
Abstract
Background and Aim
Insertional Achilles tendinopathy (IAT) is a degenerative disorder characterized by pain and functional limitation at the tendon’s calcaneal insertion. Surgical intervention is indicated when nonoperative management fails. This study aimed to compare clinical outcomes of calcaneal osteotomy with and without Achilles tendon reinsertion in patients with IAT.
Methods
In this double-blind randomized clinical trial, 42 patients (mean age: 52.25 ± 6.72 years; 69.0% male) with IAT were allocated equally to osteotomy with reinsertion (n = 21) or without reinsertion (n = 21). Functional status and pain were assessed preoperatively and at 3, 6, and 9 months postoperatively using the American Orthopaedic Foot and Ankle Society (AOFAS) ankle–hindfoot scale and the Visual Analogue Scale (VAS) for pain at rest and during activity. Complication rates were also recorded.
Results
In the reinsertion group, mean AOFAS scores improved from 51.00 ± 14.81 preoperatively to 66.33 ± 12.59 (3 months), 68.81 ± 20.54 (6 months), and 68.81 ± 20.54 (9 months). In the non-reinsertion group, scores improved from 55.10 ± 12.84 to 63.67 ± 14.22, 70.38 ± 13.14, and 70.38 ± 13.14, respectively. VAS scores for pain during activity and rest decreased progressively in both groups, approaching near-zero levels by 9 months. No statistically significant between-group differences were observed for AOFAS or VAS improvements (p > 0.05). Complication rates were low and comparable between groups.
Conclusion
Both surgical techniques provided significant and sustained pain reduction and functional improvement over 9 months. Achilles tendon reinsertion did not confer measurable short-term advantages when a substantial portion of the native insertion was preserved, although potential long-term biomechanical benefits needs further investigation.
Keywords
Introduction
The Achilles tendon is the largest and strongest tendon in the human body, connecting the gastrocnemius and soleus muscles to the calcaneus and playing a central role in walking, running, and jumping. 1 Insertional Achilles tendinopathy (IAT) is a degenerative condition affecting the tendon’s enthesis at the calcaneal insertion, often leading to pain, stiffness, and functional limitations. 2 This condition accounts for approximately 20%–30% of all Achilles tendon disorders and affects both athletic and non-athletic populations. 3 Beyond impairing sports participation, IAT significantly reduces health-related quality of life compared to the general population. 4
The pathophysiology of IAT is multifactorial, involving repetitive mechanical loading, microtrauma, and a failed healing response, which leads to collagen disorganization, neovascularization, and possible calcific deposits. 5 Intrinsic risk factors include anatomical variations, limited ankle dorsiflexion, increased body mass index, and age-related tendon degeneration, 6 while extrinsic factors include training errors, inappropriate footwear, and surface hardness. 7 Haglund deformity, which is a bony prominence of the posterosuperior calcaneus, has been strongly associated with tendon compression and exacerbation of IAT symptoms. 8
Nonoperative treatment, as the first-line approach, includes extracorporeal shockwave therapy, orthotic modifications, and nonsteroidal anti-inflammatory drugs. 7 However, failure rates of nonoperative management remain substantial, prompting consideration of surgical intervention in recalcitrant cases. 9 Surgical options target both bony and soft-tissue pathology and include debridement, retrocalcaneal bursectomy, calcaneoplasty, Zadek osteotomy, and tendon reinsertion. 10 While these techniques can provide substantial symptom relief, they vary in invasiveness, rehabilitation time, and complication profiles. 11
Calcaneal osteotomy, particularly dorsal closing wedge osteotomy (DCWCO or Zadek osteotomy), is designed to reduce mechanical impingement of the tendon by altering calcaneal morphology. 10 This approach can be performed with or without reinsertion of the Achilles tendon. Reinsertion aims to restore the tendon’s native footprint and improve long-term biomechanics. 12 Potential advantages include better alignment and preservation of tendon force transmission, 3 while disadvantages involve increased operative time, risk of wound complications, and hardware-related issues. 12 Meta-analytic evidence comparing reinsertion to osteotomy alone suggests that both techniques yield similar functional improvements, but reinsertion may carry higher wound complication rates.
