
Abstract
Objective
This study examined the associations of visceral adiposity index (VAI), body roundness index (BRI), and lipid accumulation product (LAP) with the risk, severity, and prognosis of knee osteoarthritis (KOA). The aim was to evaluate the clinical utility of these novel adiposity indices for early screening and prognostic assessment of KOA.
Methods
A total of 124 patients with clinically and radiographically confirmed KOA and 120 healthy individuals who underwent routine physical examinations during the same period were enrolled as the KOA and control groups, respectively. Baseline data were collected retrospectively from electronic medical records. KOA patients were further classified into mild, moderate, and severe subgroups based on K-L grading and were followed for 12 months.
Results
Compared with controls, the KOA group had significantly higher BMI, TG, TC, LDL-C, VAI, BRI, and LAP, and lower HDL-C (p < 0.05). VAI, BRI, and LAP increased progressively with KOA severity (p < 0.05), showing positive correlations (r = 0.608, 0.489, 0.551, p < 0.001), and were confirmed as independent risk factors (p < 0.05). ROC analysis yielded AUCs of 0.775 (95% CI: 0.718–0.833; cutoff: 2.91) for VAI, 0.752 (95% CI: 0.692–0.813; cutoff: 5.21) for BRI, and 0.779 (95% CI: 0.722–0.836; cutoff: 48.58) for LAP, with a combined AUC of 0.880 (95% CI: 0.839–0.922). Survival time differed significantly across groups stratified by these cutoffs (VAI: χ2 = 4.238; BRI: χ2 = 3.956; LAP: χ2 = 6.043; all p < 0.05).
Conclusion
This study concludes that VAI, BRI, and LAP are closely linked to KOA. Firstly, their levels are significantly raised in patients and show a positive correlation with disease severity, marking them as useful clinical indicators. Secondly, the combined detection of these indices provides superior predictive value for KOA and is associated with an unfavorable prognosis, suggesting their utility in comprehensive risk assessment.
Keywords
Introduction
Knee osteoarthritis (KOA) is characterized by pathological changes such as articular cartilage degeneration, osteophyte formation, and joint space narrowing. Patients typically experience joint pain, stiffness, and functional limitations. These symptoms significantly impair quality of life and impose a substantial economic burden.1,2 With a growing aging population globally, the prevalence of KOA is rising annually, making it one of the most common causes of disability, particularly among individuals aged over 60.3,4 Among various risk factors for KOA, obesity is a major contributor. It influences KOA primarily through direct mechanical loading on joints, as well as through systemic pathways such as metabolic dysregulation and chronic low-grade inflammation.5,6 In recent years, studies have found that the accumulation of visceral fat is closely related to a variety of metabolic diseases.7,8 Visceral adipose tissue, as a functional adipose tissue, is not only involved in the metabolic process in the body, but also able to secrete a variety of inflammatory factors, leading to a systemic inflammatory response, which in turn has a direct or indirect effect on the cartilage and bone of the joint. The primary drawback of the traditional body mass index (BMI) is its inability to differentiate between fat types or reflect distribution patterns, as it is solely based on weight and height. This limitation restricts its effectiveness in assessing the risk for specific obesity-related diseases, rendering it a suboptimal tool for comprehensive metabolic health evaluation.9,10 Therefore, in recent years, new obesity-related indicators such as visceral adiposity index (VAI), body roundness index (BRI) and lipid accumulation product (LAP) have gradually attracted the attention of researchers. VAI, as an indicator that comprehensively reflects the distribution and metabolic state of abdominal fat, has been widely used to assess the risk of cardiovascular diseases, diabetes and other diseases. Scientific investigations confirm a significant association between the VAI and KOA. Specifically, elevated VAI levels are positively correlated with worsened knee joint dysfunction, a finding most evident in patients presenting with excessive abdominal fat.11,12 BRI is proposed as a new indicator that can reflect the distribution of body shape and fat. It can better evaluate the impact of body shape and visceral fat on the disease through the calculation of variables such as height, weight, and waist circumference.13,14 LAP focuses on the combination of waist circumference and triglycerides. As a simple and highly predictive index, it has been applied to the prevention and management of obesity-related diseases. However, although some progress has been made in the study of novel fat-related indicators such as VAI, BRI, and LAP in other metabolic diseases, there is still a lack of systematic study on their relationship with KOA. Current research on KOA predominantly focuses on BMI, while the role of fat distribution remains underexplored.15,16 Although some studies have acknowledged its influence, a comprehensive analysis utilizing more precise indicators like VAI, BRI, and LAP is notably lacking. Therefore, this study aims to explore the relationship between the levels of VAI, BRI, and LAP and the risk, severity and prognosis of KOA, and further evaluate the clinical application value of these novel fat-related indicators in the early screening and prognosis assessment of KOA.
