
Abstract
Objective:
To determine whether any strength, range of motion (ROM), or functional improvement exists in the adductor canal block (ACB) group after completion of inpatient rehabilitation and following the removal of the continuous block.
Design:
Retrospective cohort.
Setting:
Inpatient rehabilitation at discharge and outpatient orthopedic clinic for follow-up.
Participants:
Two hundred forty-six consecutive primary total knee arthroplasties (TKAs; N = 221 patients) performed by a single surgeon in a single institution between July 2013 and August 2015 for a diagnosis of osteoarthritis.
Interventions:
All TKA cases received a continuous femoral nerve block (FNB) from July 2013 to August 2014 for postoperative pain control. From August 2014 through August 2015, all TKAs received a continuous ACB.
Main Outcome Measures:
Manual muscle tests (MMTs; 0-5 scale) of the quadriceps and passive ROM of the knee were assessed at 3 time periods (hospital discharge [HD], 1-2 weeks, and 1 month). Patient-oriented outcomes and clinical knee scores were examined preoperatively and postoperatively at 3 and 6 months.
Results:
63.6% of FNB cases had an MMT less than 3 at HD and 36.4% of FNB cases had an MMT of 3 or greater at HD. Conversely, 46% of ACB cases had an MMT less than 3 at HD and 54% had an MMT of 3 or greater at HD. There were no statistically significant differences in all postoperative variables at all tested time periods.
Conclusions:
This study showed no short-term postoperative advantages in the ACB group after catheter removal. The superior inpatient rehabilitation course in the continuous ACB group is likely not long enough to translate into any maintained benefit following catheter removal. Nevertheless, the trend toward greater strength in the ACB group in the immediate short term at HD warrants further investigation.
Introduction
Continuous catheter blocks have long been used for postoperative pain control following total knee arthroplasty (TKA). For almost 2 decades, continuous femoral nerve blocks (FNBs) have been an effective adjunct for postoperative pain control following TKA. The FNB provides satisfactory pain control during TKA but also causes quadriceps weakness, which delays physical therapy and places patients at risk of falling. As an alternative, adductor canal blocks (ACBs) have been shown to provide adequate analgesia following TKA by primarily blocking the saphenous nerve. 1 –3 This preserved quadriceps strength afforded by the ACB when compared to the FNB has been supported in multiple studies. 4 –6 Thus, the continuous ACB has been gaining favor as the preferred method of pain control. 7,8 A superior inpatient rehabilitation course 9 –11 with the ACB has also been documented by multiple studies, in terms of earlier ambulation 12,13 with increased ambulation distances 14 –16 and decreased fall risk, 16,17 during the inpatient stay while the catheter is in place.
However, the clinical advantages of ACB compared to FNB after catheter removal have not been explored. Therefore, the primary objective of this study was to determine whether any quadriceps strength or range of motion (ROM) advantage remained in the ACB group following catheter removal during the subacute postoperative period. The secondary objective was to examine whether any functional advantages were evident between the groups in the subacute postoperative period by assessing patient-oriented outcomes and clinical knee scores.
Methods
Participants
The study demographic included patients with osteoarthritis (OA) who received a primary TKA and a continuous nerve catheter (FNB or ACB) for pain control. Exclusion criteria were as follows: revision TKA, TKA for a diagnosis other than OA, or absence of a continuous nerve catheter as part of the patient’s pain control regimen.
Study Design and Statistical Analysis
A retrospective study was conducted on 246 consecutive primary TKAs (221 patients) performed by a single surgeon in a single institution between July 2013 and August 2015. A continuous FNB was used on all TKA cases in the study from July 23, 2013, to August 12, 2014, for postoperative pain control. From August 18, 2014, through August 3, 2015, all TKAs included in the study received a continuous ACB. This change from postoperative continuous FNB to continuous ACB nerve block was the only change made to the TKA protocol during this time period.
