
Abstract
Background
Thrombocytopenia leads to increased postoperative complications and mortality in elective surgeries.
Questions/purposes
Specific roles of thrombocytopenia on outcomes in orthopedic surgery remain relatively unexplored. This study aimed to assess the impact of chronic thrombocytopenia on outcomes of metastatic spinal tumor surgery.
Patients and Methods
Data from the United States Nationwide Inpatient Sample database 2005 to 2018 were examined. Patients ≥20 years old with metastatic spinal tumors undergoing surgery were identified. Propensity score matching (PSM) was used to balance the baseline characteristics between patients with and without chronic thrombocytopenia. Associations between chronic thrombocytopenia and hospitalization outcomes were determined by logistic regression analyses, adjusted for demographic and clinical factors.
Results
After PSM, a total of 8915 patients were included in the analysis. Chronic thrombocytopenia was associated with increased risk of in-hospital mortality (adjusted odds ratio [aOR] = 2.28; 95% confidence interval [CI]: 1.82-2.86), prolonged length of stay (aOR = 1.89; 95% CI: 1.67-2.14), non-home discharge (aOR = 1.52; 95% CI: 1.35-1.71), and perioperative complications (aOR = 3.14; 95% CI: 2.79-3.54) compared to no chronic thrombocytopenia (all, p < .001). Chronic thrombocytopenia was also significantly associated with increased risk of acute respiratory distress (ARDS) syndrome/respiratory failure (aOR = 2.49), tracheostomy/mechanical ventilation (aOR = 2.49), acute kidney injury (AKI) (aOR = 1.71), venous thromboembolism (aOR = 1.87), transfusion (aOR = 2.41), acute postoperative hemorrhagic anemia (aOR = 2.44), hematoma/seroma (aOR = 2.13), shock (aOR = 2.74), and sepsis (aOR = 1.56).
Conclusion
Chronic thrombocytopenia is a strong independent predictor of worse outcomes following surgery for metastatic spinal tumors.
Clinical Relevance
When managing these patients’ careful consideration of thrombocytopenia is imperative for informed decision-making.
Introduction
Metastatic spinal tumors are the most prevalent neoplasms of the spine, frequently arising from malignancies affecting various sites of the body.1,2 A recent systematic review reported that the occurrence rates of spinal metastases and metastatic epidural spinal cord compression in patients with cancer were approximated at 16% and 3%, respectively, and about 13% cause pathologic vertebral compression fractures, leading to a profound loss of autonomic mobility that significantly diminishes patients’ quality of life. 3 Surgery is often considered when there is spinal instability, significant pain, or neurological deficits due to spinal cord compression. 4 The goals of surgery for metastatic spinal tumors are to relieve symptoms, preserve neurological function, and improve overall quality of life.5,6
A critical factor that can influence the surgical outcomes in general, as well as in spinal tumors specifically, is the presence of thrombocytopenia. 7 Thrombocytopenia is defined as a platelet count below 150,000 cells/µL, and the lower the platelet count, the greater the risk of bleeding during operations as well as from minor traumas experienced in daily life. 8 The etiology of thrombocytopenia encompasses a spectrum of factors, ranging from diminished platelet production to increased platelet destruction, with conditions such as hypersplenism triggered by various diseases contributing to its occurrence. 9
The clinical significance of thrombocytopenia goes beyond its identification in lab tests, influencing preoperative screening protocols and patient management due to its broader implications. 10 Notably, studies have reported that thrombocytopenia can adversely affect the outcomes of orthopedic surgical procedures, including total hip arthroplasty (THA) and total knee arthroplasty (TKA). 11 In addition, thrombocytopenia has been reported to adversely affect the outcomes of spine surgical procedures in a few prior studies.7,12,13 However, the impact of thrombocytopenia on outcomes following surgical intervention for spinal metastases, and whether screening for this condition is beneficial in clinical practice, remains under-researched.
