
Abstract
Background
The routine use of postoperative drainage after total knee arthroplasty (TKA) remains controversial, particularly in the era of modern blood-saving strategies. While drains have traditionally been used to reduce hematoma formation, their effect on early postoperative pain has not been clearly established. This study aimed to evaluate whether postoperative drainage influences early pain outcomes following primary TKA.
Methods
An assessor-blinded randomized comparative study was conducted including 60 patients undergoing primary hybrid TKA with posterior cruciate ligament preservation. Patients were randomly allocated to a drainage or no-drainage group, with stratification by sex. All patients followed identical anesthetic, surgical, and multimodal analgesic protocols, including routine administration of tranexamic acid. Pain was assessed using the visual analogue scale (VAS) preoperatively and at 48 h postoperatively. The number of postoperative morphine rescue doses was recorded as an objective pain-related outcome. Secondary outcomes included haemoglobin level at discharge and length of hospital stay.
Results
No significant differences were observed between the drainage and no-drainage groups regarding postoperative VAS pain scores, morphine rescue requirements, haemoglobin levels at discharge, or length of hospital stay (all p > 0.05). In both groups, postoperative pain was significantly lower than preoperative pain (p < 0.05). Higher body mass index was associated with greater preoperative pain but did not influence postoperative pain outcomes.
Conclusion
Within contemporary perioperative protocols including tranexamic acid, routine use of postoperative drainage after primary TKA does not improve early postoperative pain control or reduce opioid requirements. These findings support omitting routine drainage without compromising early pain outcomes.
Keywords
Introduction
Total knee arthroplasty (TKA) is an effective and widely performed surgical procedure for end-stage knee osteoarthritis, providing substantial pain relief and functional improvement. As the number of TKAs continues to increase worldwide, optimization of perioperative management has become essential to enhance recovery and minimize complications. 1
Closed suction drainage has traditionally been used after TKA with the aim of reducing postoperative hematoma, minimizing wound complications, and facilitating early mobilization. However, with the widespread adoption of tranexamic acid and modern blood-conservation strategies, perioperative blood loss has been markedly reduced. Consequently, the clinical relevance of routine drainage has been increasingly questioned. Several randomized trials and meta-analyses have failed to demonstrate clear benefits of drainage in terms of blood loss, infection rates, or functional outcomes, while some have suggested potential disadvantages such as increased transfusion rates and delayed mobilization.2,3
One area that has received little attention is the influence of drains on postoperative pain. While it is theoretically possible that drains could reduce pain by decreasing the tension caused by a haematoma, this idea is not consistently supported by high-quality scientific evidence. The available literature does not provide clear evidence that using drains reduces pain in the immediate postoperative period. Furthermore, many of the available studies do not consider pain as a primary outcome, nor do they describe it in sufficient detail, which makes it difficult to draw clear conclusions in this regard.4,5
Adequate pain control is essential to enable early mobilization, which is a cornerstone of enhanced recovery and fast-track protocols after total knee arthroplasty. Despite growing evidence questioning the routine use of surgical drains, their application remains highly variable worldwide. The purpose of this randomized study was therefore to evaluate whether the use of postoperative drainage affects early postoperative pain following primary TKA, using both subjective pain assessment and objective opioid consumption as outcome measures.
Materials and methods
Study design and participants
An assessor-blinded randomised clinical trial was conducted in our institution from September 2024 to January 2025. The trial was approved by the Local Research Ethics Committee.
Patients awaiting hybrid total knee arthroplasty surgery with posterior cruciate ligament preservation were recruited. Those who had previously undergone ipsilateral or contralateral knee surgery (contralateral knee arthroplasty, osteotomy, cruciate ligament repair or meniscal repair), those with a history of rheumatic diseases or joint infection, and those with pathologies that could lead to overestimation of pain were excluded from the study. A pilot study including 20 patients was conducted to estimate variability of the primary outcome. Based on pilot postoperative VAS pain scores (standard deviation 1.75), the study was powered to detect a minimum clinically relevant difference of 1.5 points between groups. Assuming a two-sided alpha level of 0.05 and a power of 80%, the minimum required sample size was 52 patients; therefore, 60 patients were included to account for potential dropouts (Figure 1). Consolidated standards of reporting trials diagram depicting flow of study participants.
Randomization and blinding
Patients were randomly allocated to either a drainage group (Group A) or a no-drainage group (Group B). Randomization was stratified by sex to ensure balanced group distribution. Outcome assessors collecting pain and opioid-use data were blinded to group allocation.