The primary objective of this study was to determine whether any quadriceps strength or ROM advantage remained in the ACB group following catheter removal during the subacute postoperative period. The cases were separated into 2 groups based on the type of continuous catheter blocks they received following surgery: (1) femoral nerve block group (FNBG; n = 104) or (2) adductor canal block group (ACBG; n = 142) with ropivacaine. Manual muscle tests (MMTs; 0-5 scale) of the quadriceps and passive ROM were assessed at 3 time periods (hospital discharge [HD], 1-2 weeks, 1 month after surgery). The MMT values obtained were separated into 2 groupings based on antigravity strength ([0, 1, 2] = less than antigravity strength vs [3, 4, 5] = antigravity strength or greater). This was done in order to increase power for analysis and to make the MMT measure more objective. The ROM testing was conducted with a goniometer. Both MMT and ROM assessments were conducted by the operating physician. The MMT measurements were assessed with Pearson χ2/Fisher exact tests (categorical variables). Fisher exact test was utilized for the definitive analysis of the manual muscle testing data as this data set called for a 2 × 2 contingency table (2 groups tested with 2 possible outcomes) and represents a more accurate statistical tool under these circumstances. The ROM measurements were assessed with independent t tests (continuous variables).
The secondary objective was to examine whether any functional advantages were evident between the groups in the subacute postoperative period by assessing patient-oriented outcomes and clinical knee scores. These variables were assessed postoperatively at 3 and 6 months after surgery. The following patient-oriented outcomes were assessed: pain intensity and frequency as measured by a visual analog scale (VAS, range 0-10), Quality of Well-Being 7 total score, Short Form 36 (SF-36) physical function, role physical, bodily pain, general health, vitality, social functioning, role emotional, mental health, physical component summary, and mental component summary scores and Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores (function, pain, stiffness, and total). The following clinical knee measures were assessed: Hospital for Special Surgery (HSS) knee score and Knee Society knee/function scores. These same variables, with the addition of knee active and passive flexion, were also assessed preoperatively to look for any differences between the groups at baseline. Independent t tests were utilized for these comparisons.
Demographics and baseline patient characteristics were recorded for all cases in the study. The values included the following: age, gender (male vs female), race (white vs black), ethnicity (Hispanic vs non-Hispanic), body mass index (kg/m2), Charlson comorbidity index, American Society of Anesthesiologists classification, and chronic opiate prescription (yes or no). Pearson χ2 tests and Fisher exact tests were calculated for categorical variables, while independent t tests were used for all continuous variables. Pearson χ2, Fisher exact, and independent t tests were used to assess significant differences in demographics and baseline patient characteristics. Patient-oriented outcomes and clinical knee measures were compared between both groups using independent t tests. An α was set at .05.
Results
Demographics and baseline variables were not found significantly different between the 2 groups. No attribute or variable was associated with having an ACB or FNB. Consequently, no covariates were used going forward (Tables 1 and 2).
Preoperative Demographics (Categorical Variables): Pearson χ2/Fisher Exact Tests.a

Abbreviations: ACBG, adductor canal block group; FNBG, femoral nerve block group; ASA, American Society of Anesthesiologists.
aFisher exact values were only calculated and utilized for 2 × 2 contingency tables.
bCannot be computed.
Preoperative Demographics (Continuous Variables): Independent Samples Test.

Abbreviations: ACBG, adductor canal block group; BMI, body mass index; FNBG, femoral nerve block group; SEM, standard error of the mean.
The following preoperative patient-oriented outcomes and clinical knee scores assessed with independent t tests were found to yield statistically significant values: VAS–pain frequency; SF-36 bodily pain, vitality, social functioning, and role emotional; Knee Society function score; and WOMAC stiffness and total (Table 3).
Group Statistics at Surgery Presentation (Preoperative; Continuous Variables): Independent Samples Test.

Abbreviations: ACBG, adductor canal block group; FNBG, femoral nerve block group; HSS, Hospital for Special Surgery; QWA, Quality of Well-Being score; SF-36, Short Form 36 score; SEM, standard error of the mean; VAS, visual analog scale; WOMAC, Western Ontario and McMaster University Arthritis Index Score; The bold values represent statically significant values between preoperative measurements in the two groups.
