
Abstract
Purpose
Adjacent segment disease (ASD) is a recognized complication following lumbar fusion, characterized by new symptomatic and radiological degeneration at levels adjacent to the fused segment. While revision decompression with extended fusion has traditionally been performed, minimally invasive fusion-sparing strategies such as unilateral biportal endoscopic (UBE) decompression have gained attention. High-level evidence regarding their effectiveness in carefully selected stable ASD remains limited.
Methods
This retrospective cohort study included 17 consecutive patients with clinically and radiologically confirmed ASD treated with isolated UBE posterior decompression between 2022 and 2025. Patients with radiographic instability requiring fusion were excluded. Clinical outcomes included Visual Analog Scale (VAS) scores for back and leg pain, Oswestry Disability Index (ODI), and walking capacity assessed by the self-paced walking test (SPWT). Radiological evaluation included MRI-based canal measurements and standing lateral radiographs assessing segmental kyphosis and sagittal alignment. Pre–post comparisons were performed using paired statistical analyses.
Results
Median age was 66 years (IQR 64–70). Significant postoperative improvements were observed in SPWT distance and duration (p < 0.001), VAS-back and VAS-leg scores (p < 0.001), and ODI (p < 0.001). MRI demonstrated significant enlargement of canal dimensions at the ASD level (p < 0.001). Segmental kyphosis improved modestly without deterioration of global sagittal balance. Two perioperative complications (one dural tear, one epidural hematoma) were managed successfully without permanent neurological deficit.
Conclusion
In carefully selected patients with stable ASD, UBE posterior decompression provides meaningful pain relief, functional improvement, and effective neural decompression while preserving sagittal alignment. This tissue-sparing approach may be considered a treatment option in selected high-risk or elderly patients.
Level of evidence
IV.
Keywords
Introduction
Lumbar fusion is one of the most commonly performed surgical procedures for the treatment of degenerative lumbar spine disorders; however, the biomechanical alterations resulting from intersegmental immobilization may lead to increased loading, shear forces, and hypermobility in adjacent motion segments, thereby accelerating degenerative processes over time.1–5 This phenomenon may give rise to the clinical entity known as adjacent segment disease (ASD), which is characterized by the development of new clinical symptoms accompanied by radiological deterioration at segments adjacent to the fused level. 1 Meta-regression analyses have reported an annual incidence of ASD of approximately 2%, while radiological degeneration has been observed at a rate of 6% per year.1,6
The primary goal of ASD treatment is to relieve newly developed neural compression and to stabilize the segment if associated instability is present. Traditionally, posterior revision decompression combined with extended fusion has been employed; however, due to high morbidity, increased blood loss, and prolonged recovery times, these approaches are increasingly reserved for more limited patient populations. 1 With the growing adoption of minimally invasive techniques, endoscopic decompression has emerged as a more physiological alternative for ASD treatment, aiming to relieve stenosis without adding further fusion.7–12
The historical development of spinal endoscopy originated from the adaptation of arthroscopic technologies to spinal surgery. In contemporary practice, biportal endoscopic surgery (UBE) has become widely utilized for posterior decompression due to its simultaneous dual-portal configuration, high-resolution visualization, continuous saline irrigation, and wider working angles.13–18 The principal advantages of UBE include reduced soft-tissue damage, preservation of multifidus muscle integrity, wide-angle visualization of the spinal canal and lateral recess, shorter hospital stays, and lower complication rates.7,19–22 By allowing effective neural decompression without the need for an anterior approach, UBE offers a viable treatment alternative for selected patients with stable ASD, obviating the necessity for additional fusion. 23 Nevertheless, as fusion may still be required in the presence of instability, careful subgroup selection remains a critical component of minimally invasive surgical decision-making. 7 The literature on minimally invasive treatment strategies, particularly UBE decompression for ASD, remains limited. Most available studies are based on small sample sizes, retrospective designs, and heterogeneous patient populations, with a lack of standardized data regarding technical details, indication thresholds, and complication profiles.7,23,24 While UBE has been proposed as a potential fusion-sparing option in stable ASD, high-level evidence regarding clinical outcomes, surgical success, complication rates are still lacking.
