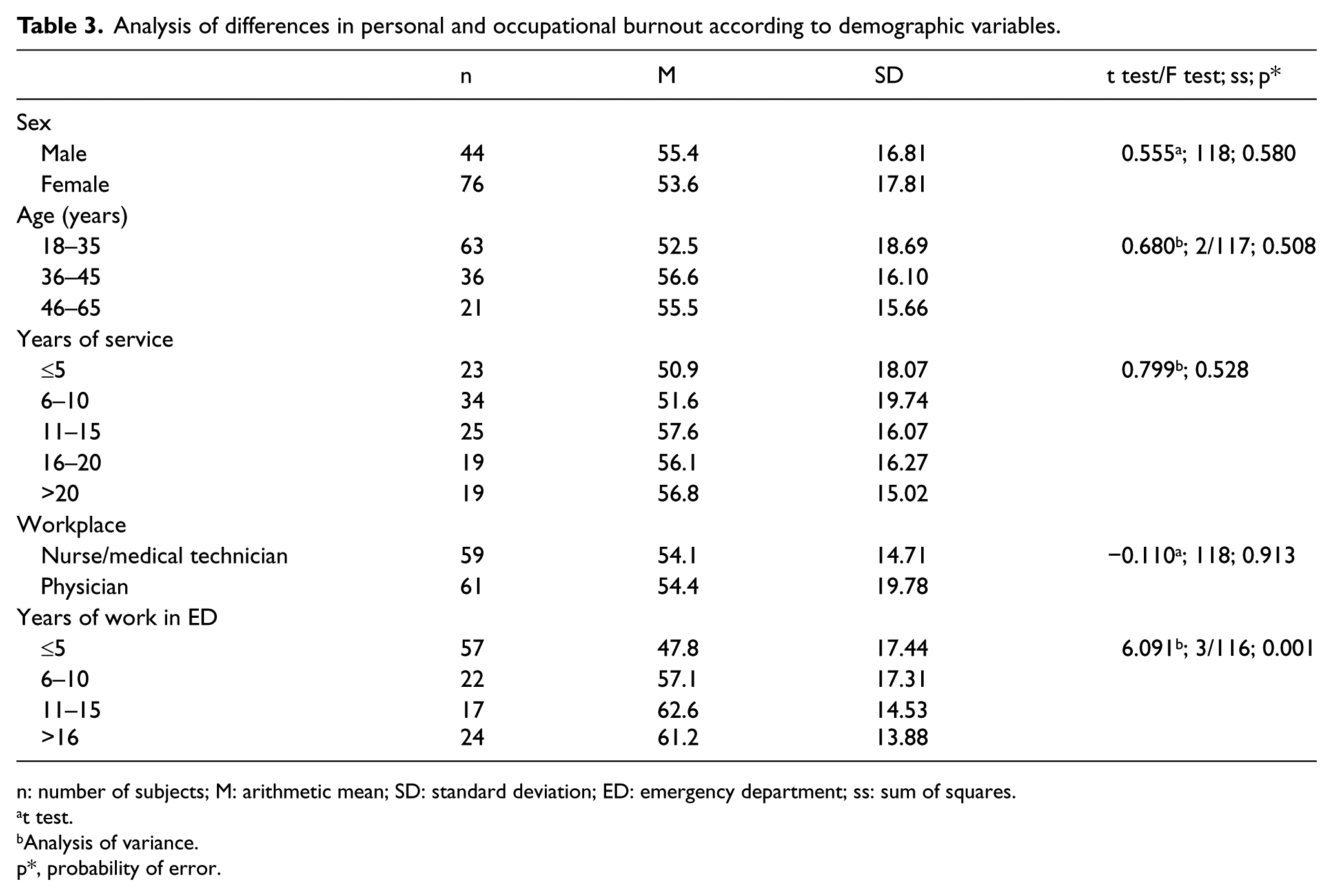
n: number of subjects; M: arithmetic mean; SD: standard deviation; ED: emergency department; ss: sum of squares.
t test.
Analysis of variance.
p*, probability of error.
Table 4 shows differences in burnout related to work with patients according to age, sex, years of service, workplace, and years of work in ED. The level of burnout differed only according to the years of work in ED (p = 0.028), while statistical significance was only found between the subjects with ≤5 and those with 11–15 years of service (p = 0.054).
Analysis of differences in burnout related to work with patients according to demographic variables.