Accordingly, we hypothesized that chronic thrombocytopenia could independently affect short-term outcomes following surgeries for spinal metastases. To fill the knowledge gap, this study aimed to examine the prevalence of chronic thrombocytopenia in these patients and to assess how thrombocytopenia influences surgical outcomes in patients treated for metastatic spinal tumors, using data from a nationally representative database.
Methods
Data source
Data for this study were extracted from the 2005 to 2018 Nationwide Inpatient Sample (NIS), a database developed by the Healthcare Cost and Utilization Project (HCUP) in the United States that is maintained by the Agency for Healthcare Research and Quality (AHRQ). 14 The NIS database represents a 20% sample of inpatient admissions from 45 states and 1051 hospitals that participate in collecting patient data at discharge. Principal and secondary diagnoses, principal and secondary procedures, admission date and diagnosis, discharge status, patient demographic data, and length of stay (LOS) are included for each inpatient. Statistical weights that allow generalized estimates of national case volumes are also provided in the NIS.
Study design and ethical considerations
This retrospective study was population-based and complied with the terms of the NIS data-use agreement. The data utilized in this study were obtained through the Online HCUP Central Distributor. Given that this study solely involved the analysis of secondary data, there was no direct involvement of the general public or patients.
Study population
Patients aged 20 years and older with a diagnosis of metastatic malignant spinal tumors who underwent surgical intervention (either open or minimally invasive procedures) were included in the study. These conditions and procedures were identified from the NIS using the International Classification of Diseases, Ninth and Tenth Revisions (ICD-9 and ICD-10) diagnostic and procedure codes, as listed in Supplemental Table 1. Patients without information on sex, with incomplete information on the main outcomes of interest, with acute thrombocytopenia, thrombotic thrombocytopenic purpura, or heparin-induced thrombocytopenia were excluded. The included patients were separated into 2 groups based on whether or not they had chronic thrombocytopenia. In clinical practice, a diagnosis of thrombocytopenia is generally made when the platelet count is less than 150,000 cells/µL. However, as the NIS is a claims database, we used the following approach to identify chronic thrombocytopenia diagnoses: (1) Diagnostic codes for unspecified primary thrombocytopenia, immune thrombocytopenic purpura (ITP), other primary thrombocytopenia, and congenital/hereditary thrombocytopenic purpura (ICD-9: 287.30, 287.31, 287.32, 287.33, 287.39, 287.5; ICD-10: D69.3, D69.4, D69.6) were applied. (2) To ensure the thrombocytopenia diagnoses were chronic, we cross-referenced these codes with the ‘chronic condition indicator,’ a data flag in the NIS database that specifies if a condition, such as thrombocytopenia, has been present for at least 1 year. (3) As documented in the exclusion criteria above, we excluded codes that explicitly indicate acute thrombocytopenia, such as thrombotic thrombocytopenic purpura or heparin-induced thrombocytopenia. Accordingly, patients identified through these approaches were likely to have chronic thrombocytopenia. While this approach is not as precise as direct lab. data, it is feasible for this type of national claims database analysis, and was adopted in multiple recent publications.11,15–17
Main outcomes and variables
The main outcomes of this study were in-hospital mortality, non-routine discharge, prolonged length of stay (LOS), and perioperative complications. Non-routine discharge was defined as discharge to a long-term care facility. Prolonged LOS was defined as having a LOS ≥75th percentile of the study population (i.e., 13 days). Perioperative complications studied included perioperative cardiac arrest, acute respiratory distress syndrome (ARDS)/respiratory failure, acute stroke, tracheostomy/mechanical ventilation, acute kidney injury (AKI), venous thromboembolism (VTE), transfusion, acute postoperative hemorrhagic anemia, hematoma/seroma, and shock/sepsis, identified through ICD codes.
