
Abstract
Objective
This study examined the trends in demographics, the distribution of microorganisms, and antibiotic resistance in patients with periprosthetic joint infection (PJI).
Methods
We conducted a retrospective study of 231 consecutive patients diagnosed with PJI in our hospital from January 2006 to December 2015 (93 and 138 patients diagnosed in 2006–2010 and 2011–2015, respectively). The linear-by-linear chi-squared test was used to assess the trends in demographics, the distribution of microorganisms, and antibiotic resistance.
Results
Gram-positive cocci accounted for 63.9% of all pathogens, and coagulase-negative Staphylococcus (CoNS) accounted for 38.1% of all isolates. The proportion of isolates identified as methicillin-resistant CoNS significantly increased over the study period (39.0% vs. 61.8%). In addition, the proportions of levofloxacin-resistant CoNS (4.9% vs. 21.8%) and Staphylococcus aureus (6.3% vs. 45.0%) isolates significantly increased over the study period. By contrast, the proportions of penicillin-resistant CoNS (82.9% vs. 40.0%) and S. aureus (75.0% vs. 30.0%) isolates decreased over the study period.
Conclusion
Our research revealed changes in the distribution of microorganisms and antibiotic resistance profile of the pathogens responsible for PJI over time, which could complicate treatment. These findings may serve as a reference for strategies to prevent and empirically treat PJI in China.
Introduction
Periprosthetic joint infection (PJI) has become a major focus of orthopedic doctors in China and other countries in recent years because it is a catastrophic complication of joint replacement that seriously affects the function of the affected limb and imposes heavy physical, psychological, and economic burdens on patients. PJI is also one of the most challenging problems faced by orthopedic surgeons in clinical practice. Although advances in technology, strict aseptic techniques, and various preventive measures have reduced the incidence of PJI, the number of patients requiring joint replacement is increasing as the Chinese economy develops. The absolute number of patients with PJI has increased. Therefore, achieving an accurate diagnosis and prescribing effective treatments are particularly important. Identification of the responsible pathogenic bacteria to enable the targeted use of antibiotics plays a vital role in the diagnosis and treatment of PJI.1–4
The distributions of pathogenic microorganisms responsible for PJI differ across countries and regions.5–7 Different pathogenic microorganisms and variations in drug resistance affect the efficacy of treatments for PJI.8–10 Recent studies illustrated that the distribution of microorganisms and antibiotic resistance profiles can change over time.11–13 However, most studies focused on European and American countries.
The purpose of our study was to determine the trends in demographics, the distribution of microorganisms, and antibiotic resistance in patients with PJI in China. This study provides information that may serve as a reference for strategies to prevent and empirically treat PJI in China.
Patients and methods
This retrospective study included patients who were treated for PJI in our hospital between January 2006 and December 2015. This study was approved by the institutional review board of Chinese People’s Liberation Army General Hospital. Because this was a retrospective study that did not analyze patients’ private information, the need for signed informed consent was waived. This study complied with the Strengthening the Reporting of Observational Studies in Epidemiology statement. 14
All patients consented to treatment in our hospital. We investigated the trends in the distribution of microorganisms and antibiotic resistance profiles in patients with PJIs in our hospital over a decade. We divided this period into two 5-year intervals (2006–2010 and 2011–2015) to reduce bias. The rate of infection after initial joint replacement in our hospital is extremely low, and most infected patients have undergone initial joint replacement surgery in other hospitals.
The inclusion criterion was a diagnosis of PJI according to the criteria established by the Philadelphia International Consensus Conference. 15 According to those criteria, a prosthesis is considered to be infected when one of the following main criteria exists: the presence of a sinus communicating with the prosthesis or the isolation of the same pathogen from cultures in at least two separate samples obtained from the affected prosthetic joint. Alternatively, if at least three of the following six minor conditions are met, the prosthesis is considered to be infected: elevated serum erythrocyte sedimentation rate and serum C-reactive protein level, elevated synovial white blood cell count, elevated percentage of neutrophils in synovial fluid, suppuration in the affected joints, microorganisms isolated from a culture of tissue or fluid surrounding the prosthesis, and the presence of more than five neutrophils in each high-power field.