Patients and methods
Patients
A total of 124 patients consecutively diagnosed with KOA based on clinical and imaging examinations between March 2022 and September 2024 were included in this study, constituting the KOA group. Inclusion criteria: all patients met the American College of Rheumatology (ACR) clinical and imaging diagnostic criteria for KOA 17 ; all had undergone anteroposterior and lateral X-ray examinations of the knee, allowing clear Kellgren-Lawrence (K-L) grading; and complete clinical, imaging, and laboratory data were available. Exclusion criteria: patients with a history of knee surgery; those complicated with rheumatic immune diseases such as rheumatoid arthritis, ankylosing spondylitis, or gout; and those with severe cardiac, hepatic, or renal dysfunction. Additionally, 120 healthy individuals without knee disorders were concurrently recruited from our hospital’s health examination center during the same period and designated as controls. All data were obtained from the electronic medical record system, with complete information available for each case.
Research methods
Basic information was retrospectively collected from all subjects using an electronic medical record system. All KOA patients completed the knee joint X-ray frontal and lateral examination, and the image data were obtained from PACS system. K-L classification 18 : All the images were independently reviewed by two radiologists at the level of doctor-in-charge and above, and then classified according to the degrees of joint space stenosis, osteophyte formation, sclerosis and deformity: Grade I: slight osteophyte may exist; Class II: osteophytes were identified, and the joint space was slightly narrowed; Class III: moderate osteophyte, with significantly narrowed joint space; Class IV: Severe osteophyte, obvious stenosis of joint space and accompanied by bone end deformation. In case of disagreement between the two physicians, a third senior imaging specialist will rule. According to the K-L classification, patients in KOA group were divided into mild group (grade I–II), moderate group (grade III) and severe group (grade IV).
Following an overnight fast, venous blood samples were collected from all participants and analyzed for triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) using standardized automated analyzers in the clinical laboratory. BMI was calculated as weight in kilograms divided by the square of height in meters (kg/m2). The VAI was computed using sex-specific formulas: for males, [waist circumference (WC)/(39.68 + 1.88 × BMI)] × (TG/1.03) × (1.31/HDL-C); for females, [WC/(36.58 + 1.89 × BMI)] × (TG/0.81) × (1.52/HDL-C). BRI = (WC/height) × 100. LAP = WC × TG. All indices were calculated separately by two researchers and subsequently verified.
Patients were followed for 12 months through outpatient, telephone, or home visits. The end point of this study was total knee replacement. Indications of total knee arthroplasty: persistent severe knee pain, conservative treatment is ineffective; Imaging showed severe joint space stenosis or structural damage; The function of knee joint is severely limited, which obviously affects the quality of daily life.
Statistical methods