Demographic variables included patient age, sex, and ethnicity (grouped into white, black, Hispanic, and others), household income, insurance status/primary payer, major comorbidities, severity of comorbid conditions graded by the Charlson Comorbidity Index (CCI), primary tumor site, surgery type, surgical approach (open or minimally invasive), presence of pathologic vertebral fracture, presence of metastatic spinal cord compression, admission type (elective or emergent), and hospital bed size. CCI is a validated scoring system that quantifies overall comorbidity burden and predicts mortality risk based on the presence of 17 weighted chronic conditions. 18
Statistical analysis
The NIS database includes a 20% sample of US annual inpatient admissions. To obtain the national estimates, we applied the trend weight (TRENDWT) for 1993–2011 data and the discharge weight (DISCWT) for 2012–2022 data, as recommended by HCUP. Both weights, together with provided stratum and cluster variables, were incorporated into survey commands to generate nationally representative estimates for all analyses. Descriptive statistics of the patients were presented as number (n) and weighted percentage (%), or mean and standard error (SE). Categorical data were analyzed using the Rao-Scott chi-square test to assess significant differences between the weighted proportions of the two groups. Continuous data were analyzed using a survey-weighted linear model to evaluate differences between groups while accounting for the complex survey design.
To minimize the imbalance of baseline characteristics, the patients in the 2 groups were matched using propensity score matching (PSM) to match as cases and controls in a 1:4 ratio by age category, sex, and admission type. Caliper width for matching was set at 0.2 of the standard deviation of the logit of the propensity score. Logistic regression analyses were used to determine the associations between the presence of chronic thrombocytopenia and other study variables with inpatient outcomes, and results were presented as odds ratio (OR), adjusted OR (aOR), and 95% confidence interval (CI). Covariates with a significant difference between the 2 groups were adjusted for in the multivariable regression. All p values were 2-sided, and values of p < .05 were considered statistically significant. All statistical analyses were performed using the statistical software package SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Patient selection
A flow diagram of patient selection is shown in Figure 1. A total of 184,858 hospitalized patients ≥20 years old diagnosed with malignant metastatic spinal tumors who underwent surgery were identified in the 2005 to 2018 NIS database. Patients with diagnoses of acute thrombocytopenia, thrombotic thrombocytopenic purpura, or heparin-induced thrombocytopenia (n = 382) or missing information on study outcomes or variables (n = 74) were excluded. After PSM, there were 8915 patients included in the analysis: 1783 (20.0%) patients with chronic thrombocytopenia and 7132 (80.0%) patients without thrombocytopenia. This patient sample can be extrapolated to 43,819 adults in the US after employing the weighting method provided by the NIS. Flow diagram of patient selection.
Characteristics of the study population
Characteristics of patients before PSM are summarized in Supplemental Table S2. The mean age of the study population was 63.1 years, half of the patients were male (50%), and about 61% were admitted emergently.
Characteristics of the study population after propensity score matching.
