
Abstract
Introduction
Total knee arthroplasty (TKA) requires effective postoperative pain control to promote early mobilization, improve outcomes, and reduce complications. Common strategies include catheter-based analgesia and single-shot nerve blocks, both of which have distinct advantages and limitations. This study aims to compare the outcomes and complications of both techniques in patients who underwent primary TKA.
Materials and methods
This is a retrospective cohort study conducted at a tertiary care hospital. Patients included had undergone primary total knee arthroplasty by a single surgeon and received either a catheter or a single-shot nerve block post TKA as a pain management modality.
Results
The study included 204 patients who underwent TKA. Females represented the majority of the sample (n = 172, 84.3%), with most patients aged 61 years and older (n = 156, 76.4%). The majority of our sample was obese (n = 164, 81.1%). Catheter analgesia was utilized in 110 cases (53.9%) and single-shot nerve blocks in 94 (46.1%). Catheter analgesia use was significantly associated with lower narcotic use after 3 weeks (9.1% vs 90.9%) with a large effect size (Cramer’s V = 0.31, p < 0.001), a better range of motion at discharge (p = 0.013, V = 0.19), and lower pain mean VAS (0.15 vs 3.88), with a very large effect size (Eta Square = 0.68, p < 0.001) compared to a single-shot nerve block.
Conclusions
This study shows that both catheter and single-shot nerve block provided effective postoperative analgesia after TKA. Catheter use was associated with lower VAS scores, less prolonged narcotic consumption, and superior discharge range of motion. Older age independently predicted catheter selection, whereas longer operative time and continued opioid use favored nerve block utilization.
Introduction
Total knee arthroplasty (TKA) is one of the most commonly performed procedures, used to address pain and deformity in patients with knee joint osteoarthritis or other degenerative diseases. TKA mainly aims to reduce pain, enhance mobility, and return to daily living activities. Postoperative pain management is a critical aspect of TKA recovery as effective analgesia not only enhances patient comfort but also facilitates early mobilization, improves functional outcomes, and reduces the risk of complications such as deep vein thrombosis or pulmonary embolism.1–4 However, inadequate pain control can result in prolonged recovery times, increased hospital stay, and a higher risk of chronic pain or opioid dependence.5,6
Adequate pain control in joint arthroplasty comprises preoperative, intraoperative, and postoperative modalities. Oral and intravenous analgesia, regional block, and local infiltration are all suggested modalities that have proven effective.7,8 The latter two treatments aim to reduce pain by targeting nerve pathways, although their mechanisms, durations, and side-effect profiles significantly differ, making the choice of technique a subject of ongoing research.7,8
Catheter-based analgesia (e.g., continuous epidural or femoral nerve catheters) provides prolonged pain relief by continuously administering local anesthetics at a low dose through a catheter placed near the targeted nerve or spinal space. 9 This method enables titration of analgesia, potentially offering more consistent and flexible pain control. However, complications such as hypotension, catheter migration, infection, or motor block might arise, particularly in the elderly or those with comorbidities. 10
On the other hand, single-shot nerve blocks such as the femoral nerve block or lumbar plexus block typically provide fast and effective analgesia by temporarily interrupting the nerve conduction pathways. These blocks have the advantage of a more straightforward application and a quicker recovery time compared to catheters. However, their effect is limited to the duration of the anesthetic agent, often requiring additional analgesia in the postoperative period—such as opioids—to manage pain in the hours following surgery.11–14
Several studies have compared the effectiveness and safety profiles of these two pain management strategies in TKA.9,11 Previous research by Tallawy et al. (2023) suggests that continuous catheter techniques might provide superior pain relief over a longer period, reducing the need for supplemental analgesics. 15 Recent evidence has shown that multimodal analgesia—which combines regional techniques such as nerve blocks with systemic analgesics (e.g., nonsteroidal anti-inflammatory drugs (NSAIDs) or opioids)—can further improve outcomes, reducing both pain and opioid consumption. 5 Despite this, the debate persists concerning whether a catheter or single-shot nerve block offers the best balance between efficacy, safety, and recovery time. In this study, we aim to explore the outcomes of both techniques for patients undergoing primary total knee arthroplasty performed by a single surgeon.
Materials and methods
This was a retrospective cohort study conducted at a tertiary care hospital. The study included a sample of patients who underwent primary TKA for primary knee osteoarthritis between January 2018 and December 2024, utilizing a single surgical approach by a single surgeon and received one of the modalities of pain management post operatively. Patients undergoing revision TKA and those with incomplete data were excluded. Flow Chart is shown in Figure 1. Flow chart for the inclusion criteria.
Non-probability convenience sampling was chosen by including all patients who met the inclusion criteria. Data was collected using a data collection sheet. Patients were divided into two groups based on whether they received a continuous adductor canal block (CACB) or a single-injection adductor canal block (SACB). Data collected included sample demographics. Outcome variables included length of stay (LOS), narcotic use at the 3-weeks point, estimated surgery time, range of motion (ROM) upon discharge, and visual analogue score (VAS), measured on days 0, 1, and 2 postoperatively.
A comprehensive statistical analysis was conducted, encompassing both descriptive and inferential methodologies. A descriptive analysis was conducted to summarize the demographic characteristics of the participants, including age, gender, and other features. The Chi-Square Test (effect size assessed using Cramer’s V) and Fisher’s Exact Test (effect size also by Cramer’s V) were employed to determine associations between categorical variables. Effect size thresholds for Cramer’s V were interpreted as small (V ≈ 0.1), medium (V ≈ 0.3), and large (V ≥0.5). For continuous variables, the Independent Samples T-Test was applied, with effect size quantified by the mean difference between groups, normality was assessed using the Shapiro–Wilk test and inspection of histograms prior to applying independent t-tests. Thresholds for mean difference were interpreted following Cohen’s convention as small (d ≈ 0.2), medium (d ≈ 0.5), and large (d ≥ 0.8). 16 All statistical analyses were conducted using IBM SPSS Statistics, version 29.0.0.
All data were kept confidential, and patients’ privacy was assured. No identifiers were collected, and all copies were kept in a secure place. Data access was restricted to the study group members.
Results
Sociodemographic and baseline characteristics (Table 1)
Sociodemographic and other parameters of participants (n = 204).