Specimens for culture were obtained from synovial fluid and infected necrotic tissue in the joint capsule, medullary cavity, or acetabulum. Standard microbiological techniques were used to identify and test the drug susceptibility of isolates in accordance with the methods approved by the Clinical and Laboratory Standards Institute. The collected specimens were plated in different media and broths to culture aerobic bacteria, anaerobic bacteria, and fungi and to test the drug sensitivity of the isolates. The specimens were incubated in a constant temperature incubator at 37°C for 18 to 24 hours before isolation and purification. A sufficient number of pure colonies was obtained with a sterile inoculation loop and added to 3.0 mL of sterile saline (0.45%–0.50% NaCl, pH 5.0–7.2) to prepare a bacterial suspension. Using an electronic turbidity meter to measure turbidity, suspensions of gram-positive and gram-negative bacteria were prepared within the range of 0.50 to 0.63 McGill units. For fungal cultures, the specimens were cultured on Sabouraud glucose agar and chocolate agar plates and incubated at 25°C for 2 weeks. The VITEK2 Compact system (bioMérieux, Marcy-l’Étoile, France) was used for identification and antimicrobial susceptibility testing of the bacterial suspensions.
We recorded patient demographics, comorbidities, pathogens, and drug resistance. When multiple pathogens were intermittently cultured from the same joint, the preoperative or intraoperative culture results were recorded. Infection with multiple strains of bacteria was defined as the simultaneous isolation of more than two pathogenic bacterial strains from the tissue or synovial fluid surrounding the prosthesis. The trends in demographics, the distribution of microorganisms, and antibiotic resistance were analyzed.
Statistical analysis
The linear-by-linear chi-square test was used to assess the trends in demographics, the distribution of microorganisms, and antibiotic resistance in patients with PJI. Statistical significance was indicated by P < 0.05. SPSS version 25.0 software (IBM, Armonk, NY, USA) was used for statistical analysis.
Results
Demographics
In total, 231 patients were enrolled from January 2006 to December 2015. Among them, there were 93 patients diagnosed between 2006 and 2010 and 138 patients diagnosed between 2011 and 2015. The demographic characteristics of all patients are presented in Table 1. The sex ratio (P = 0.472) and age (P = 0.217) were not significantly different between the two periods. The proportion of patients with knee joint PJI increased from 40.9% in the first period to 58.0% in the second period (P = 0.011).
Patient characteristics.

IHD, ischemic heart disease; COPD, chronic obstructive pulmonary disease.
▲ Significant at P < 0.05.
In terms of comorbidities, the proportions of patients with hypertension and ischemic heart disease increased from 23.7% and 5.4%, respectively, in the first period to 37.0% and 15.2%, respectively, in the second period (P = 0.033 and P = 0.021, respectively). The prevalence of other comorbidities, such as diabetes, arrhythmia, and chronic obstructive pulmonary disease, did not significantly differ between the two periods.
Distribution of microorganisms
As highlighted in Table 2, 252 pathogenic microorganisms were isolated from 231 patients with PJI. In total, 21 patients were infected with multiple strains of bacteria, including 8 and 13 patients in the first and second periods, respectively. The rate of infection with multiple bacteria did not differ between the periods (8.6% vs. 9.4%, P = 0.832; Table 3). Table 2 presents the distribution of microorganisms. The main pathogens were gram-positive cocci, accounting for 63.9% of the isolates, and the most common pathogen was coagulase-negative Staphylococcus (CoNS), accounting for 38.1% of the isolates. Gram-negative bacilli accounted for 12.3% of the isolates, fungi accounted for 5.6% of the isolates, and Mycobacterium spp. accounted for 2.4% of the isolates. In total, 15.9% of the bacterial cultures were negative. The distribution of these microorganisms did not differ between the two study periods.
Microorganisms in patients with periprosthetic joint infection.

CoNS, coagulase-negative Staphylococcus.
Polymicrobial infections.
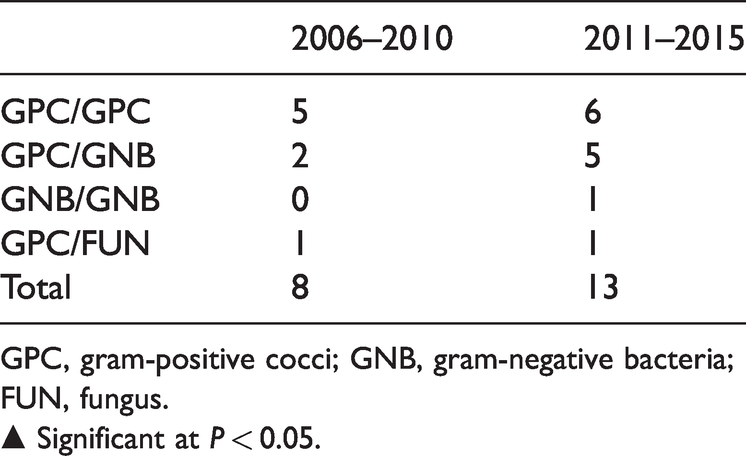
GPC, gram-positive cocci; GNB, gram-negative bacteria; FUN, fungus.