The aim of the present study was to evaluate the clinical outcomes, safety profile of UBE decompression in the treatment of ASD following lumbar fusion, and to help address this gap in the existing literature by further clarifying the role of UBE in ASD management.
Materials and methods
This study is a retrospective cohort analysis of patients who underwent biportal endoscopic (UBE) decompression at a single tertiary center between 2022 and 2025. Data were obtained from electronic medical records, operative reports, and imaging archives. Patients with a history of lumbar decompression or fusion surgery who subsequently developed clinically and radiologically confirmed adjacent segment disease (ASD) and were treated with UBE decompression were included in the study. A minimum follow-up duration of 12 months was required for inclusion in the study to ensure adequate assessment of clinical and radiological outcomes.
Radiographic grading of adjacent segment degeneration based on disc height loss, osteophyte formation, and endplate changes.

MRI-based grading of adjacent segment disc degeneration using the Pfirrmann classification.

All procedures were performed by the same surgical team in accordance with standardized two-portal UBE principles. Targeted decompression of the central canal (Figure 1), lateral recess and when indicated, the foraminal region was achieved, while multifidus muscle dissection was minimized and posterior elements were preserved as much as possible. During follow-up, clinical improvement, pain scores, functional parameters, and complications were routinely recorded during standard clinical care and retrospectively analyzed. A patient with adjacent segment disease at L2–3 level treated with unilateral biportal endoscopy (UBE). Preoperative X-ray (a), preoperative sagittal MRI (b), and preoperative axial MRI (c) showing the pathology at the L2–3 level. Postoperative axial CT scan (d) and postoperative axial MRI (e) at the operated level demonstrating adequate decompression.
The primary outcome was defined as the change in functional capacity, assessed using the Self-Paced Walking Test (SPWT) and supported by changes in the Oswestry Disability Index (ODI). SPWT performance was recorded in meters and seconds, reflecting walking distance and duration under standardized conditions. Secondary outcomes included changes in pain intensity measured by the Visual Analog Scale (VAS) for back and leg pain; radiological parameters, including pre- and postoperative canal dimensions and segmental alignment at the ASD level; and perioperative outcomes such as complication rates (dural tear, infection, neurological deficit), need for reoperation, and evidence of postoperative instability. In addition, clinical meaningfulness was assessed using established MCID thresholds for VAS and ODI.28,29 All radiological measurements were performed using the institutional PACS system (Picture Archiving and Communication System). Measurements were obtained by a single experienced observer using standardized digital measurement tools, including angle and distance functions within the PACS software. Each parameter was measured in a consistent manner using predefined anatomical landmarks to ensure measurement uniformity.
Statistical analyses were performed using Python (version 3.12) with standard scientific libraries for data analysis and statistical testing. Continuous variables were summarized as median with interquartile range (IQR), given the small sample size and the non-normal distribution observed in several parameters. Categorical variables were presented as frequencies and percentages. Data distribution was assessed using the Shapiro–Wilk test in combination with graphical inspection. Preoperative and postoperative comparisons were conducted using paired t-tests for variables showing normal distribution and Wilcoxon signed-rank tests for non-normally distributed variables. All statistical tests were two-tailed. Given the exploratory nature of the study and the limited sample size, analyses were primarily focused on within group pre–post comparisons. Statistical significance was defined as p < 0.05. Given the retrospective design of the study, no a priori sample size calculation was performed. To provide additional context for the observed changes, a post hoc power analysis was performed using effect sizes derived from paired comparisons. Furthermore, effect size estimates (Cohen’s dz) were calculated for all variables to complement significance testing and to better characterize the magnitude of the observed changes.
Results
A total of 17 patients were included in the study, comprising 4 males and 13 females. The median age of the cohort was 66 years (IQR: 64–70). Adjacent segment disease involved a single spinal level in 14 patients, whereas multilevel adjacent segment involvement was observed in 3 patients.
Preoperative and postoperative comparisons of clinical, laboratory, and radiological parameters (effect sizes are reported as Cohen’s dz for paired comparisons).
