
Abstract
Introduction
Mental disorders are among the leading causes of the global health-related burden. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019 showed that the two most disabling mental disorders were depressive and anxiety disorders, which increased disability-adjusted life-years (DALYs). In 2019, anxiety and depression ranked among the top 25 leading causes of burden worldwide1,2 and nearly 301.4 and 279.6 million individuals worldwide were separately influenced by anxiety and depression disorders. 2
To our knowledge, several studies have identified that anxiety and depression present as adverse prognosticators in lumbar spine surgery (LSS), 3 in association with multiple negative outcomes, particularly concerning factors including the length of stay (LOS), life quality, patient satisfaction, and disability.3–6 Moreover, psychological stress had an immunosuppressive impact that may cause an increased risk for postoperative complications, 5 and the risk factors for anxiety and depression after LSS were observed. 7 Connell et al. 8 have described that depression particularly increased opioid use in those who underwent lumbar interbody fusion procedures. Tuomainen et al. 9 concluded that patients with lumbar spinal stenosis could suffer from heightened risks of disability and postoperative pain even if their depressive symptoms elevated slightly. 9 Along with depression, the presence of preoperatively trait anxiety has been identified to be the main determinant of postoperative pain in LSS patients. 10 However, some research shows that preoperative psychological disorders do not worsen adverse reactions following LSS surgery, drawing conflicting conclusions.11–13 Besides, limited studies, especially without a large sample study, have thoroughly examined the postoperative outcomes of patients with either preexisted anxiety or depression,6,7,9 and relatively few indicators of postoperative pain and complications in lumbar surgery were included, leaving with their potential risks underestimated.5,9,14
Therefore, with the use of a nationwide database, we aimed to investigate the following concerns: (1) the occurrence of anxiety or depression in patients undergoing LSS; (2) their influence on postoperative outcomes; and (3) whether anxiety and depression acted as independent risk factors for postoperative complications and pain episodes after LSS.
Methods
Data source
The Healthcare Utilization Project (HCUP) is a collection of databases supported by the Agency for Healthcare Research and Quality (AHRQ), which supplies the most extensive source of hospital data in the United States. In this research, data was collected through the National Inpatient Sample (NIS) database from 2010 to 2019, the most massive all-payer database of inpatient hospitalizations operated by HUCP and publicly available in the United States.
Research sample
As illustrated in Supplemental materials, inclusion criteria contained patients who underwent lumbar discectomy, decompression surgery, fusion surgery, or laminectomy. Individuals with mania, schizophrenia, and those with missing data were excluded. Patients undergoing LSS from 2010 to 2019 and patients with anxiety disorders were identified based on the International Classification of Diseases, Ninth and Tenth Revision, Clinical Modification (ICD-9 and ICD-10) procedure codes. According to the definition of anxiety and depression in the clinical classification software 2015 of HCUP and data elements of AHRQ respectively, those identified populations were then divided into four groups: LSS patients diagnosed with (1) anxiety, (2) depression, (3) both, or (4) neither anxiety nor depression.
Statistical analysis
A retrospective cohort study was conducted. Patient demographics, hospital characteristics, comorbidities and postoperative complications, and inpatient outcomes were investigated. A Chi-squared test was conducted to assess categorical variables, including the age group, gender, race, type of admission, hospital location and bed size, type of hospital, comorbidities, and postoperative complications. On the other hand, the rank sum test, the Student-Newman-Keuls test (SNK), the least significant difference test (LSD), as well as the Bonferroni test were conducted to assess continuous variables, including age, length of stay (LOS), costs, and the number of diagnoses and procedures. Moreover, a multiple logistic regression analysis was conducted to identify the potential risk of postoperative complications in patients accompanied by anxiety and depression undergoing LSS. The covariates considered in the multivariate regression included age, sex, race, hospital location, hospital bed size, type of hospital, admission type, and comorbidities listed in Table 3 (excluding depression). The odds ratios (OR) and the 95% confidence intervals (CI) were assessed. p < 0.05 was defined as the level of statistical significance. SPSS version 25 (IBM Corp, Armonk, NY) was employed to perform all statistical analyses.