These comparisons revealed superior preoperative scores for those patients who would later receive an FNB (group 1) with regard to VAS–pain frequency; SF-36 vitality and social functioning scores; and WOMAC stiffness and total. Superior preoperative scores for those who would later receive an ACB (group 2) were found with regard to SF-36 bodily pain and role emotional scores and Knee Society knee score. Despite statistically significant differences in the aforementioned variables between both groups at baseline, no group had a clear superiority in outcomes.
The MMTs (0-5 scale) of the quadriceps and passive ROM were compared between the FNBG and ACBG postoperatively at 3 time periods (HD, 1-2 weeks, 1 month). After removal of the continuous blocks at HD, 63.6% of the FNB group had an MMT less than 3 and 36.4% had an MMT of 3 or greater. Conversely, 46% of ACB cases had an MMT less than 3 at HD and 54% had an MMT of 3 or greater at HD. Despite this trend toward a greater preserved quadriceps strength measurement in the ACB group at HD, Fisher exact test assessing the 2 blocks at HD did not yield a statistically significant difference (P = .051). The χ2, Fisher exact, and independent t tests performed to compare all other postoperative variables at all tested time periods did not show associations (Tables 4 through Table 7).
Postoperative Knee Extension Strength With MMT (Hospital Discharge, 1- to 2-Week Follow-Up, 1-Month Follow-Up; Categorical Variables): Pearson Chi-Square/Fisher Exact Tests.a
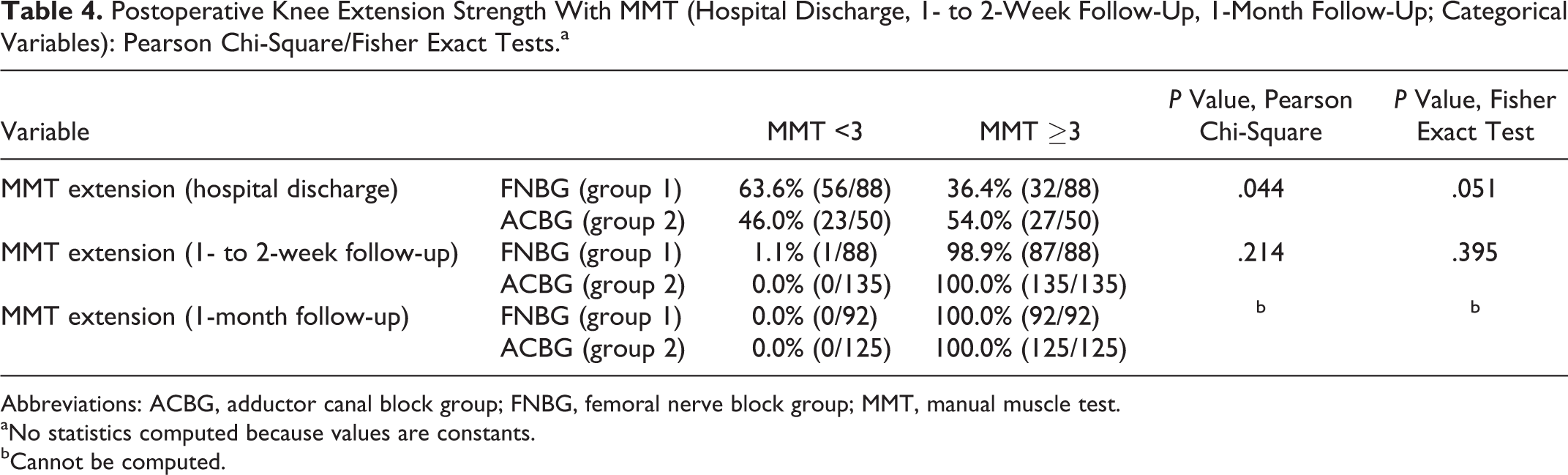
Abbreviations: ACBG, adductor canal block group; FNBG, femoral nerve block group; MMT, manual muscle test.
aNo statistics computed because values are constants.
bCannot be computed.
Postoperative Knee Passive Range of Motion (Hospital Discharge, 1- to 2-Week Follow-Up, 1-Month Follow-Up; Continuous Variables): Independent Samples Test.