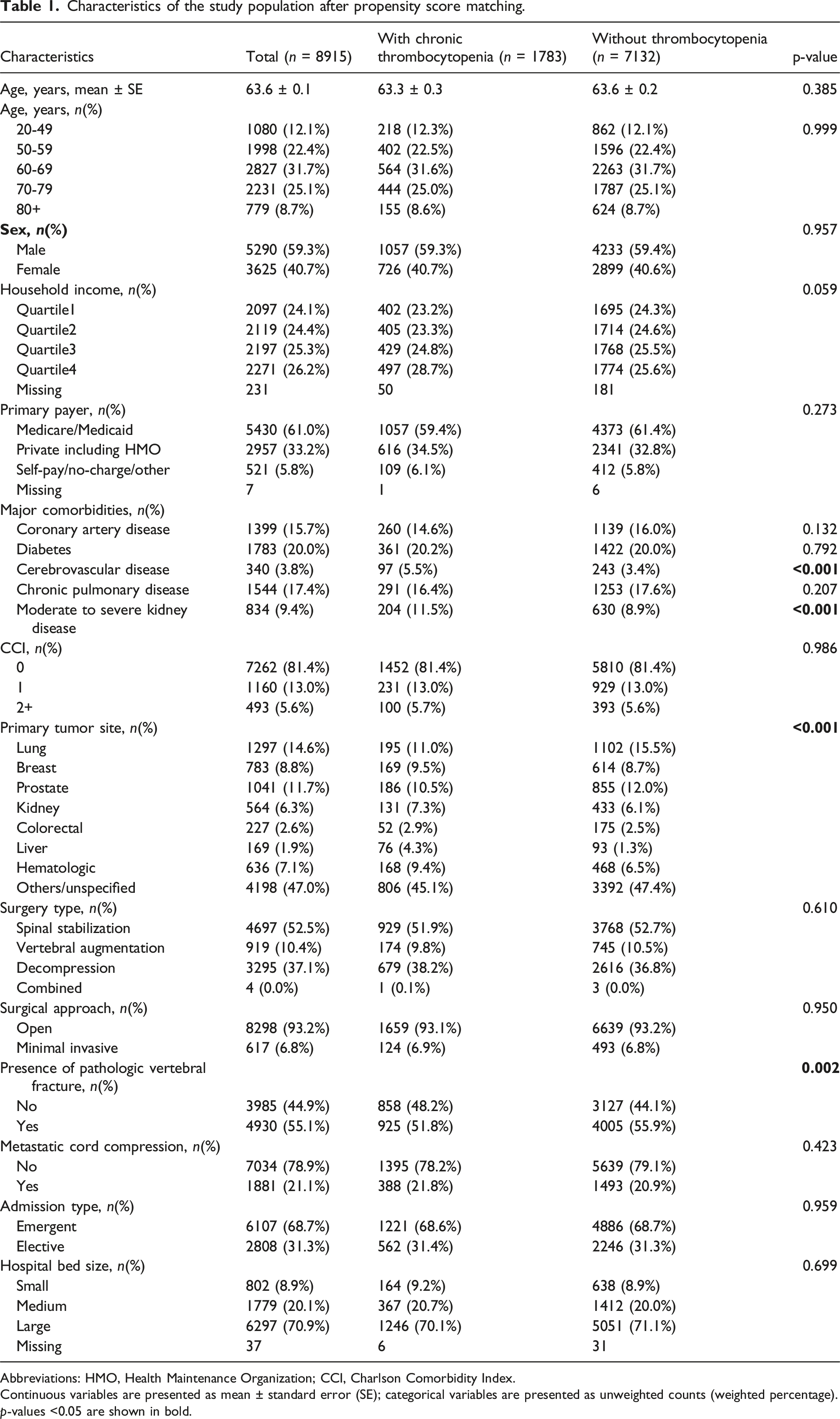
Abbreviations: HMO, Health Maintenance Organization; CCI, Charlson Comorbidity Index.
Continuous variables are presented as mean ± standard error (SE); categorical variables are presented as unweighted counts (weighted percentage).
p-values <0.05 are shown in bold.
In-hospital outcomes
Outcomes after propensity score matching.

Abbreviations: LOS, length of hospital stay; ARDS, acute respiratory distress syndrome; AKI, acute kidney injury; VTE, venous thromboembolism.
Continuous variables are presented as mean ± SE; categorical variables are presented as unweighted counts (weighted percentage).
aExcluding patients who died in the hospital.
bLOS ≥13 days.
p-values <0.05 are shown in bold.
Associations between chronic thrombocytopenia status and in-hospital outcomes
Associations between chronic thrombocytopenia (vs without thrombocytopenia) and outcomes.