▲ Significant at P < 0.05.
The percentage of isolates that were gram-positive cocci was slightly lower in the second period (66.3% in 2006–2010, 62.3% in 2011–2015; P = 0.509). Among them, the proportions of CoNS, Staphylococcus aureus, and Enterococcus all decreased slightly from 40.6%, 15.8%, and 5.9%, respectively in the first period to 36.4%, 13.2%, and 4.0%, respectively, in the second period (P = 0.505, P = 0.565, and P = 0.473, respectively). The percentage of isolates that were streptococci increased over the study (3.0% vs. 7.3%; P = 0.144), but the difference was not significant.
The proportions of isolates that were gram-negative bacilli also slightly decreased over the study (12.9% vs. 11.9%; P = 0.822). Among them, the proportions of isolates that were Pseudomonas aeruginosa, Escherichia coli, and Klebsiella pneumoniae all decreased slightly from 6.9%, 3.0%, and 3.0%, respectively, in the first period to 5.3%, 2.6%, and 1.3%, respectively, in the second period (P = 0.592, P = 0.879, and P = 0.360, respectively).
The percentages of isolates that were fungi and Mycobacterium spp. increased from 3.0% and 1.0%, respectively, in the first period to 7.3% and 3.3%, respectively, in the second period (P = 0.144 and P = 0.273, respectively).
The percentage of cultures that were negative for bacteria decreased slightly over the study (16.8% vs. 15.2%; P = 0.734).
Increased resistance to methicillin and oxacillin was observed among Staphylococcus spp. (Table 4). Among them, the proportion of methicillin-resistant CoNS (MR-CoNS) increased significantly (39.0% vs. 61.8% P = 0.03). In addition, the proportions of CoNS and S. aureus isolates that were resistant to levofloxacin also increased significantly from 4.9% and 6.3%, respectively, in the first period to 21.8% and 45.0%, respectively, in the second period (P = 0.02 and P = 0.01, respectively). By contrast, the proportions of CoNS and S. aureus isolates that were resistant to penicillin decreased from 82.9% and 75.0%, respectively, in the first period to 40.0% and 30.0%, respectively, in the second period (both P = 0.01).