Perioperative protocol
All patients underwent surgery under spinal anesthesia with tourniquet control. Tranexamic acid was administered intravenously at a dose of 1 g before tourniquet inflation and an additional 1 g after wound closure. A standardized multimodal analgesic regimen was used for all patients, consisting of scheduled paracetamol and metamizole, with intravenous morphine available as rescue analgesia.
Outcome measures
Pain was assessed using a 10-point visual analogue scale (VAS) during ambulation preoperatively and at 48 h postoperatively, corresponding to the time of hospital discharge. The number of postoperative morphine rescue doses administered during hospitalization was recorded as an objective indicator of pain control.
Secondary outcomes included hemoglobin level at discharge and length of hospital stay. Demographic data (age, sex, body mass index) were also recorded. All pain-related variables were collected by a blinded investigator.
Statistical analysis
Statistical analysis was performed using SPSS version 28. Continuous variables are presented as means with standard deviations, and categorical variables as frequencies and percentages. Group comparisons were performed using appropriate parametric or non-parametric tests depending on data distribution. A p value <0.05 was considered statistically significant. The study was conducted and reported in accordance with the CONSORT guidelines.
Results
Sixty patients were included and evenly distributed between the drainage (n = 30) and no-drainage (n = 30) groups. The overall mean age was 71 years, and 61.7% of patients were female. Baseline demographic characteristics were comparable between groups.
Descriptive analysis of quantitative variables.

Descriptive analysis of qualitative variables.

Statistical analysis by group (A: with drainage, B: without drainage).
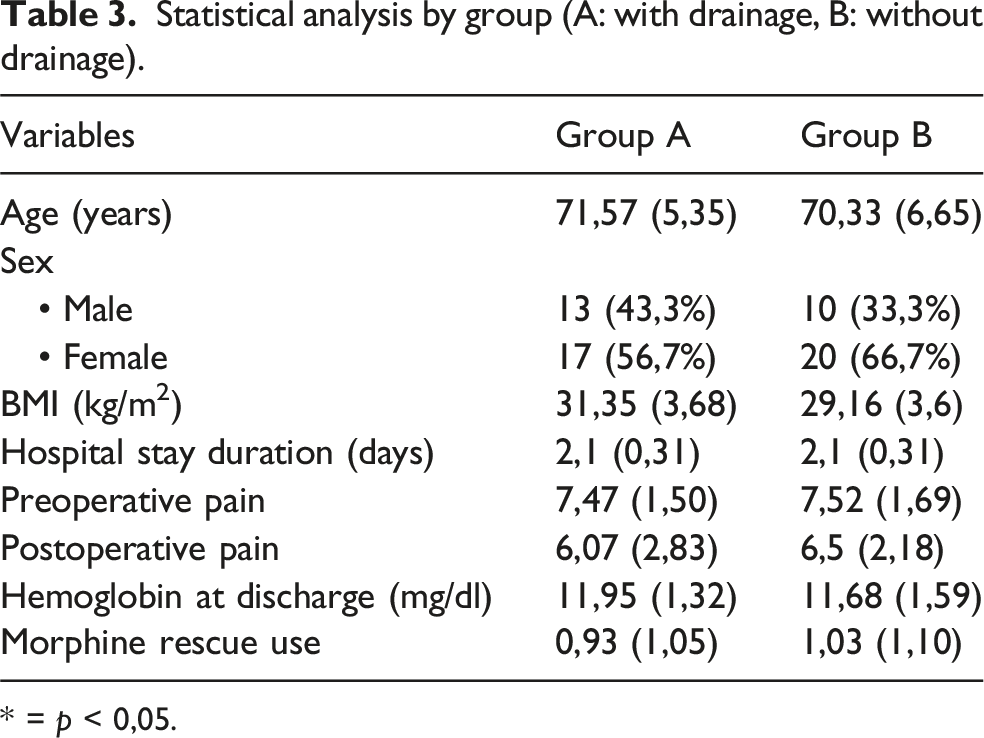
* = p < 0,05.
Comparison of preoperative vs postoperative pain stratified by variables (study group, sex, BMI).

* = p < 0,05.
Discussion
The main finding of this randomized study is that the use of postoperative drainage after primary TKA does not influence early postoperative pain or opioid consumption when contemporary perioperative protocols are applied. Patients in both groups experienced comparable pain reduction and similar analgesic requirements during the early postoperative period.
These findings align with recent scientific evidence, including the work of Zhang et al. (2018), who concluded that routine drain use in TKA does not offer clear clinical benefits and may be linked to increased blood loss and transfusion requirements. 2 Similarly, Maliarov et al. (2023) demonstrated that drainage does not influence early functional outcomes or blood loss, further supporting the absence of significant advantages 6 . These results reinforce the position taken in our study and raise reasonable doubts about the usefulness of this practice in the current context, especially given the routine use of tranexamic acid, which has been shown to significantly reduce bleeding and the risk of postoperative haematomas.