Abbreviations: LOS, length of hospital stay; CCI, Charlson Comorbidity Index; OR, odds ratio; aOR, adjusted odds ratio; CI, confidence interval.
p-values <0.05 are shown in bold.
aAdjusted for cerebrovascular disease, moderate to severe kidney disease, CCI, primary tumor site, surgery type, presence of pathologic vertebral fracture, metastatic cord compression, and admission type.
bAdjusted for age group, household income, primary payer, diabetes, cerebrovascular disease, chronic pulmonary disease, moderate to severe kidney disease, CCI, primary tumor site, metastatic cord compression, admission type, and hospital bed size.
cLOS ≥13 days.
dExcluding patients who died in the hospital.
eAdjusted for age group, primary payer, coronary artery disease, diabetes, cerebrovascular disease, chronic pulmonary disease, moderate to severe kidney disease, CCI, primary tumor site, surgery type, presence of pathologic vertebral fracture, metastatic cord compression, admission type, and hospital bed size.
fAdjusted for age group, sex, primary payer, coronary artery disease, diabetes, cerebrovascular disease, moderate to severe kidney disease, CCI, primary tumor site, surgery type, surgical approach, presence of pathologic vertebral fracture, metastatic cord compression, admission type, and hospital bed size.
Associations between chronic thrombocytopenia and specific perioperative complications
Figure 2 shows the associations between chronic thrombocytopenia and individual complications through the multivariable analyses. Compared to patients without chronic thrombocytopenia, those with chronic thrombocytopenia had significantly increased risks of ARDS/respiratory failure (aOR = 2.49, 95% CI: 2.14-2.90), tracheostomy/mechanical ventilation (aOR = 2.49, 95% CI: 2.09-2.97), AKI (aOR = 1.71, 95% CI: 1.44-2.04), VTE (aOR = 1.87, 95% CI: 1.56-2.24), transfusion (aOR = 2.41, 95% CI: 2.13-2.71), acute postoperative hemorrhagic anemia (aOR = 2.44, 95% CI: 2.15-2.76), hematoma/seroma (aOR = 2.13, 95% CI: 1.63-2.80), shock (aOR = 2.74, 95% CI: 2.06-3.65), and sepsis (aOR = 1.56, 