Results
By excluding the missing data, a total of 832,099 patients undergoing LSS from 2010 to 2019 in the United States were evaluated (Figure 1), including 53,971 (6.49%) of those accompanied by anxiety and 83,913 (10.08%) of those accompanied with depression. There were 41,539 (4.99%) patients diagnosed with both anxiety and depression, while 652,676 (78.44%) patients underwent LSS without the diagnosis of anxiety or depression. Patient demographics, including age, gender, and race, as well as hospital characteristics were summarized in Table 1. The annual morbidities of Table 2 anxiety, depression, and both anxiety and depression in those undergoing LSS from 2010 to 2019 were depicted in Figure 2. The proportion of comorbidities and postoperative complications were presented in Tables 3 and 4, respectively. The prediction effects of anxiety and depression on postoperative complications and negative outcomes were shown in Table 5 and Figure 3. The associations between the above mental disorders and symptoms related to pain in those undergoing LSS were calculated in Tables 6, and 7 as well as Figure 4 recorded the prediction effects of anxiety and depression on pain-related symptoms. ICD-9, international classification of diseases (ninth edition) clinical modification; ICD-10, international classification of diseases (tenth edition) clinical modification; LSS, lumbar spine surgery. Demographics of patients undergoing lumbar spine surgery with a concomitant diagnosis of depression, anxiety, both diagnoses, and none.
a
CI, confidence interval; LSS, lumbar spine surgery; USD, US dollar. a(Y) means there is a difference between positive diagnosis group and no diagnosis group in post hoc test, while (N) means no difference. bThe N values in this row are derived from weighted national discharge estimates based on the unweighted NIS data, in order to estimate the demographics of patients. Morbidity of depression or anxiety or both diagnoses in patients undergoing lumbar spine surgery between 2010 and 2019.
a
aThe values in this table are derived from weighted national discharge estimates based on the unweighted NIS data, in order to estimate the morbidity of patients with or without psychiatric diseases (depression or anxiety). Morbidity of depression (orange bars), anxiety (red bars), and both diagnoses (green bars) in patients receiving lumbar spine surgery between 2010 and 2019. Morbidity of comorbidities in patients undergoing lumbar spine surgery with a concomitant diagnosis of depression, anxiety, both diagnoses, and none.
a
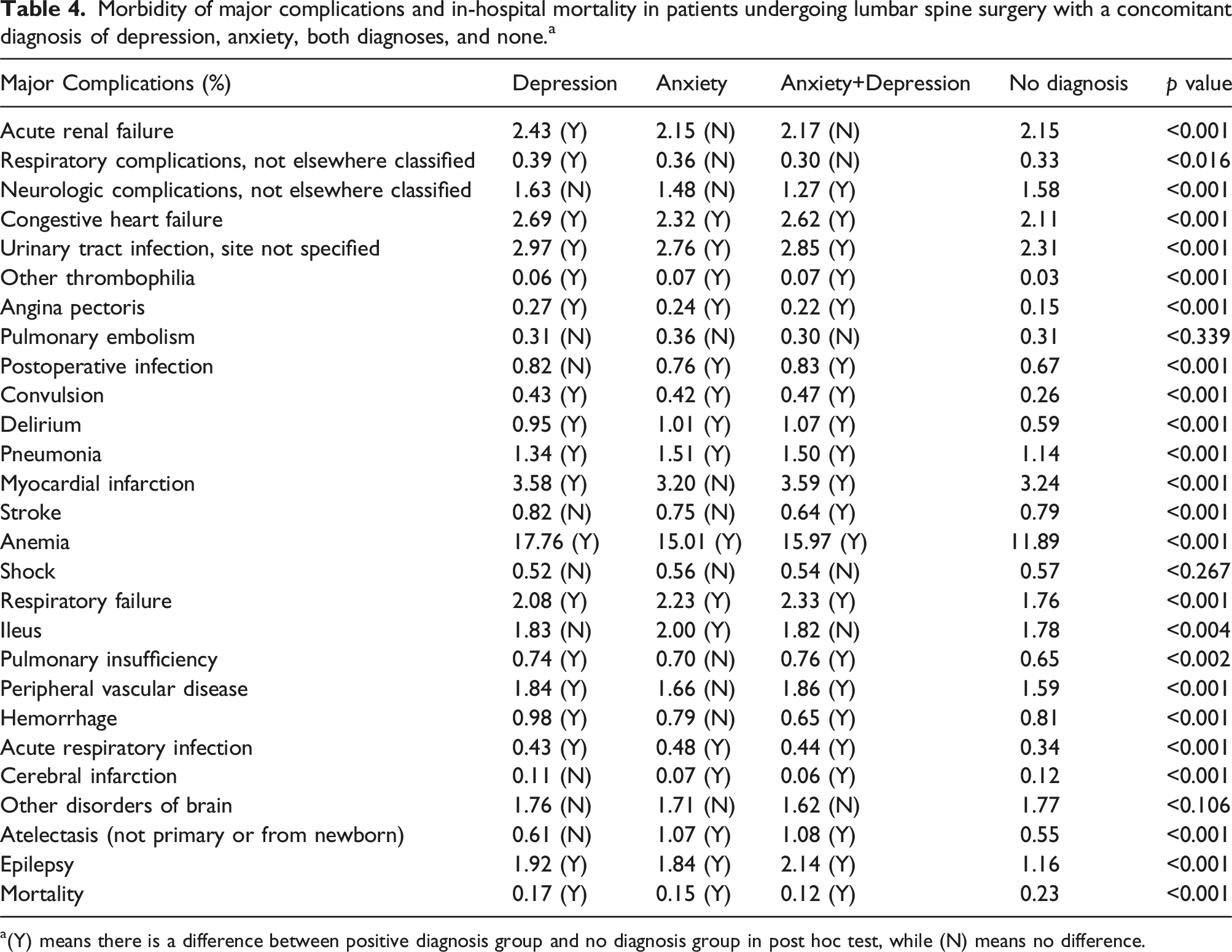
a(Y) means there is a difference between positive diagnosis group and no diagnosis group in post hoc test, while (N). Morbidity of major complications and in-hospital mortality in patients undergoing lumbar spine surgery with a concomitant diagnosis of depression, anxiety, both diagnoses, and none.