These findings are clinically relevant, as they help to avoid unnecessary procedures that do not provide measurable benefits to patients. In this context, demonstrating the absence of an advantage for routine drainage contributes to optimizing postoperative protocols without compromising outcomes.
The main finding of the study is that the use of drainage did not impact postoperative pain improvement or the use of analgesic rescues. Upon reviewing studies that directly address the relationship between surgical drainage and postoperative pain in knee arthroplasty, we found diverse and generally inconclusive results. Concina et al. (2019) concluded that drainage is associated with greater blood loss, pain and poorer functional recovery. 7 However, differences in study design and perioperative management may limit direct comparison with our results, as all patients in our cohort underwent tourniquet-assisted surgery. Erne et al. (2018) reported very slight differences in pain measured with VAS between the groups in a prospective trial, with no impact on early functional recovery. 8 Although few studies support the use of drains for pain therapy, the study by Maniar et al. (2019) is noteworthy. Like our study, it evaluated the use of drainage and its relationship with morphine analgesic rescue requirements, reporting lower consumption of morphine in the first hours after surgery in patients with drainage compared to those without, who required greater analgesic potency. 9
Compared to these studies, the present study has several distinguishing features. Firstly, pain was the main study variable rather than a secondary subanalysis within a design focused on complications or bleeding. Secondly, dual pain measurement was incorporated: in addition to a validated subjective scale (VAS), an objective, quantifiable measure was included — the number of morphine rescues required — providing a more robust approximation of the real impact of pain in the postoperative period.
We observed that postoperative pain in all patients was significantly lower than baseline, which suggests that the standard analgesic regimen is adequate and effective. This is evidenced by significantly lower postoperative pain (baseline pain = 7.49 vs postoperative pain = 6.28, p < 0.001) and a lower rate of rescue analgesia (approximately 1 per patient). Another notable finding was the influence of BMI on baseline pain, which was higher in patients with a BMI >30. However, this difference was not maintained in the postoperative period. These results suggest that being overweight leads to a more intense perception of pain before surgery, but that postoperative pain management is effective regardless of drainage or BMI. This finding is consistent with previous studies indicating that a high BMI may be a risk factor for greater pain or poorer function in the preoperative period but does not necessarily predict poorer postoperative outcomes if appropriate protocols are followed. 10
Avoiding routine drainage may simplify postoperative care, reduce patient discomfort, and facilitate early mobilization, particularly in high-volume arthroplasty units. These aspects are especially relevant within enhanced recovery pathways, where minimizing invasive measures plays an important role in patient satisfaction and resource optimization.
This study has several limitations. The relatively small sample size may limit the ability to detect subtle differences between groups. In addition, pain assessment was limited to the early postoperative period, and longer-term outcomes were not evaluated. Finally, complete blinding was not feasible due to the nature of the intervention, although the use of objective pain-related variables aimed to reduce potential bias.
Conclusion
The results of this study indicate that the use of surgical drains after total knee arthroplasty does not significantly improve early postoperative pain control. The combined use of subjective (visual analogue scale) and objective (morphine rescue requirements) pain measures provides a robust assessment of this outcome. In the context of optimized perioperative protocols and routine tranexamic acid administration, these findings support avoiding the systematic use of postoperative drains, reserving them for selected cases with a high risk of bleeding or hematoma formation.
Footnotes
Ethical considerations
This study involving human participants was reviewed and approved by the Research Ethics Committee of Córdoba and was conducted in full accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All procedures involving human participants were carried out with the approval of the appropriate institutional and/or national research ethics committee.
Consent to participate
All participants, or their legal guardians in the case of minors or individuals unable to provide consent themselves, provided written informed consent prior to their inclusion in the study. Participants also gave their consent for the publication of the study results.
Author contributions
All authors contributed equally to the conception, design, data collection, analysis, interpretation, and writing of the manuscript. All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors did not receive support from any organization for the submitted work.
Declaration of conflicting interests
The authors have no relevant financial or non-financial interests to disclose.
Data Availability Statement
The datasets generated and analysed during the current study are not publicly available due to ethical and legal restrictions related to the protection of participant privacy and confidentiality, in accordance with the approval granted by the Research Ethics Committee of Córdoba. Sharing the data openly would compromise the anonymity of the participants, as the dataset contains sensitive personal information that cannot be fully anonymised. Data may be available from the corresponding author on reasonable request and with appropriate ethical approval.