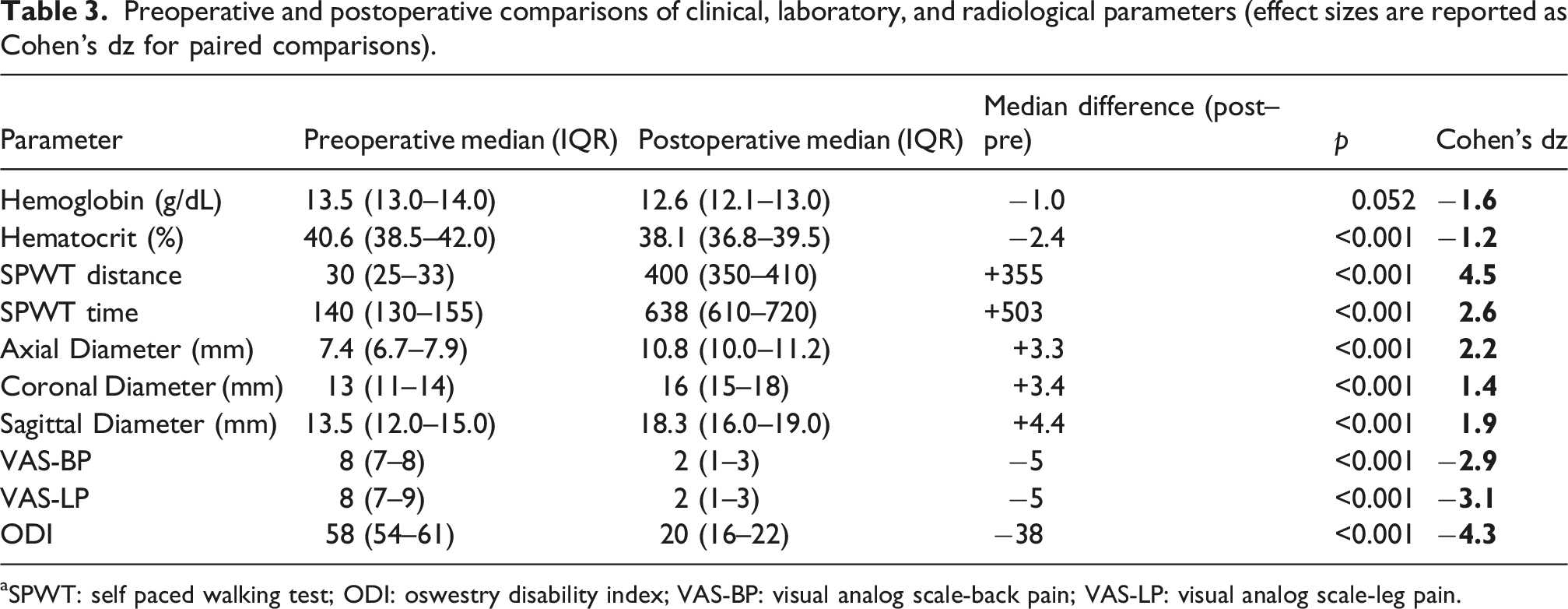
aSPWT: self paced walking test; ODI: oswestry disability index; VAS-BP: visual analog scale-back pain; VAS-LP: visual analog scale-leg pain.

Intraoperative view of a 4 mm dural tear in a patient undergoing unilateral biportal endoscopy (UBE) for adjacent segment disease.

Intraoperative findings of a patient who required revision surgery due to a postoperative epidural hematoma. Intraoperative view showing the epidural hematoma compressing the dura (a). The surgical field after complete evacuation of the hematoma, revealing the decompressed dura (b).
Sagittal alignment was evaluated on standing lateral radiographs with segmental kyphosis at the adjacent segment level. Postoperatively, segmental kyphosis at the ASD level improved from a median of 3.9° (IQR: 3.4–4.3) preoperatively to 3.4° (IQR: 3.1–3.8) at follow-up (p < 0.001). Global sagittal balance, as assessed by SVA, was preserved, with no patient demonstrating progression toward sagittal imbalance. In parallel with these radiographic changes, a consistent clinical improvement in standing and walking posture was observed. Patients who presented with a forward-flexed posture preoperatively were able to ambulate in a more upright alignment following surgery. Importantly, this postural improvement occurred without radiographic evidence of newly developed sagittal imbalance or segmental instability during the postoperative period.