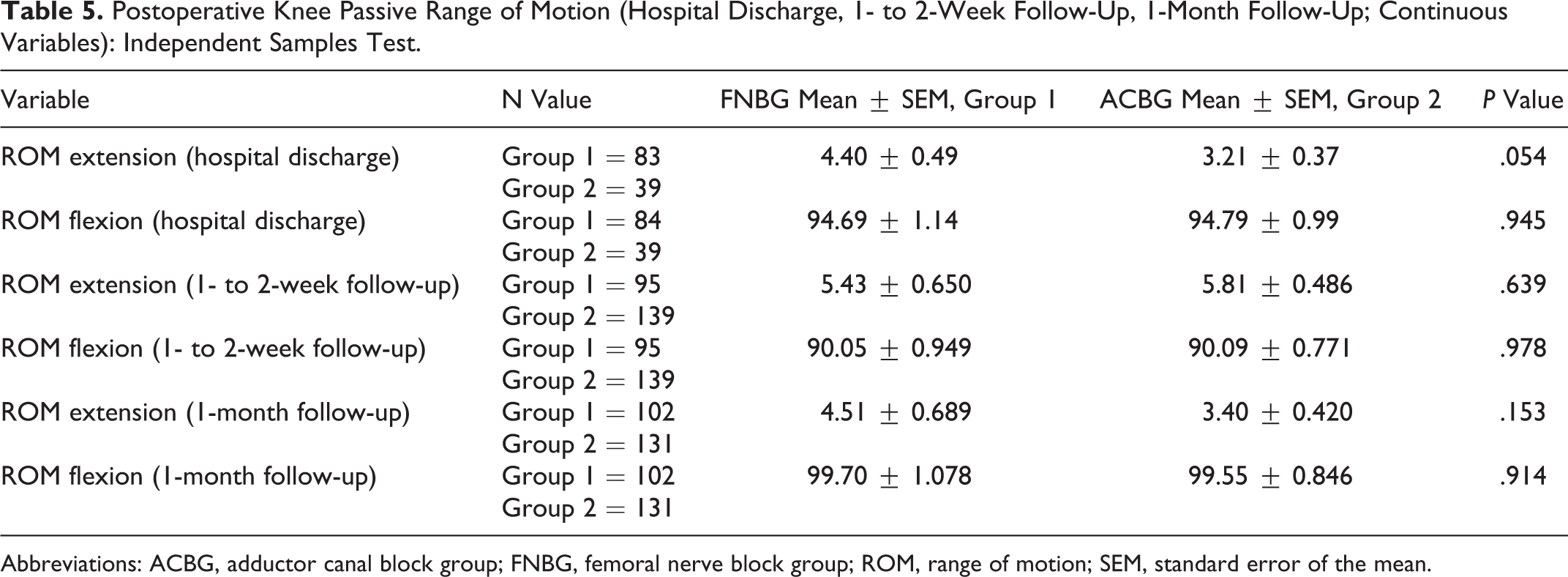
Abbreviations: ACBG, adductor canal block group; FNBG, femoral nerve block group; ROM, range of motion; SEM, standard error of the mean.
Postoperative Patient-Oriented Outcomes and Clinical Knee Scores (3 Months Postoperatively; Continuous Variables): Independent Samples Test.

Abbreviations: ACBG, adductor canal block group; FNBG, femoral nerve block group; HSS, Hospital for Special Surgery; QWA, Quality of Well-Being score; SEM, standard error of the mean; SF-36, Short Form 36 score; VAS, visual analog scale; WOMAC, Western Ontario and McMaster University Arthritis Index Score.
aCannot be computed.
Postoperative Patient-Oriented Outcomes and Clinical Knee Scores (6 Months Postoperatively; Continuous Variables): Independent Samples Test.