Despite many reports on surgical techniques, direct comparative evidence between calcaneal osteotomy with and without tendon reinsertion in IAT remains limited. 12 Lack of consensus regarding the necessity of reinsertion underscores the need for high-quality comparative studies to guide clinical decision-making. 9 Therefore, the present study aimed to compare clinical and functional outcomes of calcaneal osteotomy with and without Achilles tendon reinsertion in patients with IAT.
Methods
Study design
This study was a parallel-group, non-blinded randomized controlled trial conducted from September 2024 to June 2025 at Akhtar Hospital, Tehran, Iran. The study protocol was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (approval code: IR. SBMU.MSP.REC.1404.146) and registered with the Iranian Registry of Clinical Trials (IRCT20250607066100N1).
Participants
Patients diagnosed with IAT who had the clinical and radiographic criteria for Haglund deformity were enrolled in the study. Exclusion criteria included: history of calcaneal or ankle fracture, previous Achilles surgery, presence of old scars in the Achilles region, and lack of cooperation in follow-up.
Randomization
Eligible patients in whom less than 50% of the Achilles tendon insertion footprint was compromised during surgery were randomized to either the Achilles tendon reinsertion group or the non-reinsertion group. Randomization was performed using computer-generated random block sequences (block sizes of 2, 4, or 6) via the Sealed Envelope online randomization service. Allocation concealment was through sequentially numbered, opaque, sealed envelopes opened in the operating room.
Interventions
All procedures were performed by the same senior orthopedic surgeon specialized in foot and ankle surgery. A midline posterior incision was made over the Achilles tendon. In both groups, the tendon was retracted medially and laterally, degenerative tissue was debrided, and osteotomy was performed. In patients where more than 50% of the tendon’s insertion to the calcaneus was lost during the procedure, the tendon was repaired by drilling a tunnel in the calcaneus and securing the Achilles tendon to the bone using sutures. Patients with less than 50% insertion loss were randomly assigned to one of two groups, including the insertional and non-insertional groups. In the reinsertion group, the Achilles tendon was completely detached, a transosseous tunnel was drilled in the calcaneus, and the tendon was reattached. In the non-reinsertion group, the osteotomy was completed without detaching and reattaching the tendon.
Outcome measures
Primary outcomes were functional status assessed using the American Orthopaedic Foot and Ankle Society (AOFAS) ankle–hindfoot score and pain intensity measured by the Visual Analogue Scale (VAS) during activity and at rest. Assessments were conducted preoperatively and at 3, 6, and 9 months postoperatively. Secondary outcomes included the incidence of postoperative complications such as wound infection or delayed healing.
Sample size
A total of 42 patients (21 per group) were enrolled based on convenience sampling from eligible cases during the study period.
Statistical analysis
All statistical analyses were performed using SPSS for Windows, version 27 (IBM, Armonk, NY, USA). Continuous data are presented as mean ± standard deviation or median with interquartile range, while categorical data are presented as frequencies and percentages. Between-group comparisons of quantitative variables were conducted using the Independent Samples T-test or the Wilcoxon Rank-Sum test, and qualitative variables were compared using Pearson’s Chi-square test or Fisher’s exact test. Longitudinal changes within groups were evaluated using repeated measures ANOVA or the Friedman test, while between-group differences in temporal trends were assessed using generalized linear mixed models. A p-value <0.05 was considered statistically significant.
Ethics
All participants provided written informed consent prior to enrollment. The study was conducted in accordance with the Declaration of Helsinki.
Results
Baseline characteristics
Baseline characteristic of the participants.

aIndependent Sample T-test, Pearson’s Chi-Square Test, Fisher’s Exact Test.
Continuous data are presented as mean with standard deviation.
Categorical data are presented as frequencies and percentages.
BMI: Body Mass Index; DM: Diabetes Mellitus; RA: Rheumatoid Arthritis.