Discussion
This study evaluated the clinical, functional, and radiological outcomes of biportal endoscopic (UBE) posterior decompression in the treatment of adjacent segment disease (ASD) developing after lumbar fusion. The findings demonstrate that, in carefully selected patients with stable ASD, UBE decompression without additional fusion resulted in significant improvements in pain and functional status, accompanied by marked increases in walking tolerance and effective canal enlargement on MRI. These results suggest that ASD should not be viewed solely as an inevitably progressive biomechanical complication, but rather as a clinical entity that can be managed with a targeted and tissue-preserving surgical strategy when appropriate patient selection is applied.1,7,24,30,31 However, it should be emphasized that current evidence regarding the use of UBE in ASD remains limited and heterogeneous, with most available studies consisting of small retrospective series and variable patient selection criteria.
The primary objective of ASD treatment is not merely radiographic decompression but the relief of neural compression while avoiding further iatrogenic destabilization.1,7,24,31 Endoscopic and biportal decompression techniques have been proposed as advantageous in this context, as they better preserve posterior elements and paraspinal musculature, thereby offering a more physiological alternative for selected cases of stable ASD.7,24,30–37 One of the most debated issues in ASD management is whether decompression alone is sufficient in stable cases or whether extension of fusion is ultimately unavoidable. Given the heterogeneous mechanisms underlying ASD, a uniform surgical strategy is unlikely to be optimal for all patients. Increasing evidence supports a stability-based approach, emphasizing meticulous patient selection rather than a one-size-fits-all philosophy.1,38–40 While extended posterior fusion may provide more predictable outcomes in clearly unstable ASD, it is associated with substantial disadvantages, including greater blood loss, prolonged operative time, increased perioperative morbidity, and the potential for further degeneration at adjacent levels.1,7,24 Conversely, several series have reported satisfactory clinical outcomes with decompression-only strategies in stable ASD, particularly when minimally invasive or endoscopic techniques are employed.7,24,30,31 These findings are largely derived from retrospective analyses without standardized definitions of stability or long-term follow-up, limiting the strength of the available evidence. Nevertheless, decompression cannot be universally considered safe for all ASD patients. Aggressive or concomitant decompression at adjacent levels, especially in the presence of sagittal imbalance or facet joint compromise, has been associated with an increased risk of symptomatic ASD progression. Hikata et al. demonstrated that additional adjacent-level decompression following lumbar fusion did not necessarily reduce ASD incidence and could even accelerate its development in certain patient subsets.
41
These findings reinforce the concept that decompression alone is rational only within a well-defined subgroup of stable ASD, whereas fusion remains an important option when instability is suspected or confirmed.7,24,41 Within this framework, the technical characteristics of UBE offer specific advantages. The use of two independent portals allows separate control of visualization and instrumentation, facilitating precise and targeted decompression in anatomically altered revision settings. The panoramic field of view and continuous irrigation enable clear delineation of the central canal, lateral recess, and foraminal regions while minimizing unnecessary bone resection and facet joint violation. Preservation of posterior elements and facet joints is particularly critical in ASD, as excessive resection may further disrupt segmental biomechanics and predispose to secondary instability.7,24 In contrast, open or extensive microscopic revision procedures often entail greater paraspinal muscle trauma and facet joint compromise, which may translate into inferior mid to long term biomechanical outcomes.1,41–45 Recent studies have begun to explore the role of unilateral biportal endoscopic (UBE) decompression in the management of adjacent segment pathology. These reports, predominantly retrospective in design, have demonstrated encouraging short-term clinical outcomes, including pain relief and functional improvement. However, these studies are generally limited by small sample sizes, heterogeneous patient populations, and the lack of clearly defined stability-based selection criteria. In addition, follow-up durations remain relatively short, and comparative analyses with fusion-based revision strategies are largely lacking.46–48 Notably, a recent 2025 UBE-ASD series reported favorable clinical outcomes but also documented delayed instability in a subset of patients, with some eventually requiring fusion.