Antimicrobial resistance of gram-positive bacteria.
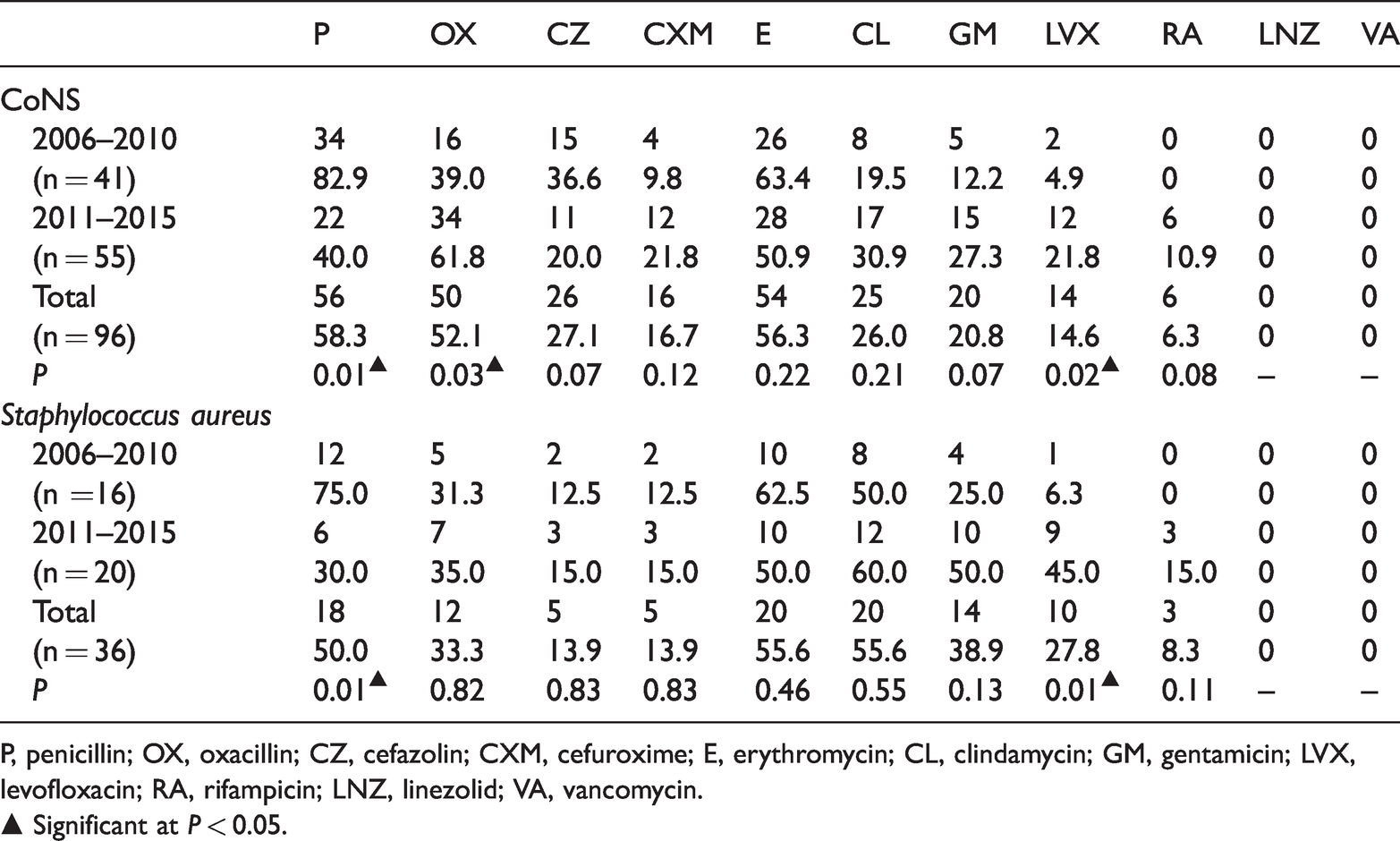
P, penicillin; OX, oxacillin; CZ, cefazolin; CXM, cefuroxime; E, erythromycin; CL, clindamycin; GM, gentamicin; LVX, levofloxacin; RA, rifampicin; LNZ, linezolid; VA, vancomycin.
▲ Significant at P < 0.05.
The proportion of gram-negative bacilli isolates that were resistant to third- and fourth-generation cephalosporins increased significantly from 23.1% in the first period to 66.7% in the second period (P = 0.018; Table 5).
Antimicrobial resistance of gram-negative bacteria.

GNB, gram-negative bacteria; GM, gentamicin; CPX, ciprofloxacin; LVX, levofloxacin; ATM, aztreonam; C, cephalosporin III/IV; SCF, cefoperazone and sulbactam; TZP, piperacillin–tazobactam; AMC, amoxicillin/clavulanic acid; CARBA, carbapenems.
▲ Significant at P < 0.05.
Discussion
In this study, the distribution of microorganisms was not significantly different between the two periods. CoNS was the most common pathogenic microorganism identified in patients with PJI, accounting for 38.1% of all cultures. The prevalence of S. aureus was approximately 14.3%. Similar to the findings in European countries, 16 the most common pathogenic microorganism in the United States 16 and Taiwan 17 is S. aureus. The prevalence of other gram-positive cocci, such as Enterococcus and Streptococcus spp., is lower. Bjerke-Kroll et al. 7 reported an increase in the incidence of PJI caused by Streptococcus spp. There was an increase in the number of infections by Streptococcus spp. in our center, but this increase was not statistically significant.
Gram-negative bacilli also play an important role in infections of prostheses. Gram-negative bacilli accounted for 12.3% of the isolates in our center, which is consistent with reports in the literature, with proportions ranging from 5% to 20%.18,19 A recent Spanish multicenter study reported a significant increase in the incidence of PJI caused by Enterobacteriaceae, 13 but the proportions of cases caused by gram-negative bacilli in our center were not significantly difference between the two period.