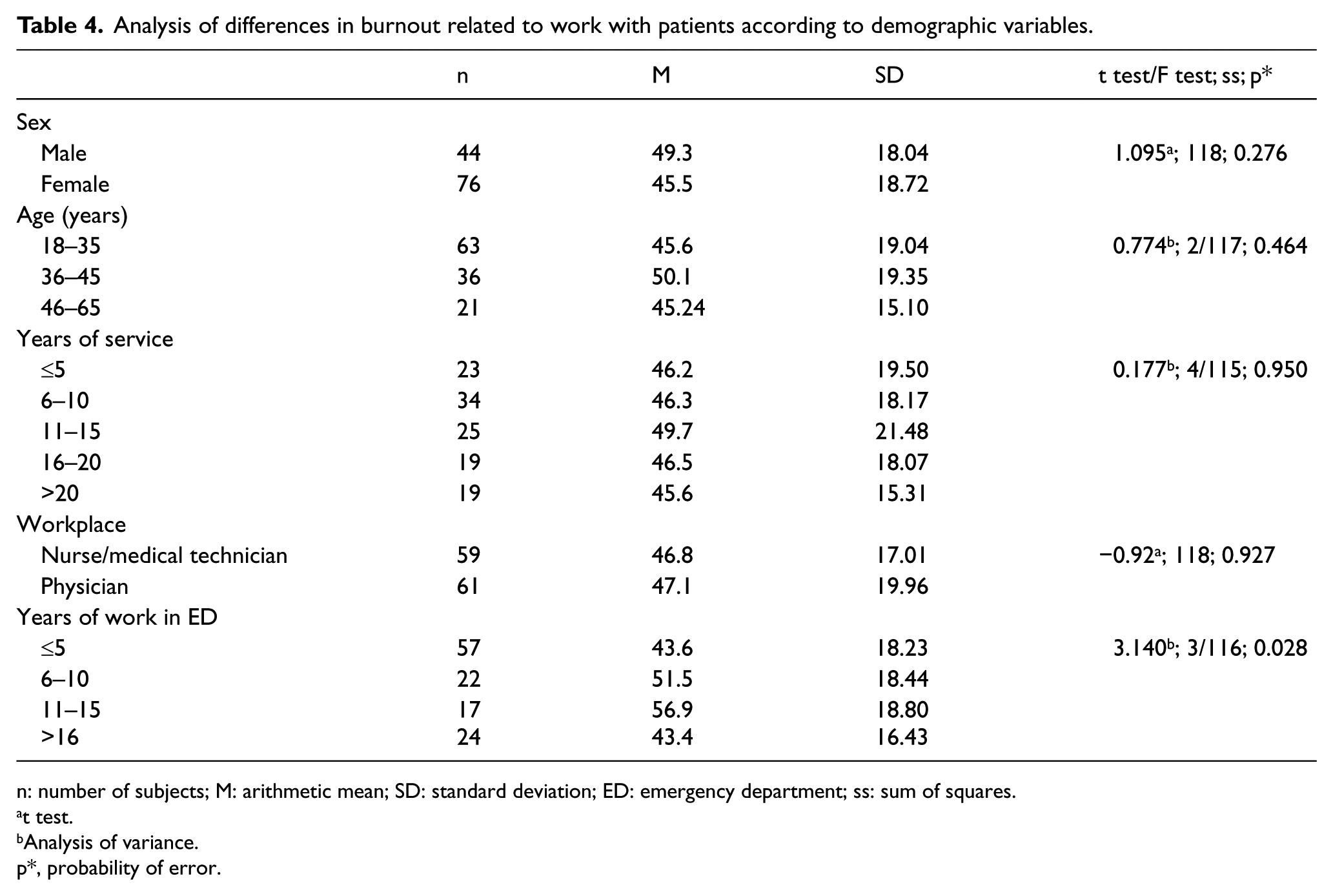
n: number of subjects; M: arithmetic mean; SD: standard deviation; ED: emergency department; ss: sum of squares.
t test.
Analysis of variance.
p*, probability of error.
As shown in Table 5, in the group of questions on social support, 86 subjects felt that their co-workers offered them support and assistance frequently. Support from their superiors was reported by 78 subjects. Considering the question on the sense of community, that is, on the atmosphere at their workplace, 62 subjects described it as usually good, and 77 subjects felt being part of the community.
Results on social support, feedback information, and sense of community.