95% CI: 1.34-1.81). Association between chronic thrombocytopenia and specific complications Abbreviations: CCI, Charlson Comorbidity Index; aOR, adjusted odds ratio; CI, confidence interval. Adjusted for age group, sex, primary payer, coronary artery disease, diabetes, cerebrovascular disease, moderate to severe kidney disease, CCI, primary tumor site, surgery type, surgical approach, presence of pathologic vertebral fracture, metastatic cord compression, admission type, and hospital bed size.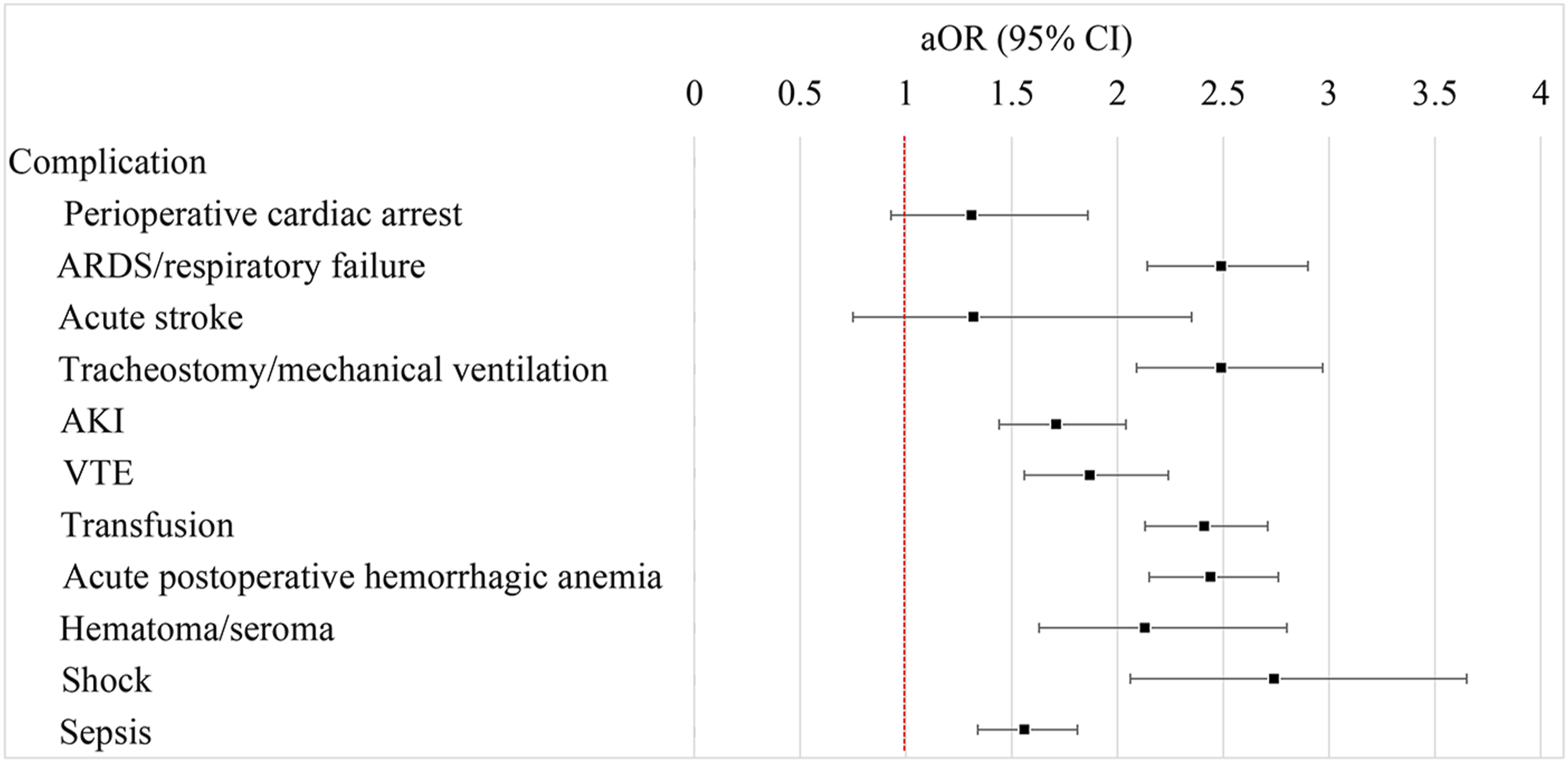
Discussion
This study examined the impact of chronic thrombocytopenia on surgical outcomes for metastatic spinal tumors using a nationally representative database. Patients with chronic thrombocytopenia undergoing surgery for metastatic spinal tumors were found to have significantly elevated risks of various in-hospital outcomes, including more than 2-fold increased risk of mortality, a 3-fold increased risk of overall perioperative complications, as well as increased risk of unfavorable discharge and prolonged LOS. In addition to expected postoperative hemorrhagic anemia, need for transfusion, and perioperative shock, the presence of comorbid chronic thrombocytopenia is also predictive of the occurrence of ARDS/ respiratory failure and tracheostomy/mechanical ventilation (2.5-fold), AKI (1.7-fold), and sepsis (1.6-fold). These findings highlight the critical necessity for vigilant screening of chronic thrombocytopenia in patients undergoing surgery for metastatic spinal tumors to optimize surgical and postoperative outcomes.
While few studies have specifically examined the effect of thrombocytopenia on outcomes after surgery for spinal metastases, existing literature suggests a broader impact of thrombocytopenia on surgical outcomes. It has been associated with increased risks of mortality and complications in various surgical procedures, including cardiac surgeries,15,19 orthopedic procedures such as THA and TKA,15,20 general surgical procedures,10,21 as well as short- and long-term outcomes after cancer-directed surgeries.