Fungi and Mycobacterium spp. were rarely the causative pathogens of PJI, causing approximately 1 and 0.4% of all cases of PJI, respectively.13,20 In our center, 5.6% of the isolates were fungi, and 2.4% were Mycobacterium spp. These proportions were higher than those in previous studies. The reason may be that some patients underwent artificial joint replacement surgery in another hospital, and they had already received treatment for PJI with broad-spectrum antibiotics and re-operation in those hospitals. 21 The small number of cases in our study may have affected the statistical analysis. A Spanish multicenter study also reported a significant increase in the incidence of PJI caused by fungi. 13 The proportions of fungal and mycobacterial infections increased in our center, but the differences were not significant.
The proportion of negative bacterial cultures in our center was 15.9%. In a previous 15-year study, the incidence of negative cultures ranged 11.9% to 33.3% each year. 22 The proportion of negative bacterial cultures in our center only slightly decreased, and it is important to further increase the proportion of positive bacterial cultures.
In our study, the proportion of Staphylococcus isolates resistant to methicillin or oxacillin increased over the study period. Among them, the proportion of MR-CoNS isolates increased significantly. This is consistent with the widespread high prevalence of methicillin-resistant Staphylococcus spp. in China. 23 The results are consistent with the findings in a report published by Stefansdottir et al., 5 who reported that the proportion of MR-CoNS isolates increased annually. This trend was possibly attributable to the country’s antibiotic management policies. 16 In addition, the proportions of CoNS and S. aureus isolates that were resistant to levofloxacin were also significantly higher in the second period. This may be because levofloxacin is an unrestricted antibacterial drug that has a broad bactericidal spectrum, few side effects, convenient oral and intravenous administration routes, a moderate price, and widespread use, leading to increased drug resistance. Conversely, the proportions of CoNS and S. aureus isolates that were resistant to penicillin decreased. This may be attributable to unplanned restrictions on antibiotics that led to reduced resistance. Therefore, planned restrictions on antibiotics constitute a possible means of reducing antibiotic resistance. The antibacterial treatment of PJI is likely to become increasingly complicated. We cannot blindly choose antibiotics that have a broader antibacterial spectrum because of the increase in the prevalence of infection by MR-CoNS. We need to weigh the advantages and disadvantages, determine the risk factors, and design individualized antibiotic treatment regimens.
In the treatment of PJI, the resistance of gram-negative bacilli to antibiotics is problematic and leads to poor therapeutic efficacy. 24 Benito et al. 13 reported that the resistance of gram-negative bacilli to ciprofloxacin was significantly increasing. 13 In our study, the proportion of isolates of gram-negative bacilli that were resistant to third- and fourth-generation cephalosporins significantly increased over the study period, but our number of cases was small. Therefore, it may be necessary to avoid the use of third- and fourth-generation cephalosporins as initial prophylactic antibiotics or to wait for the results of PJI cultures rather than administering antibiotics empirically.
The reasons for the observed trends are unclear. We observed an increase in patients with knee PJI. The proportion of patients with hypertension and ischemic heart disease is increasing. Other possibilities include changes in microbiological diagnoses or antimicrobial practices, although further study is required for validation.
These observations may reflect global differences in the distributions of microorganisms and antibiotic resistance in patients with PJI. The findings of this study may serve as a reference for strategies to prevent and empirically treat PJI in China. It is necessary for infectious disease experts, microbiologists, and orthopedic surgeons to continue to monitor the distribution of microorganisms and antibiotic susceptibility patterns related to PJI in China. This research will provide a reference for future research.
This study had several limitations. First, because of its retrospective design, selection bias was unavoidable. In addition, some patients underwent artificial joint replacement and initial treatment for PJI in another hospital, which may have led to confounding bias. Third, this was a single-center study with a relatively small number of cases. The results need to be further confirmed in multicenter, large-sample studies.
Conclusions
We found that the distribution of microorganisms did not significantly change over a 10-year period. CoNS was the most common pathogenic microorganism. The proportion of MR-CoNS isolates significantly increased. The proportions of CoNS and S. aureus isolates that were resistant to levofloxacin also significantly increased over time; contrarily, the proportions of CoNS and S. aureus isolates that were resistant to penicillin decreased. The proportion of isolates of gram-negative bacilli that was resistant to third- and fourth-generation cephalosporins significantly increased. Our research indicated that the distribution of microorganisms and antibiotic resistance in cases of PJI can change over time, and the antibacterial treatment of PJI is likely to become increasingly complicated. It is necessary to weigh the advantages and disadvantages, determine the risk factors, and design individualized antibiotic treatment regimens.