48
This finding underscores the importance of cautious interpretation when considering decompression-only strategies. In the present study, no cases of delayed instability or conversion to fusion were observed; however, this may be attributable to factors such as shorter follow-up duration, stricter patient selection, and the exclusion of patients with suspected instability. In addition, the use of a tissue-preserving surgical technique characterized by minimal disruption of posterior stabilizing elements and limited laminotomy, as shown in Figure 4, may have contributed to maintaining segmental stability. Although this cannot be established definitively within the scope of this study, careful surgical execution and adherence to stability-preserving principles may play a role in optimizing outcomes. Consistent with the existing literature, the present study supports the potential role of endoscopic decompression in selected patients with ASD. By incorporating a more explicitly defined, stability-oriented selection framework, our findings aim to further clarify the subset of patients in whom decompression-only strategies may be considered. While these observations align with the broader fusion-sparing trend in lumbar stenosis literature, ASD should not be directly equated with primary stenosis due to its unique post-fusion biomechanical context. Three-dimensional CT reconstruction demonstrating the limited extent of laminotomy and preservation of posterior osseous structures following unilateral biportal endoscopic (UBE) decompression. The image illustrates a tissue-preserving approach with minimal disruption of posterior stabilizing elements. The part indicated by the yellow arrows is the area where the laminotomy was performed.
Sagittal alignment is a key determinant in ASD and highlights the need for individualized surgical planning. In this context, the role of endoscopic decompression in ASD may be described as relieving symptoms while preserving sagittal alignment, rather than actively correcting global balance.33,49,50 In the present study, sagittal alignment was assessed using standing lateral radiographs, focusing on segmental kyphosis at the adjacent level. Postoperative findings showed no evidence of radiographic deterioration in segmental alignment. Although the magnitude of change in segmental kyphosis was small, alignment appeared to be maintained during the follow-up period. No radiographic signs of newly developed instability were observed. These findings should be interpreted cautiously, given the limited magnitude of change and the absence of formal reliability analysis. Although patients with overt instability or significant deformity were excluded, this selection strategy aligns with current biomechanical concepts of ASD and likely contributed to the favorable clinical and functional outcomes observed. When instability and deformity are carefully ruled out, UBE posterior decompression appears capable of providing meaningful symptomatic relief while maintaining sagittal alignment, supporting its role as a biomechanically neutral yet clinically effective treatment option. Beyond efficacy, surgical safety and perioperative morbidity are central considerations in ASD management. Extended revision fusion procedures have been associated with increased blood loss, longer operative times, and higher complication rates, particularly in elderly or medically fragile patients. In contrast, endoscopic and biportal decompression techniques have been shown to offer a more favorable perioperative profile, characterized by reduced tissue trauma, lower blood loss, and shorter hospital stays.1,7,24,31 Reports focusing on ASD and adjacent level stenosis have documented relatively low rates of major neurological complications, deep infections, and early conversion to fusion following endoscopic decompression. In the present series, the observed complication rate was 11.7% (2/17), which may appear relatively high for a minimally invasive technique. However, this finding should be interpreted in the context of the small sample size, where a limited number of events can disproportionately influence the overall rate. Moreover, ASD represents a technically demanding clinical scenario, often characterized by altered anatomy, epidural scarring, and segmental degeneration, which may increase procedural complexity even in minimally invasive approaches. Importantly, all procedures were performed after completion of the surgeon’s learning curve, suggesting that these complications are less likely related to early technical inexperience and more reflective of the intrinsic challenges of the technique in this specific patient population. Furthermore, the concept of “minimally invasive” should not be interpreted as risk-free, but rather as an approach aimed at reducing tissue disruption while maintaining adequate decompression. Therefore, our findings should be considered within the framework of feasibility and early clinical outcomes, and larger studies with longer follow-up are necessary to more accurately define the true safety profile of this approach. Although perioperative complications were observed in two patients, both events were successfully managed without permanent neurological sequelae, and overall postoperative clinical improvement was sustained across the cohort. These findings are consistent with previous reports describing acceptable and manageable complication profiles in endoscopic and biportal decompression for adjacent segment disease7,34,36,46–48,51 Notably, the observed complications highlight the importance of careful perioperative management, particularly in patients with underlying comorbidities such as anticoagulant use, even when standard preoperative protocols are followed. Despite the limited sample size, our findings are in line with previous studies suggesting that UBE decompression may be considered in selected patients. However, outcomes remain dependent on surgical experience and institutional expertise.52,53