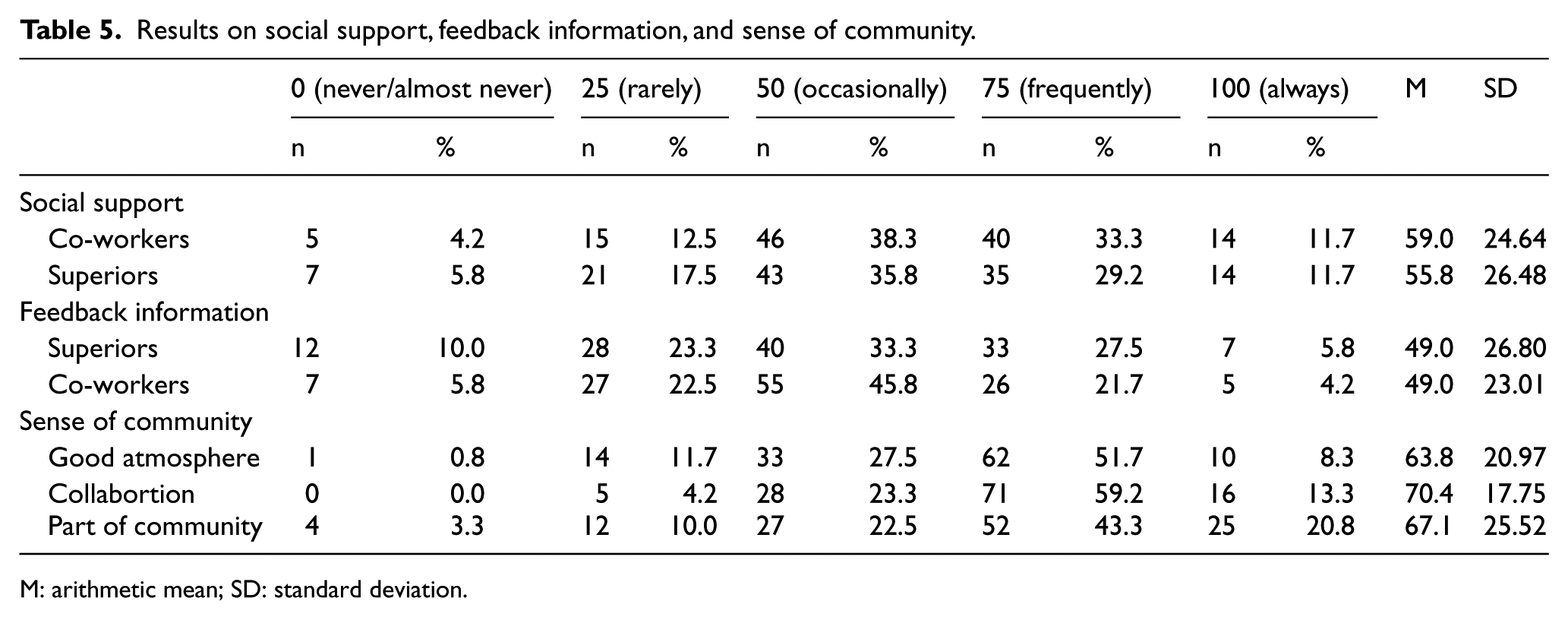
M: arithmetic mean; SD: standard deviation.
Table 6 illustrates correlation of personal and occupational burnout and burnout related to work with patients with the variables of social support, feedback information, and sense of community. The subjects showing a higher level of personal and occupational burnout reported a lower level of social support, less feedback information received, and lower sense of community. The subjects manifesting a higher level of burnout related to work with patients also reported a lower level of social support and lower sense of community. These correlations were statistically significant (p < 0.001).
Correlation of personal and occupational burnout and burnout related to work with patients with social support, feedback information, and sense of community.