Preoperative findings
The mean preoperative AOFAS score was 55.10 ± 12.84 in the control group and 51.00 ± 14.81 in the intervention group. Moderate pain was the most common pain category, and 42.9% of patients reported limited daily and recreational activities. The most frequent maximal walking distance was 1–3 blocks, with 54.8% experiencing difficulty walking on uneven terrain. Marked gait abnormality was observed in 38.1% of patients. Severe sagittal motion restriction occurred in 45.2%, and moderate hindfoot motion restriction in 50.0%. Hindfoot instability was reported in 40.5%, while 33.3% had good alignment. Mean pain scores were 6.50 ± 0.89 during activity and 3.86 ± 0.52 at rest. No significant differences were found between groups for any subscale or pain score. Detailed findings are provided in Supplemental Table 1.
Third-month evaluation
At 3 months, AOFAS scores improved to 63.67 ± 14.22 in the control group and 66.33 ± 12.59 in the intervention group. Mild, occasional pain was most frequent. No activity limitation was reported by 42.9% in each group. The most common walking capacity was 4–6 blocks in the control group and 1–3 blocks in the intervention group. Difficulty walking on uneven terrain was significantly more prevalent in the control group. Gait was most often normal or slightly abnormal. Sagittal motion was usually moderately restricted in the control group and normal/mildly restricted in the intervention group. Hindfoot motion was most frequently normal or mildly restricted. Hindfoot instability occurred in 23.8% and 28.6% of control and intervention patients, respectively. Alignment was most often fair in both groups. Median pain during activity was 4.00 in both groups, and was 2.00 at rest. Supplemental Table 2 provides complete subgroup data.
Sixth-month evaluation
At 6 months, median AOFAS scores increased further to 71.00 in the control group and 74.00 in the intervention group. The control group most frequently reported mild, occasional pain, whereas no pain was most common in the intervention group. No activity limitation was reported by 61.9% of control and 38.1% of intervention patients, while no limitation of daily activities was most frequent in the intervention group. The predominant walking capacity in both groups was 4–6 blocks, and most participants reported no difficulty on uneven terrain. Gait was most often normal or slightly abnormal in both groups. Sagittal motion was generally moderately restricted in the control group and normal/mildly restricted in the intervention group. Hindfoot motion was most often normal or mildly restricted in the control group but moderately restricted in the intervention group. Hindfoot instability remained infrequent. Alignment was most commonly fair in the control group and good in the intervention group. Median pain during activity was 1.00 in both groups; pain at rest was absent in all participants. Full details are provided in Supplemental Table 3.
Ninth-month evaluation
At 9 months, the mean AOFAS score was 70.38 ± 13.14 in the control group and 68.81 ± 20.54 in the intervention group. No pain was most common in the control group, whereas mild, occasional pain predominated in the intervention group. No activity limitation was reported by 52.4% of control patients and 81.0% of intervention patients. Walking capacity was most often greater than six blocks in both groups. Most patients reported no difficulty on uneven terrain. Gait was usually normal or slightly abnormal. Sagittal motion was most frequently normal/mildly restricted in the control group and in the intervention group. Hindfoot motion followed the same pattern. Hindfoot instability was rare in both groups. Alignment was most often good in the intervention group and poor in the control group, with a statistically significant difference (p = 0.036). Pain during activity was minimal, and pain at rest was absent in both groups. Supplemental Table 4 presents detailed subgroup findings.
Complications and temporal trends in clinical outcomes
Evaluation of complications revealed an increase in pain in three patients within the intervention group; however, this difference was not statistically significant compared with the control group.
Within- and between-group comparisons of AOFAS score and pain outcomes over time.