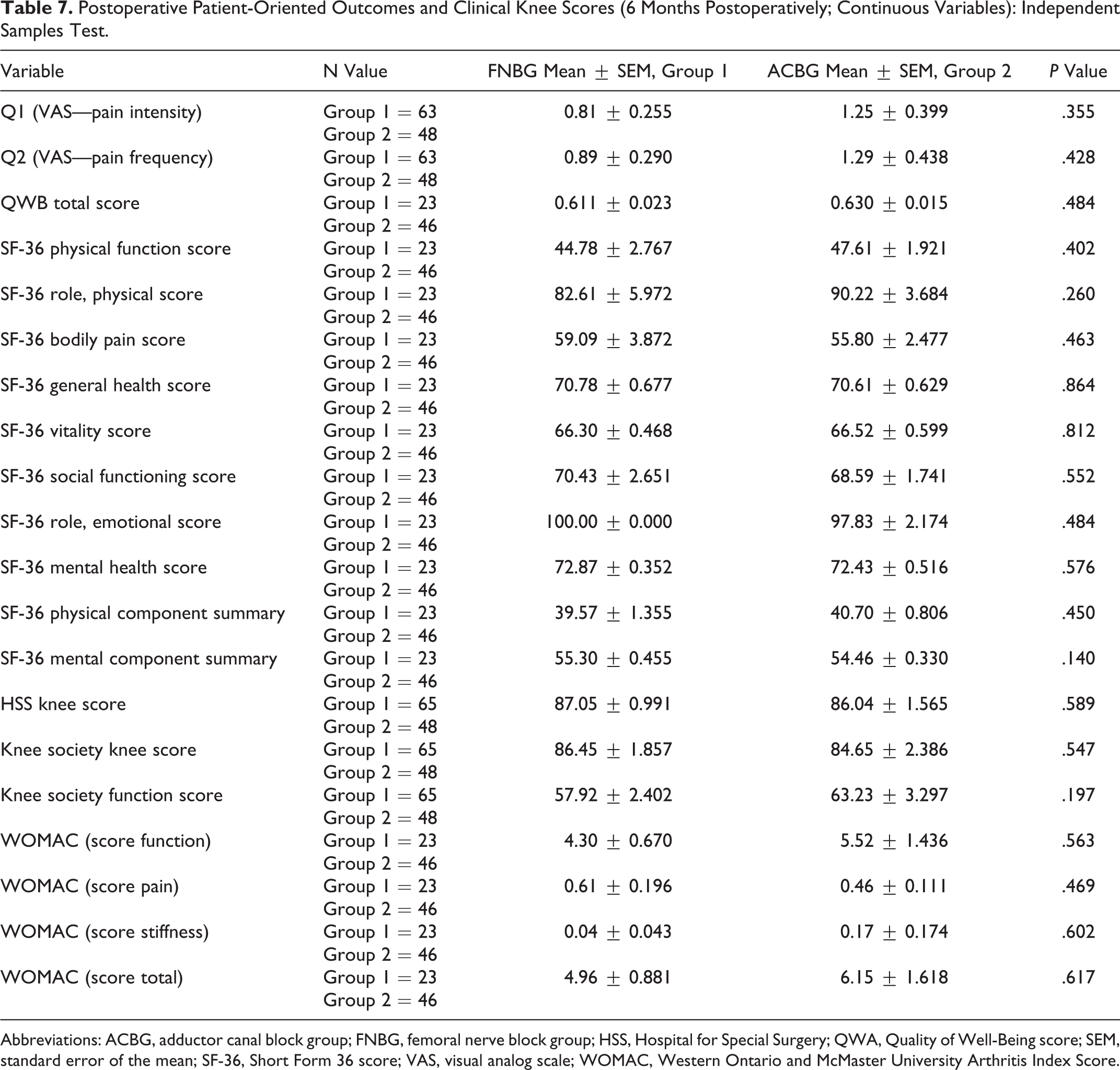
Abbreviations: ACBG, adductor canal block group; FNBG, femoral nerve block group; HSS, Hospital for Special Surgery; QWA, Quality of Well-Being score; SEM, standard error of the mean; SF-36, Short Form 36 score; VAS, visual analog scale; WOMAC, Western Ontario and McMaster University Arthritis Index Score.