a
a(Y) means there is a difference between positive diagnosis group and no diagnosis group in post hoc test, while (N) means no difference. Binary regression results of major complications, LOS, and total charge.
a
CI, confidence interval; LOS, length of stay; OR, odds ratio. aValues in this table were performed by no diagnosis group as a reference. Odds ratios (horizontal axis) for major complications. (The horizontal bars represent the 95% confidence intervals). Morbidity of symptoms related to pain in patients undergoing lumbar spine surgery with a concomitant diagnosis of depression, anxiety, both diagnoses, and none.
a
a(Y) means there is a difference between positive diagnosis group and no diagnosis group in post hoc test, while (N) means no difference. Binary regression results of pain-related symptoms.
a
OR, odds ratio; CI, confidence interval. aValues in this table were performed by no diagnosis group as a reference. Odds ratios (horizontal axis) for pain-related symptoms. (The horizontal bars represent the 95% confidence intervals).









The morbidity of anxiety and depression
As presented in Figure 2, the morbidity of depression was decreasing from 12.35% to 8.77% during this period. However, the morbidity of anxiety kept elevating from 4.10% to 9.49%, and the population accompanied with both anxiety and depression were taking up a larger proportion.
Inpatient outcomes
Notably, LSS patients experiencing anxiety and depression were identified to incur significantly higher medical costs ($76,840, $85,375, $88,542, and $73,899 in the depression, anxiety, comorbid group, and no diagnosis respectively, p < 0.001). Furthermore, patients presenting with either anxiety or depression, and particularly those with both conditions, were demonstrated a higher frequency of diagnoses, recording 10, 10, and 12 diagnoses in the depression, anxiety, and comorbid group, respectively (p < 0.001). Additionally, the LOS and number of procedures were both observed to be notably associated with the aforementioned mental disorders. However, the average duration of hospitalization and numbers of diagnoses remained consistent across these groups.
Individuals undergoing LSS with either anxiety (OR = 0.71, 95%CI 0.56-0.89, p < 0.001) or depression (OR = 0.75, 95%CI 0.63-0.90, p < 0.003), along with those experiencing comorbid conditions (OR = 0.63, 95%CI 0.47-0.84, p < 0.001) appeared to face reduced risks of inpatient mortality. Moreover, patients with anxiety, as well as those with both conditions, exhibited approximately 1.2 to 1.3 times increased likelihood of prolonged hospital stay and higher medical costs. Notably, despite those with depression presenting 1.17 times increased likelihood of longer LOS, depression was not considered as an independent risk factor for elevated medical costs.
Comorbidities
Remarkably, aside from lymphoma and solid tumors without metastasis, notable distinctions in comorbidities were observed between individuals with either anxiety or depression and those without such conditions. Among the delineated comorbidities, a significantly higher prevalence was observed in the anxiety or depression population and the comorbid group for conditions including acquired immunodeficiency syndrome (AIDS), alcohol abuse, deficiency anemia, rheumatoid arthritis and collagen vascular diseases (RA/CVD), congestive heart failure (CHF), chronic pulmonary disease (CPD), coagulopathy, diabetes, drug abuse, hypertension, hypothyroidism, liver disease, fluid and electrolyte disorders, neurologic disorders, obesity, peptic ulcer disease without bleeding, and valvular disease (p < 0.001). Additionally, patients with chronic blood loss anemia, peripheral vascular disorders, pulmonary circulation disorders (PCD), and renal failure were found to constitute a notably larger proportion exclusively in the depression group (p < 0.001). Conversely, patients with paralysis or psychoses comprised a smaller proportion in the depression and comorbid group, while those with metastatic cancer constituted a diminished proportion in the depression group (p < 0.001). Moreover, a markedly higher prevalence of psychoses was detected in the anxiety group (p < 0.001).