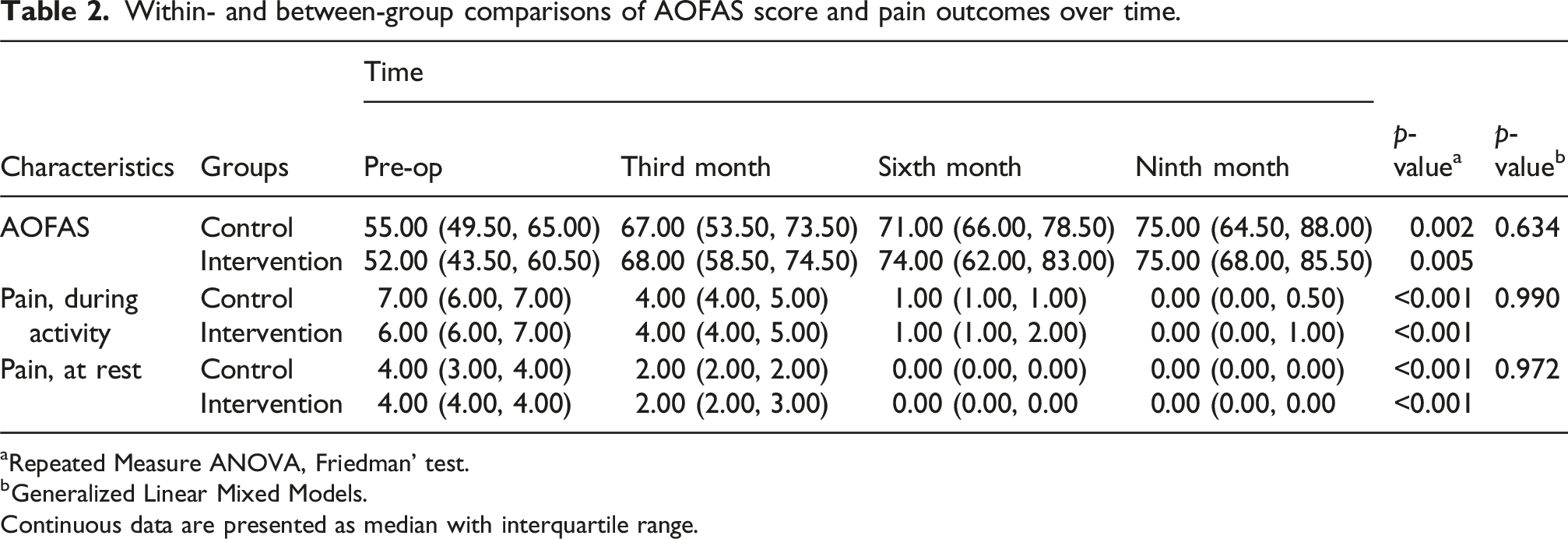
aRepeated Measure ANOVA, Friedman’ test.
bGeneralized Linear Mixed Models.
Continuous data are presented as median with interquartile range.
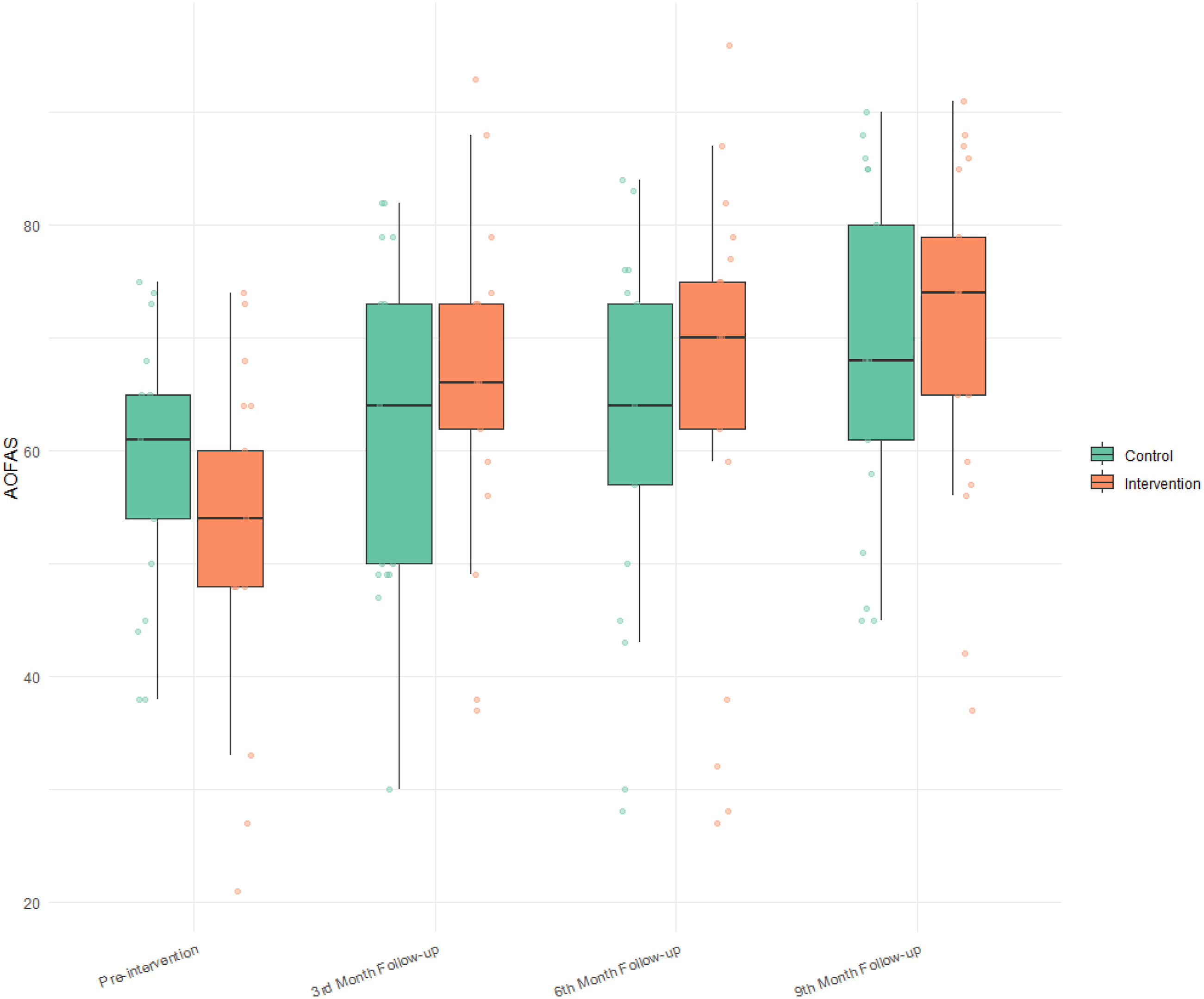
Temporal changes in functional scores from baseline to nine months.
Discussion
This randomized controlled trial evaluated the clinical and functional outcomes of calcaneal osteotomy with and without Achilles tendon reinsertion in patients with IAT. During the 9-month follow-up, both surgical approaches led to a considerable reduction in pain during activity and at rest, with many patients reporting almost no pain by the sixth and ninth months, as shown by VAS scores. AOFAS hindfoot scores also improved, showing better foot and ankle function along with reduced pain. These improvements were consistent and progressive over the follow-up period, which shows a maintained benefit of both surgical approaches. Additionally, complication rates were low in both groups, with no significant between-group differences, which indicates the safety of both interventions.