(N) Frequency, (%) Percentage.
Perioperative and postoperative clinical characteristics (Table 2)
Baseline surgical, anesthetic, and postoperative characteristics of patients undergoing total knee arthroplasty (n = 204).

(N) Frequency, (%) Percentage.
Postoperative complications and block-related outcomes (Table 3)
Postoperative complications and pain management-related outcomes following total knee arthroplasty (n = 204).

(N) Frequency, (%) Percentage.
Comparison of postoperative outcomes by pain management modality (Table 4)
Association between postoperative parameters and complications with the pain management modality (n = 204).

aChi-Square Test (Effect Size by Carmer’s V).
bFisher’s Exact Test (Effect Size by Carmer’s V).
cIndependent T Test (Effect Size by Eta Square).
Factors associated with selection of pain management modality (Table 5)
Association between sociodemographic parameters with the pain management modality (n = 204).

aChi-Square Test (Effect Size by Carmer’s V).
bIndependent T Test (Effect Size by Eta Square).
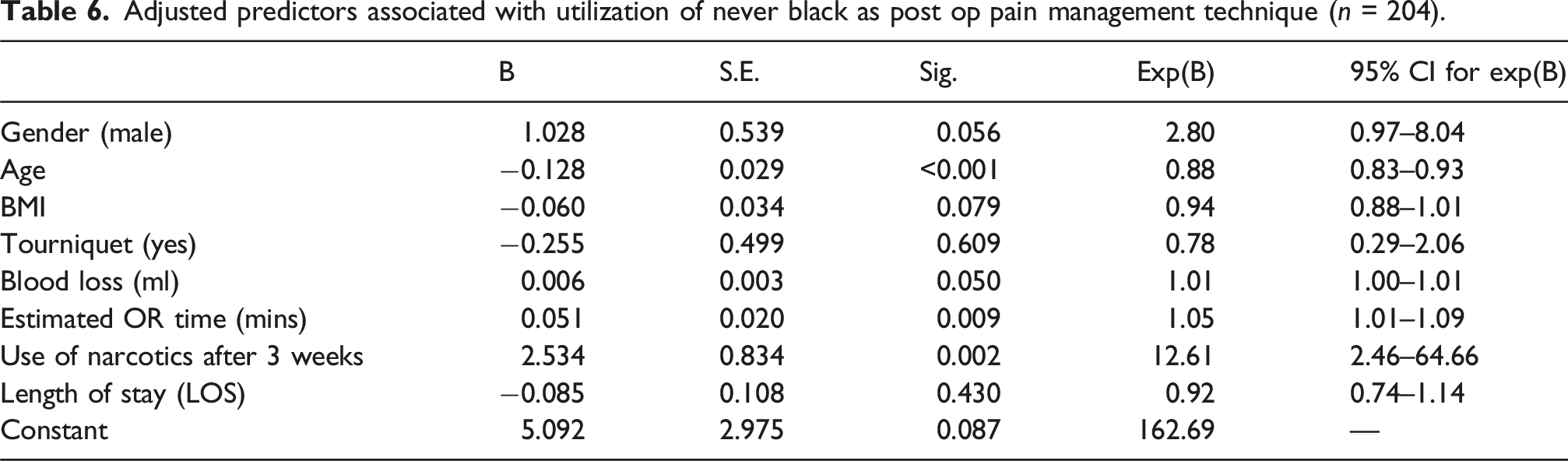
Multivariable analysis of factors associated with selection of postoperative analgesic modality
Adjusted predictors associated with utilization of never black as post op pain management technique (n = 204).
Adjusted predictors associated with utilization of catheter as post op pain management technique (n = 204).