SPSS 22.0 was used for all statistical analyses, and GraphPad Prism 8 was utilized for graphing. Categorical data were expressed as rates and compared using the chi-square test. Inter-group comparisons of continuous variables were performed with t-tests. Spearman’s analysis was conducted to evaluate correlations. Multivariate analysis was carried out using logistic regression. The predictive value of VAI, BRI, and LAP was determined by ROC curve analysis. Survival analysis was performed with Kaplan-Meier curves, and groups were compared using the Log-rank test. A P-value of less than 0.05 was considered statistically significant.
Results
Comparison of two groups of general information
Comparison of general information between two groups.

Comparison of VAI, BRI, and LAP levels between the two groups
The KOA group demonstrated significantly elevated levels of VAI, BRI, and LAP compared to the control group (p < 0.05). See Figure 1. A comparison of adiposity index levels between the KOA group and the control group, showing (a) VAI, (b) BRI, and (c) LAP. Note. *p < 0.05.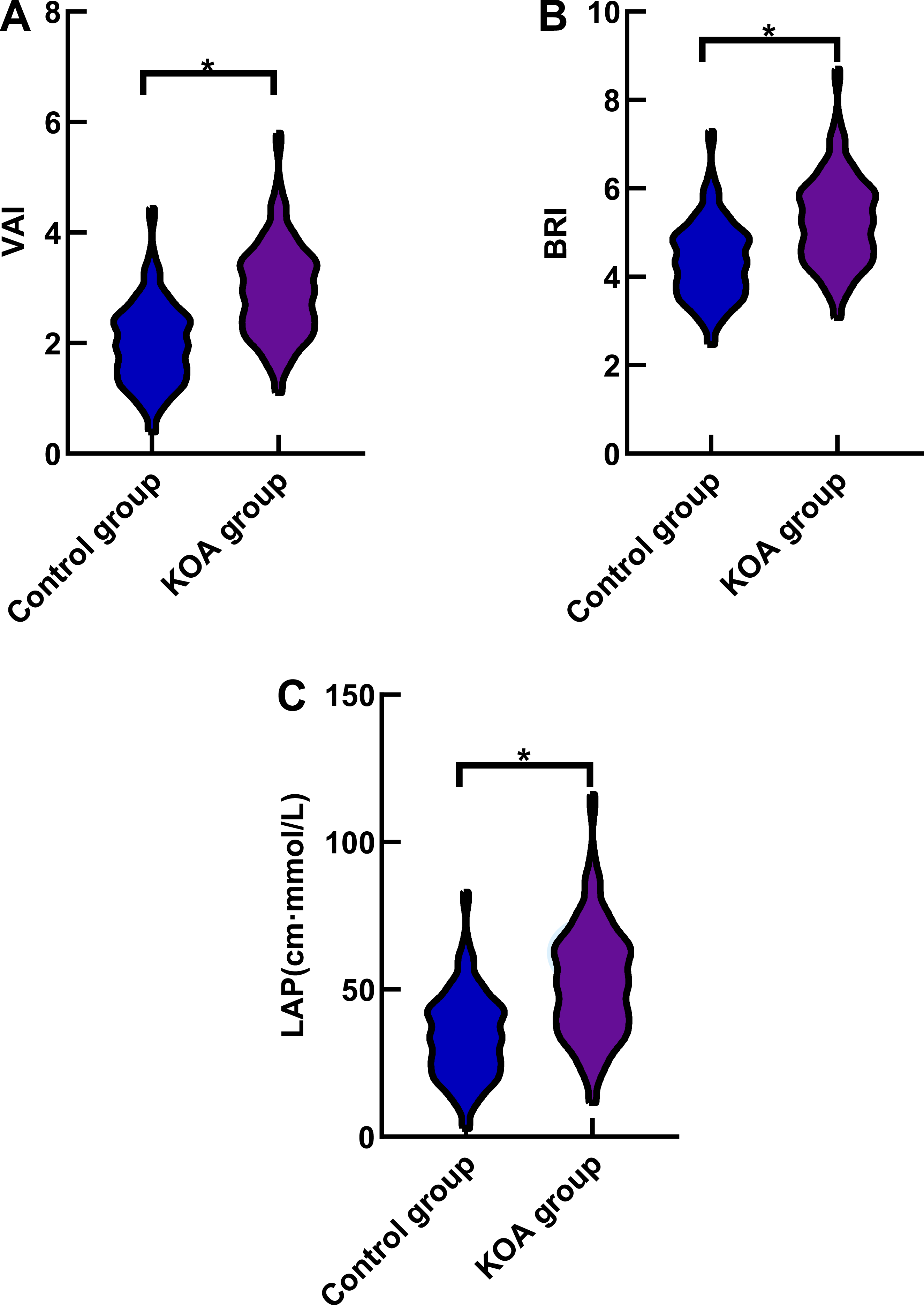
Comparison of VAI, BRI, and LAP levels among patients with KOA of different stages of disease
The VAI, BRI, and LAP levels in the severe group and the moderate group were higher than those in the mild group, and the VAI, BRI, and LAP levels in the severe group were higher than those in the moderate group (p < 0.05). See Figure 2. Levels of adiposity indices stratified by KOA severity. (a) VAI; (b) BRI; (c) LAP. Note. *p < 0.05.
Correlation of VAI, BRI, and LAP with KOA severity
Correlation of VAI, BRI, and LAP with KOA severity.

Multi-factor analysis of risk factors for the development of KOA
Risk factors for onset of KOA by multivariate analysis.

Predicted value of VAI, BRI and LAP levels in predicting the occurrence of KOA
Predicted value of VAI, BRI and LAP levels in predicting the occurrence of KOA.


ROC curves for KOA prediction. (a) VAI; (b) BRI; (c) LAP; (d) combined model.
Analysis of survival curve of VAI, BRI and LAP levels on the prognosis of patients with KOA
The results of Log-rank test showed that there were significant differences in survival time of KOA patients among different VAI (<2.91, ≥2.91), BRI (<5.21, ≥5.21) and LAP (<48.58, ≥48.58) levels (χ2 = 4.238, 3.956 and 6.043, p < 0.05). See Figure 4. Prognostic survival curves for KOA patients. (a) VAI; (b) BRI; (c) LAP.
Discussion
As a disabling disease, the pathological mechanism of KOA cannot be summarized by simple mechanical wear. Obesity has traditionally been considered a major risk factor for KOA by increasing knee joint load, which has led to a core assessment of BMI.19,20 However, the “obesity paradox” is commonly observed in clinical practice, whereby some individuals with normal BMI still develop KOA, while certain severely obese individuals maintain joint health. This suggests that the distribution and functional heterogeneity of adipose tissue may hold greater pathological significance than total body weight.21,22 In recent years, the focus of research has shifted from overall obesity to visceral adipose tissue, and its accumulation will lead to a systemic chronic low-grade inflammation and metabolic disorders.23,24 By assessing the relationship between VAI, BRI, and LAP and the risk and severity of KOA, this study provides a new perspective to explore the relationship between fat distribution and KOA.