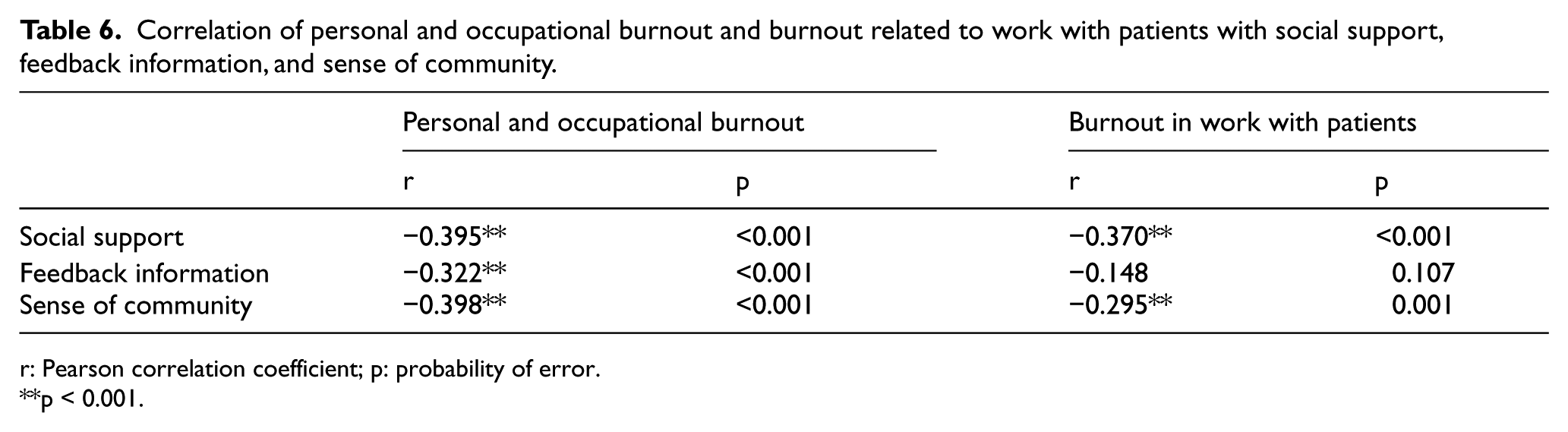
r: Pearson correlation coefficient; p: probability of error.
p < 0.001.
Discussion
This study examined the factors of personal and occupational burnout syndrome in nurses/medical technicians and physicians working in hospital ED in relation to their work with patients and of burnout related to interpersonal relationships, social support, and relationship with their superiors. Analysis of socio-demographic data showed female subjects to prevail in the study group, which is consistent with the higher proportion of women in healthcare service in Croatia. According to data from 2012, there were 7245 nurses/medical technicians (6570 of them were female) and 4153 physicians (2480 of them were female) employed in healthcare institutions in the city of Zagreb, the capital of Croatia. 14
Data obtained from study subjects on personal burnout point to increased fatigue, physical and emotional exhaustion, and proneness to illness. Most of these subjects had >11 years of work in ED. This information indicates that long-standing exposure to mental and physical strain, chronic stressors, and professional responsibility breaks the protective mechanisms and adjustability; with long-standing exposure to stress, the power of stress reactions is also transferred to the somatic level, resulting in proneness to diseases and an increased risk of developing burnout syndrome. In the study by Goldberg et al., 15 the length of service and age were not significant factors for burnout syndrome despite the high prevalence of this syndrome in ED physicians, whereas our study results pointed to the length of work in ED as one of the significant factors contributing to the development of burnout syndrome. These results could be related to organizational problems in medical personnel working hours, which generally arise due to shortage of medical staff, uneven distribution of working hours, and unplanned sick leaves for occupational diseases.
Schaufeli 16 compared the prevalence of burnout syndrome between physicians and nurses. The results showed physicians to be at a higher exposure to burnout syndrome because of higher psychological and emotional demands, while having low social support at work. We did not find higher prevalence of burnout syndrome in ED physicians as compared with ED nurses, which can be in part explained by the organization of work in EDs in Croatia. Namely, formal education of specialists in emergency medicine has been introduced for only several years now, so that physicians of various specialties (internists, surgeons, neurologists, anesthesiologists, and others) currently work in EDs. They generally are on duty in EDs 4–6 times a month and spend the rest of working hours doing some other jobs; that is, they are not constant members of ED teams. Unlike physicians, nurses are regular members of ED teams. Because of such a structure and distribution of work in ED, where physicians are not continuously exposed to ED stress despite the higher level of responsibility and emotionally more demanding work, their level of stress exposure does not exceed the level of stress in nurses.
Burnout syndrome is known to manifest with signs of emotional exhaustion, that is, weakness, irritability, pain, and insomnia, which in turn renders medical worker hard-hearted, insensitive for problems of the others, losing interest in his or her job, and assuming inappropriate behavior with patients. 17 In our study, emotional exhaustion also stood out as the most significant burnout symptom. As many as 70% of our study subjects felt exhausted occasionally or frequently, while more than 30% of subjects reported frequent sense that they could not stand such emotional exhaustion much longer. Stechmiller and Yarandi analyzed data collected on 300 nurses employed at nine hospitals full-time for at least 3 months. Their results showed progression of stress and emotional exhaustion, while satisfaction with job influenced their emotional exhaustion significantly. 18 In our study, analysis of data on occupational burnout revealed that subjects generally felt exhausted at the end of the day, were frustrated from work, occasionally did not have enough time for family and friends, and considered that work exhausted them emotionally. The highest prevalence of burnout syndrome was also recorded in the subjects with >11 years of ED service.