Discussion
TKA is widely performed to relieve pain and improve functional outcomes in patients with degenerative knee conditions. 17 Effective postoperative pain control is paramount in such cases as it contributes to improved patient experience and early mobilization and rehabilitation. 18
The results of this study highlight the outstanding advancements in pain management techniques following knee arthroplasty. The two main techniques for peripheral nerve block are catheter-based analgesia and single-shot nerve blocks, each of which has distinct benefits and limitations. While catheters offer prolonged and adjustable pain relief, single-shot nerve blocks are simpler, with a quicker onset. 19
Among catheter analgesia, CACB is associated with less opioid use, and greater walking distance, as reported by Dobson et al.. 20 This is consistent with the results of Klement et al., raising the question of whether adductor canal block should be the standard practice regarding catheter analgesia. 21 However, to a lesser extent, similar results have been reported with SACB compared to other forms of a single-shot nerve block. 22 Niyonkuru et al. (2024) similarly reported that peripheral nerve blocks significantly reduced opioid use and improve functional recovery in patients who underwent major lower extremity surgery.19,23 Moreover, Erwin et al. (2024) found that femoral nerve blocks provided effective analgesia and were associated with lower morphine requirements compared to systemic opioids or epidural analgesia. 24 These findings are similar to ours, as patients who underwent CACB in our study showed significantly less opioid use.
SACB is a quick and simple method, although it requires an expert to perform, and is short-acting, lasting up to 12-24 h. Therefore, it often requires relocks, which is exhibited in our results, as 32% of our sample who underwent SACB required another block on days 1 or 2 post-operation25,26 Compared to CACB—which is applied in the operating room—it can be simply administered by the nursing staff in the ward, or through an infusion pump, thus reducing costs and improving feasibility. Continuous catheter analgesia offers another advantage in that it can be installed with an ambulatory infusion pump, which can be administered by the patient at home. 27
In terms of pain, our results demonstrated significantly lower VAS scores within the catheter group, in agreement with the results of a meta-analysis published by Jabur et al., which showed superior results of CACB across all domains.28,29
Although highly effective, peripheral nerve block is associated with complications, whereby both techniques have the risk of nerve or vessel damage, as well as local anesthetic systemic toxicity (LAST). 30 The risk of the aforementioned complications can be reduced with US-guided block. 31 Continuous catheter analgesia carries a risk of catheter-related infections, which were found to range from 0% to 3.2% in a systematic review by Nicolotti et al. 32 Risk factors included immunosuppression, diabetes mellitus, postoperative hyperglycemia, postoperative intensive care unit (ICU) admission, and a lack of preoperative antibiotic prophylaxis. Although we did not encounter any cases with catheter-related infection among our sample, we recommend carefully calculating the mode through which local analgesia is delivered in patients with risk factors for catheter-related infections. 32
The importance of postoperative rehabilitation and the immediate ROM cannot be overlooked. Pain has a direct impact on patients’ capacity to perform physiotherapy adequately, which might contribute to a longer hospital stay and further pain due to knee stiffness.33,34 An adductor canal block has the advantage of maintaining quadriceps strength, which favors it over femoral nerve block, as reported by Abdallah et al. 35
Among our sample, catheter-based analgesia was significantly associated with older age, which suggests a clinical bias toward the selection of the catheter-based pain control for more complex or higher-risk patients. This likely reflects real-world clinical practice where continuous analgesia is favored for patients with expected higher pain burdens or mobility limitations, as continuous analgesia is associated with superior pain control following primary TKA. 36
The complication rates across both groups were remarkably low, with no clinically significant complications reported in our study. These findings are consistent with the literature, where both the catheter and single-shot nerve block techniques are generally considered safe when performed under sterile conditions and guided by experienced anesthesiologists. Hasegawa et al. (2022) showed that the overall side-effect profile is favorable compared to other forms of PNB and epidural analgesia. 37
This study has several limitations. Its retrospective design limits causal inference and introduces potential selection bias. Although a multivariable regression analysis was performed in order to adjust for key confounders, unmeasured factors which included baseline functional status, pain tolerance, and rehabilitation adherence, there may still have influenced both analgesic selection and outcomes. No formal correction for multiple comparisons was performed, which imposed further limitation. The single-center setting and convenience sampling further restrict generalizability. In addition, the very low VAS observed in the catheter group may be clinically unexpected and should be interpreted cautiously.
There is a clinical value in tailoring postoperative pain management to the patient’s characteristics and surgical factors. The catheter group showed lower mean VAS score and better early functional outcomes, making them preferable. Future research should focus on multicenter randomized controlled trials to validate these outcomes and assess the long-term functional recovery, quality of life, and cost-effectiveness of each modality within enhanced recovery protocols.
Conclusion
This study shows that both catheter-based and single-shot nerve block techniques have provided effective postoperative pain control after TKA. The use of catheter was associated with lower mean VAS score, lower narcotic consumptions, and improved early range of motion at discharge. However, these findings should be interpreted cautiously given baseline group differences and the retrospective design. Well-designed prospective randomized studies with the long-term functional outcomes and quality-of-life measures are required in order to confirm whether these associations represent a true treatment effect and to guide optimal analgesic selection in contemporary enhanced recovery pathways.
Footnotes
Ethical considerations
This study was approved by King Abdullah International Medical Research Center (KAIMRC) with the following protocol number: NRR24/040/11.
Consent to participate
The need for informed consent was waived due to the retrospective nature of the study.
Authors’ contributions
All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.