In another study of elective spine surgery by studying a population from a multicenter registry, Murphy et al. 22 reported that, among other factors, thrombocytopenia was a risk factor for dural tears. Surgeons are concerned about perioperative blood loss in oncological spine surgery. A previous study documented that factors such as tumor histology, procedure length, Epidural Spinal Cord Compression (ESCC) score, tumor localization, BMI, and surgical strategy significantly impact intraoperative blood loss and transfusion needs; whereas the anesthesiological parameters like the American Society of Anesthesiologists (ASA) Physical Status classification score do not. 23 Our analysis adds to the literature, emphasizing that chronic thrombocytopenia is a strong outcome predictor that increases risks for transfusion, hemorrhagic anemia, hematoma, and seroma. Yet, the causality of this relationship remains unclear, underscoring the need for further validation through prospective studies.
The study by Ansari et al., 7 analyzing 3574 patients undergoing extradural spine tumor resection, highlighted the significant correlation between preoperative thrombocytopenia and increased risks of perioperative transfusions, cardiac complications, non-home discharge, and 30-day mortality. However, it did not distinguish between acute and chronic thrombocytopenia or assess respiratory complications, kidney injury, infections, sepsis, or shock. Our study, with over double the cohort size, focuses on chronic thrombocytopenia and reveals novel associations with sepsis and respiratory issues. Additionally, we accounted for comorbidities, tumor site, vertebral fractures, cord compression, and hospital characteristics, enhancing our findings’ reliability.
Interestingly, according to our analyses, chronic thrombocytopenia is significantly associated with elevated risks of severe postoperative complications, including ARDS/respiratory failure, tracheostomy/mechanical ventilation, AKI, shock, and sepsis. Chronic thrombocytopenia indicates a compromised physiological state, increasing vulnerability to infections and inflammation, 24 thus raising sepsis risk. Reduced clotting ability leads to significant blood loss, decreasing oxygen delivery to vital organs and causing end-organ dysfunctions. In the lungs, this may result in ARDS, requiring mechanical ventilation, while in the kidneys, it leads to AKI due to decreased oxygen supply and blood volume. 25 These interpretations remain speculative and require further validation.
Clinical implications
The findings of this study underscore the critical need for rigorous screening and management of chronic thrombocytopenia in patients undergoing surgery for metastatic spinal tumors. Chronic thrombocytopenia significantly predicts adverse outcomes, including increased mortality, complications, and extended hospital stays, necessitating vigilant clinical monitoring. Proactively identifying and addressing thrombocytopenia can guide the adjustment of surgical plans and postoperative care strategies, potentially mitigating risks and improving patient outcomes. Furthermore, a multidisciplinary approach involving collaboration between hematologists, oncologists, and surgeons to optimize patient care should be considered in the overall management of patients with metastatic spinal conditions, particularly those with underlying hematological issues.
Although routine preoperative screening for thrombocytopenia is standard practice in surgical planning, the specific implications of chronic thrombocytopenia in metastatic spinal tumor surgery remain underexplored. The study findings indicate that chronic thrombocytopenia significantly increases the risk of perioperative complications, including non-hematologic complications that are less frequently discussed in the literature, such as respiratory failure and sepsis. While transfusion thresholds for thrombocytopenia in spine surgery remain debated, current guidelines generally recommend maintaining a platelet count above 50,000/µL for major non-neuraxial surgeries and above 100,000/µL for surgeries involving the central nervous system or posterior eye. 26 However, specific recommendations for instrumented spine surgery are not well-established, and further research is needed to determine optimal transfusion thresholds in this context.
Strengths and limitations
This is the largest study focused on this topic, analyzing data from a substantial, nationally representative sample that provides generalizable estimates of the inpatient chronic thrombocytopenia prevalence and its impact on surgeries for metastatic spinal tumors in the US population. Despite its strengths, the study faces several limitations.