Our findings are in line with previous meta-analytic evidence, which found no significant functional difference between procedures performed with or without tendon reinsertion in IAT, though reinsertion has been associated with a higher risk of wound-related complications. 12 Similarly, systematic reviews have reported that dorsal closing wedge osteotomy can provide pain relief and functional recovery in patients with IAT; however, they didn’t mention whether reinsertion is performed.10,11 This strengthens the generalizability of our findings, particularly in populations with preserved partial tendon insertion. The lack of between-group differences in our study may be explained by the preservation of sufficient native tendon insertion in the non-reinsertion group, maintaining adequate biomechanical stability for effective postoperative function. Barg & Ludwig (2019) similarly noted that both techniques yield comparable functional outcomes when native insertion is preserved. 9
The biomechanical rationale for reinsertion lies in restoring the physiological footprint of the Achilles tendon, and improving load distribution and force transmission. 1 However, when a large portion of the native tendon insertion is preserved, the biomechanical advantages of reinsertion may have little impact on early postoperative clinical outcomes. This observation aligns with comparative evidence showing similar short-term outcomes between reinsertion and osteotomy-alone techniques Haglund deformity contributes to mechanical compression of the Achilles tendon 8 and reducing this compression has been shown to relieve symptoms in IAT. 13 In our study, by altering calcaneal morphology, both procedures likely reduced the compressive forces that contribute to persistent pain and degeneration. Previous clinical trials have demonstrated that reducing tendon compression either surgically or via targeted rehabilitation can provide significant functional gains in IAT patients. 13 Furthermore, decompression and removal of degenerative tissue appear to be more critical to symptom resolution than full anatomic restoration of the tendon insertion in many cases.2,14
These findings support an appropriate approach to surgical management. In patients with limited insertional compromise, non-reinsertion may reduce operative time, minimize the extent of soft-tissue handling, and lower the risk of wound complications.9,12,15 Conversely, in cases involving more extensive insertional loss or higher biomechanical needs, reinsertion may be necessary for improving long-term tendon function. 16
The strengths of this study include its randomized controlled design, the use of a single experienced foot and ankle surgeon to ensure procedural consistency, and validated outcome measures at multiple postoperative intervals. However, some limitations should be acknowledged. A formal sample size calculation was not performed due to limited prior data, and the relatively small sample may have limited statistical power to detect subtle differences between groups, which may affect the generalizability of the findings. However, the follow-up period of 9 months is sufficient to assess short-term recovery, but may not consider long-term functional or structural outcomes. Previous research has shown that tendon adaptation and remodeling can continue for more than a year. 5 Additionally, the absence of objective biomechanical or imaging-based postoperative assessments limits our ability to correlate structural changes with functional outcomes. Furthermore, patient demographic characteristics such as disease severity, age, activity level, and other individual factors were not analyzed in detail; these variables could influence surgical outcomes. Future research should focus on larger multicenter randomized trials with longer follow-up durations, incorporation of advanced biomechanical assessments, and subgroup analyses based on activity level, extent of tendon degeneration, and comorbidity profiles. Additionally, future studies should control for key demographic and clinical variables such as disease severity, age, and activity level to investigate the effects of surgical technique on outcomes.
In conclusion, both calcaneal osteotomy with and without Achilles tendon reinsertion provided significant and sustained improvements in pain and function in patients with IAT. However, osteotomy without reinsertion appears to be an appropriate and potentially less invasive alternative.
Supplemental Material
Supplemental material - Comparative outcomes of calcaneal osteotomy with and without Achilles tendon reinsertion in insertional Achilles tendinopathy: A randomized controlled trial
Supplemental material for Comparative outcomes of calcaneal osteotomy with and without Achilles tendon reinsertion in insertional Achilles tendinopathy: A randomized controlled trial by Aliasghar Alamian, Ali Motevallizadeh, Amir Bisadi and Mohamad Qoreishy in Journal of Orthopaedic Surgery
Footnotes
Ethics considerations
All procedures were according to the 1961 Declaration of Helsinki and its following extensions. The study protocol was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (approval code: IR. SBMU.MSP.REC.1404.146) and registered with the Iranian Registry of Clinical Trials (IRCT20250607066100N1).
Author contributions
Aliasghar Alamian: Conceptualization, Methodology, Investigation, Data Curation, Writing – Original Draft, Ali Motevallizadeh: Conceptualization, Methodology, Validation, Formal Analysis, Supervision, Project Administration, Writing – Review & Editing, Amir Bisadi: Software, Visualization, Data Curation, Writing – Review & Editing, Mohamad Qoreishy: Resources, Investigation, Validation, Writing – Review & Editing
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be shared if needed by contacting the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.