Our findings revealed significantly elevated levels of VAI, BRI, and LAP in KOA patients compared to controls. The reason is that the increase of VAI and BRI reflects the abnormal distribution of visceral fat, while the increase of LAP indicates the aggravation of lipid accumulation. This kind of abnormal metabolic state often coexists with many chronic diseases, which may be related to the occurrence and development of KOA by changing the metabolic environment of the body.25,26
Our study found that VAI, BRI, and LAP levels were positively correlated with KOA severity and exhibited a graded increase across patient subgroups with more advanced disease. These results indicated that the levels of VAI, BRI and LAP were closely related to the severity of KOA. The reason is that VAI, BRI and LAP, as indicators that comprehensively reflect the distribution characteristics of visceral fat and lipid metabolism, can sensitively characterize the overall metabolic background related to the progress of KOA. With the aggravation of KOA’s illness, patients’ pain and joint function limitation are becoming more and more obvious, and their daily activities and exercise levels are gradually decreasing. This long-term decrease in activities may be accompanied by further aggravation of visceral fat accumulation and abnormal lipid metabolism, thus making the levels of VAI, BRI and LAP show a trend of gradual increase. On the other hand, visceral fat accumulation often coexists with metabolic regulation imbalance, including abnormal lipid metabolism and changes in insulin sensitivity, which may be aggravated simultaneously in different stages of illness. Although the specific relationship between insulin resistance and systemic hyperglycemia and pro-inflammatory state has not been clearly expounded, the above metabolic abnormalities may jointly constitute an unfavorable systemic metabolic environment, which is related to the severity of KOA. In addition, with the progress of the disease, patients often have multiple metabolic-related comorbidities, and their overall health status and metabolic burden increase, which may also be reflected in the increase of comprehensive metabolic indicators such as VAI, BRI and LAP to varying degrees. Therefore, the incremental changes of VAI, BRI and LAP in different disease grades are more likely to reflect the dynamic accompanying characteristics of metabolic state in the process of KOA progress, rather than the direct driving effect of a single factor on disease progress.27,28
ROC curve analysis demonstrated that the AUCs of VAI, BRI, and LAP for predicting KOA were 0.775, 0.752, and 0.779, respectively. The combined predictive AUC of these three indices for KOA occurrence was 0.880. This further confirms the critical role of visceral fat accumulation and related metabolic disorders in the pathogenesis of KOA. The combined prediction using the three indices demonstrated high predictive value, which can help improve the identification of high-risk populations. Patients with VAI ≥ 2.91, BRI ≥ 5.21, or LAP ≥ 48.58 had shorter survival periods than those with VAI < 2.91, BRI < 5.21, or LAP < 48.58, indicating that patients with higher VAI, BRI, and LAP levels have a poorer prognosis.
Although this study has provided an analysis of the association between indicators such as VAI, BRI, and LAP and the risk and severity of KOA, some limitations remain. Firstly, its retrospective, single-center design introduces inherent selection biases that may limit the generalizability of the findings, necessitating validation by future prospective, multi-center studies. Secondly, while correlations were observed, the specific molecular mechanisms underlying the role of dysfunctional adipose tissue in KOA pathogenesis remain unexplored. Subsequent research integrating molecular biology techniques is warranted to elucidate these mechanisms and identify potential therapeutic targets. Furthermore, while VAI, BRI, and LAP are effective predictors of the risk and severity of KOA, these indicators are not the only risk factors for KOA. In future studies, comprehensive analysis should be performed based on multiple factors such as genetic factors and lifestyle to improve the accuracy of KOA prediction model. In this study, the stratified analysis of the progress of different subgroups of patients to total knee arthroplasty was not further carried out, which was mainly limited by the follow-up time and the number of end-point events. However, patients who reached the end point showed higher levels of VAI, BRI and LAP at baseline, suggesting that patients with KOA with more significant metabolic abnormalities may have a faster risk of disease progression. In the future, it is still necessary to clarify the progress characteristics of different high-risk subgroups in prospective studies with larger samples.
Conclusion
This study concludes that VAI, BRI, and LAP are closely linked to KOA. Firstly, their levels are significantly raised in patients and show a positive correlation with disease severity, marking them as useful clinical indicators. Secondly, the combined detection of these indices provides superior predictive value for KOA and is associated with an unfavorable prognosis, suggesting their utility in comprehensive risk assessment.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Natural Science Foundation of Hunan Province (Grant No.2024JJ7528).
Declaration of conflicting interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Publish declarations
All the authors agreed to publish the article.