First, as a retrospective study, the level of evidence is inherently low, and the analyses demonstrate associations rather than causation between chronic thrombocytopenia and adverse perioperative outcomes. Although strong predictive links were identified, the underlying pathophysiology remains speculative.
Second, similar to previous studies using ICD codes, there are risks of coding errors that could affect the accuracy of the data. Miscoding of diagnostic and procedural records in the database may lead to underestimations or overestimations of chronic thrombocytopenia cases or complications. Moreover, the validity of the ICD codes used to identify chronic thrombocytopenia has not been fully established, as there are no validation studies assessing their sensitivity or positive predictive value (PPV), which may introduce bias in the classification of the exposure variable.
Third, the administrative nature of the NIS database means it inherently lacks the clinical granularity required for a detailed analysis. For example, specific laboratory values, such as preoperative and postoperative platelet counts, the severity of thrombocytopenia, and detailed surgical information like operative time and estimated blood loss, are unavailable. Additionally, key hematologic parameters, including marrow suppression, chemotherapy-induced thrombocytopenia, and marrow replacement therapy, are unavailable. Clinical details, such as primary tumor site, chemotherapy regimens, and the extent of tumor resection, are not recorded, further limiting the depth of our findings.
Finally, the study lacks long-term follow-up, readmission rates, post-discharge survival data, and patient quality of life metrics, limiting a more comprehensive analysis.
Conclusions
This study highlights the significant impact of chronic thrombocytopenia on short-term outcomes in patients undergoing surgery for metastatic spinal tumors. Specifically, these patients experience higher in-hospital mortality, increased rates of non-routine discharge, prolonged hospitalization, and greater perioperative complication risks, particularly shock and respiratory failure. Our findings contribute to the limited literature on the association between chronic thrombocytopenia and surgical outcomes in spinal tumor patients, emphasizing the need for rigorous preoperative screening and risk assessment in this high-risk population. For patients with chronic thrombocytopenia who must undergo urgent spinal surgery, prompt hematology consultation and platelet transfusion are advised to mitigate bleeding risk. Future research should focus on evaluating preoperative transfusion thresholds, optimal transfusion timing, and other perioperative management strategies to mitigate thrombocytopenia-related complications.
Supplemental Material
Supplemental Material - Chronic thrombocytopenia and outcomes following surgery for metastatic spinal tumors: An analysis of the United States Nationwide Inpatient Sample 2005–2018
Supplemental Material for Chronic thrombocytopenia and outcomes following surgery for metastatic spinal tumors: An analysis of the United States Nationwide Inpatient Sample 2005–2018 by Yu-Tse Liu, Ting-Wei Chang, Cheng-Chi Lee, Ching-Chang Chen, Chun-Ting Chen, Mun-Chun Yeap, Yu-Chi Wang in Journal of Orthopaedic Surgery
Footnotes
Ethical considerations
This retrospective study was population-based, and complied with the terms of the NIS data-use agreement. The data utilized in this study were obtained through the Online HCUP Central Distributor. Given that this study solely involved the analysis of secondary data, there was no direct involvement of the general public or patients.
Author Contributions
Conceptualization: Yu-Tse Liu, Ting-Wei Chang, Yu-Chi Wang
Data curation: Yu-Tse Liu
Formal Analysis: Ting-Wei Chang
Funding acquisition: Mun-Chun Yeap
Investigation: Ching-Chang Chen
Methodology: Ting-Wei Chang
Project administration: Mun-Chun Yeap
Resources: Yu-Tse Liu, Ting-Wei Chang
Software: Cheng-Chi Lee
Supervision: Ching-Chang Chen
Validation: Ching-Chang Chen
Visualization: Chun-Ting Chen
Writing – original draft: Yu-Tse Liu
Writing – review & editing: Yu-Chi Wang
All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
All of the data supporting underlying findings are included in the manuscript and its supplemental files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.