A study conducted in Croatia in 2014 11 found 64.7% of nurses/medical technicians to have psychological symptoms of fatigue, 29.4% felt emotionally dull, 34.3% were frustrated, and 46.1% did not have enough free time. Symptoms of emotional exhaustion were reported by 88.2% of subjects working with dying patients. Our study subjects also showed severe emotional exhaustion and frustration, and thus a higher prevalence of burnout syndrome, although trying to save as much time as possible for their families and friends. Such a high prevalence of burnout syndrome indirectly points to inadequate familiarity of medical personnel with the problem and thus its late recognition. The symptoms like headache, insomnia, early waking, night waking, and problems with falling asleep usually tend to be related to weather conditions, spine problems, and various private life situations but not with occupational burnout. That is why in our study, burnout syndrome was most common in medical staff working in ED for years. Occupational burnout can be associated with inappropriate working premises and poor working conditions, inappropriate working supplies, and inadequate wages. Performance and health of medical staff are influenced by shift work, high level of responsibility in ED staff members throughout working hours, poor organization of the working process, lack of communication among staff members, inadequate number of staff members, frequent interpersonal conflicts, and so on. Quite frequently, burnout syndrome is not just a problem of an individual but is usually workplace related. 19
Burnout syndrome was also recorded in the work with patients. Our study subjects stated that it was difficult and frustrating to work with patients, to feel exhausted and tired. The greatest proportion of study subjects reported that they were giving more than receiving in return in their work with patients. Because of the great number of critical patients, working in ED requires high concentration and simultaneous care for several patients at the time and rapid decision-making, frequently with inadequate information available. Following complete patient workup and hospitalization, due to the shortage of time and great bulk of work, medical staff usually cannot receive subsequent information on patient health condition and therapeutic outcome. Thus, medical workers are deprived of receiving confirmation of their work and the feeling of success.
Considering social support in the form of assistance and support from co-workers and superiors, our study results indicated most of the study subjects to feel they had support and assistance from their co-workers, and consequentially they had the sense of belonging to the community. However, their superiors appeared to be less willing to provide support to their subordinates. The same held true for feedback information, which frequently failed to be communicated not only by the superiors but also by the co-workers. The data obtained in the study point to the importance of good interpersonal relationships and the role of superiors in creating a good working atmosphere. With their knowledge, professionalism, competences, and organizational capacity, the superiors greatly influence social support. Good communication and collaboration reduce the level of adverse stress effects on the work process and thus on the workers themselves. Workers should be educated on the importance of communication and superiors on the need to appreciate, as well as criticize particular procedures or events. Every appreciation, suggestion, advice, and assistance is highly relevant in the work process, while considerably reducing the level of burnout syndrome. Satisfaction of the staff will be higher if they receive appreciation from their superiors more frequently, if their superiors follow their work, have established an open dialogue with them, and if they have good relationships with their co-workers, thus creating a pleasant social environment. The workers whose personality, knowledge, and competences correspond to the needs posed by the workplace have a higher level of satisfaction at work.
The risk of burnout syndrome is increased by a number of factors, for example, disproportion of responsibilities and authorities; ill-defined work distribution and system of superiors; inadequate day breaks and week rest; lack of the sense of community, commitment to team and organization; lack of confidence; suspiciousness; inhibiting independence and creativity; uncertainty; competitiveness; autocratic and centralized management; inability to express opinions and to influence decision-making; and inadequate feedback information. 17 Comparison of these findings with our study results revealed that the level of burnout syndrome was lower in those subjects who reported positive collaboration, good atmosphere at work, and sense of community.
In conclusion, results of our study showed the burnout syndrome to be present in ED staff members, in particular in those working in ED for more than 11 years. The predominating symptoms of burnout syndrome were fatigue and exhaustion at the end of the day, lack of feedback information from co-workers and superiors, and feeling that they were giving more than receiving in return. The ED staff members were aware of the need to develop the sense of community and of the importance of social support from co-workers and superiors. The level of burnout syndrome was lower just in those nurses and physicians who reported a higher level of social support, sense of community, and feedback information.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.