Several limitations of the present study should be acknowledged. First, the retrospective design and relatively small sample size limit the generalizability of the findings and preclude definitive conclusions regarding the long-term durability of decompression-only strategies in ASD. Importantly, the small cohort reflects a highly selected patient population meeting strict criteria for “stable” ASD treated with decompression alone, which may further limit external applicability. Although statistically significant clinical and radiological improvements were observed, the study was not powered to identify predictors of failure or to compare decompression with extended fusion strategies. Second, the absence of a control group treated with revision fusion restricts direct comparison between surgical strategies. As a result, the findings should be interpreted as evidence supporting the feasibility and short- to mid-term effectiveness of UBE decompression in selected patients rather than as proof of superiority over fusion-based revision procedures. Accordingly, no causal or comparative inference can be made regarding the relative efficacy of UBE versus other treatment strategies, including alternative decompression techniques or conservative management. Third, global alignment and spinopelvic parameters were not available for all patients and were not analyzed as a primary quantitative endpoint, limiting detailed biomechanical interpretation. Given the well-established role of sagittal balance in ASD pathogenesis and progression, the lack of detailed alignment data limits more nuanced biomechanical interpretation of the results. Although patients with overt instability or deformity were excluded, subtle alignment abnormalities may still have influenced outcomes and could not be evaluated within the scope of this study. Fourth, the follow-up duration may be insufficient to fully capture late instability, recurrent symptoms, or the eventual need for additional fusion in some patients. ASD is known to evolve over time, and longer follow-up is essential to determine whether symptom relief achieved with decompression alone is sustained or merely delays the progression of disease and the eventual need for fusion-based revision surgery. Forth, all procedures were performed by a single experienced surgical team at a tertiary referral center. While this ensured technical consistency, it may limit the external validity of the results, as outcomes and complication rates associated with UBE are known to be influenced by the learning curve, surgeon experience, and institutional volume. Finally, intraobserver and interobserver reliability were not formally assessed (e.g., using ICC), which may limit the interpretation of small radiological differences. Despite these limitations, the study provides clinically relevant data on a narrowly defined patient population and contributes to the growing evidence supporting minimally invasive, stability-preserving approaches for the management of ASD.
Consequently, in selected patients with stable adjacent segment disease following lumbar fusion, biportal endoscopic posterior decompression was associated with meaningful improvements in pain, function, and walking capacity, along with effective radiological decompression. By preserving posterior elements and avoiding additional fusion, this tissue-sparing approach may offer a less invasive treatment option in carefully selected cases, particularly in elderly patients or those with significant comorbidities in whom surgical morbidity is a major concern. These findings highlight the importance of meticulous patient selection and a stability-oriented surgical strategy. However, given the study design, the results should be interpreted as preliminary and hypothesis-generating. Further prospective, comparative, and long-term studies are required to determine the durability of symptom relief and to clarify the role of UBE decompression relative to fusion-based revision strategies in the management of adjacent segment disease.
Footnotes
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the local ethics committee. (Selcuk University, Date: 16.12.2025, Number: 2025/722) The Ethics Committee waived the requirement for informed consent, as the study was retrospective and used previously collected data.
Consent to participate
Therefore, obtaining informed consent from participants was not necessary according to national regulations.
Author contributions
A.G. Conceptualization, Methodology, Formal analysis, Writing - Original Draft, Writing - Review & Editing, Project administration. E.E. Conceptualization, Writing - Original Draft, Writing - Review & Editing. A.B Validation, Investigation, Data Curation, Methodology, Writing - Original Draft. Ay.G. Methodology, Formal analysis, Writing - Original Draft. B.K.A Writing - Original Draft, Writing - Review & Editing, Supervision. S.C. Validation, Investigation, Data Curation, Formal analysis, Methodology, Writing - Original Draft. All authors have read and approved the final submitted manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Selçuk University Scientific Research Projects (BAP) provided support for the article processing charge of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to the fact that they involve patient-related information obtained from the hospital but are available from the corresponding author on reasonable request.