Discussion
This study sought to evaluate the impact of ACB versus FNB on the rehabilitation course of TKA cases and whether any advantage observed during the utilization of the catheter translated into functional benefits following removal of the catheter up to 6 months after surgery. The primary objective was to determine whether any quadriceps strength or knee ROM advantage remained in the ACB group in the short term following block removal. The secondary objective was to examine whether any functional advantages were evident in the subacute postoperative period with regard to patient-oriented outcomes and clinical knee scores. The main findings established in this study were as follows: (1) there was no superior quadriceps strength observed in the immediate short term (after catheter removal) associated with receiving an ACB when compared to receiving an FNB; (2) there is no statistically significant difference in the short term with regard to ROM of the operated knees between the 2 block groups; and (3) there are no functional advantages evident between the 2 groups postoperatively with regard to patient-oriented outcomes and clinical knee scores up to 6 months after surgery.
The finding of superior quadriceps strength afforded by the ACB, while the catheter is in place, during inpatient rehabilitation has been previously demonstrated by multiple studies. 4 –6 The preserved strength has been documented to translate into superior inpatient rehabilitation with earlier ambulation, 12,13 increased ambulation distances, 14 –16 and a 70% reduction in fall risk. 16,17 Patients who receive ACB have also been noted to experience an equal level of pain control satisfaction with no increase in opioid consumption when compared to patients who receive FNB. 17 The findings of this study provide new evidence about the rehabilitation course in ACB cases following catheter removal. Despite the established inpatient benefits afforded by the ACB, the data of this study suggest that patients do not continue to experience greater quadriceps strength beyond their inpatient stay after the continuous block is removed. This lack of preserved advantage in the ACB group may be due to the short time period of the inpatient rehabilitation course (with a mean value of 3.62 days in this study). The superior inpatient rehabilitation course in the continuous ACB group, in terms of earlier ambulation and preserved quadriceps strength, is likely not long enough to translate into any maintained benefit immediately following catheter removal.
However, 54% of ACB cases had an MMT of 3 or greater at HD compared to 36.4% of FNB cases with an MMT of 3 or greater at HD. This trend toward greater strength in the ACB group in the immediate short term warrants further investigation with a prospective study and more objective strength measurements. If any strength difference were to exist following the ACB removal, it would be expected to be found in the short term given the short duration of the inpatient rehabilitation course. This equivocal testing time period in this study requires further investigation as it carries implications for patient safety. A patient being discharged from the hospital with greater quadriceps strength is presumably being discharged in a more functional and safer condition. If any significant difference does indeed exist at this point, it may later prove to result in less postoperative falls and complications following HD as well as a sooner return to an optimal functional status. Such evidence would provide an additional nod for the choice of an ACB over an FNB for postoperative pain control following TKA.
In addition to its retrospective nature (level 3 evidence), this study has multiple limitations. First, a standardized time interval between removal of the catheter and measurement of quadriceps strength at HD was not documented in the data used for this study. Second, MMTs (0-5 scale) were used to measure quadriceps strength. A value of 3 (representing antigravity strength) was used as a cutoff value in order to make this measurement more objective. Ideally, a follow-up study would use a dynamometer to objectively measure postoperative strength. Additionally, a follow-up study would measure postoperative quadriceps strength while the catheter is in place as well as beyond removal. Finally, other tests should be considered to monitor function and safety in addition to quadriceps strength. Such tests might include the Timed Up and Go (TUG) test as well as the determination of the rate of postoperative falls throughout the study.
In conclusion, despite numerous studies documenting strength and clinical advantages of continuous ACB while they are in place, data from this study suggest that patients who receive a continuous ACB do not demonstrate a statistically significant greater quadriceps strength after its removal. They also do not appear to have superior functional outcomes after catheter removal otherwise, as demonstrated by lack of differences in knee ROM, patient-oriented outcomes, or clinical knee scores up to 6 months after surgery. Thus, the advantages afforded by continuous ACB in comparison with continuous FNB appear to be limited to the time period while they are in place and actively providing analgesia. However, the trend toward a significant strength advantage in the ACB group after removal of the catheter at HD provides enough equivocal evidence to warrant further investigation on this topic with follow-up studies. A prospective randomized controlled trial is suggested.
Footnotes
Authors’ Note
To the knowledge of the authors, the rehabilitation course of total knee arthroplasties comparing continuous adductor canal blocks and femoral nerve blocks after the removal of the catheters has not been studied in any previously published articles at the time this project was started.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.