Postoperative complications
As shown in Table 4, individuals with either anxiety or depression, and the comorbid group were associated with multiple postoperative complications. According to the logistic regression analysis (Table 5), patients with anxiety emerged as independent risk factors of thrombophilia (OR = 1.82, 95% CI 1.27-2.60, p < 0.002), atelectasis (OR = 1.74, 95% CI 1.59-1.90, p < 0.001), delirium (OR = 1.54, 95% CI 1.40-1.70, p < 0.001), angina pectoris (OR = 1.44, 95% CI 1.19-1.75, p < 0.001), acute respiratory infection (ARI, OR = 1.31, 95% CI 1.15-1.50, p < 0.001), pneumonia (OR = 1.22, 95%CI 1.13-1.32, p < 0.001), postoperative anemia (OR = 1.16, 95%CI 1.12-1.20, p < 0.001), epilepsy (OR = 1.14, 95%CI 1.05-1.23, p < 0.002), ileus (OR = 1.12, 95%CI 1.05-1.20, p < 0.002), and respiratory failure (OR = 1.11, 95%CI 1.04-1.19, p < 0.003). On the other hand, individuals with depression served as an independent risk factor of thrombophilia (OR = 1.55, 95%CI 1.13-2.13, p < 0.007), angina pectoris (OR = 1.43, 95%CI 1.22-1.68, p < 0.001), postoperative anemia (OR = 1.38, 95%CI 1.34-1.41, p < 0.001), delirium (OR = 1.37, 95%CI 1.26-1.49, p < 0.001), CHF (OR = 1.15, 95%CI 1.10-1.21, p < 0.001), myocardial infarction (OR = 1.13, 95%CI 1.09-1.18, p < 0.001), and urinary tract infection (UTI, OR = 1.12, 95%CI 1.07-1.17, p < 0.007). Furthermore, besides the complications mentioned above, those undergoing LSS with both anxiety and depression were identified as independent risk factors of convulsion (OR = 1.26, 95%CI 1.08-1.47, p < 0.005), and Peripheral Vascular Disease (PVD) (OR = 1.21, 95%CI 1.06-1.39, p < 0.008), while serving as protective factors of hemorrhage (OR = 0.84, 95%CI 0.74-0.95, p < 0.006).
Pain-related symptoms
According to our results, patients undergoing LSS with either anxiety or depression were found to be associated with heightened prevalence of various pain-related symptoms. In addition, the comorbid group was identified to be associated with heightened generalized pain, whereas those combined with either anxiety or depression showed no statistical significance in this regard.
As outlined in Table 7, individuals with anxiety were at heightened risk of developing pain-related complications after LSS. Notably, pain disorders related to psychological factors exhibited the highest risk (OR = 4.00, 95% CI 2.37-6.74, p < 0.001), followed by chronic pain syndrome (OR = 2.18, 95% CI 2.06-2.30, p < 0.001), migraine or hemicrania (OR = 1.96, 95% CI 1.88-2.05, p < 0.001), whereas lumbago or low back pain (OR = 1.43, 95% CI 1.35-1.52, p < 0.001), and leg pain (OR = 1.33, 95% CI 1.16-1.52, p < 0.001) were associated with the lowest risks. On the other hand, individuals with depression presented the highest risk for migraine or hemicrania (OR = 2.16, 95%CI 2.09-2.24, p < 0.001) and headache (OR = 1.95, 95%CI 1.52-2.52, p < 0.001), followed by chronic pain syndrome (OR = 1.91, 95%CI 1.81-2.01, p < 0.001), other chronic pain (OR = 1.54, 95%CI 1.50-1.58, p < 0.001), abdominal pain (OR = 1.43, 95%CI 1.24-1.65, p < 0.001), other acute postoperative pain (OR = 1.22, 95%CI 1.17-1.28, p < 0.001), and chest pain (OR = 1.17, 95%CI 1.07-1.27, p < 0.001).
Discussion
From 2010 to 2019, our study revealed a consistent upward trend in the occurrence of anxiety disorders, with the morbidity of depression consistently exceeding 8.6% during this period. This trend may be attributed, in part, to the escalating stress of contemporary life. Notably, our analysis yielded intriguing results, indicating that individuals within the three psychological groups exhibited higher ORs for total charges but lower ORs for postoperative in-hospital mortality. This suggests that anxiety and depression might function as protective factors for inpatient mortality. The heightened likelihood of individuals with anxiety and depression interpreting bodily sensations and changes as indicative of a severe illness might be a reason. 15 Additionally, it is plausible that patients diagnosed with anxiety may exhibit heightened health-related concerns compared to their counterparts, leading to increased vigilance and investment in their healthcare. 16 Consequently, such proactive engagement with their health may contribute to improved postoperative outcomes while concurrently escalating hospitalization costs.
Contrary to our expectations, we identified that the coexistence of anxiety and depression might serve as an independent protective factor against respiratory complications. This finding deviates from an earlier study conducted in 1993. 17 Several hypotheses may account for this observed difference. Firstly, the variance in our findings might be attributed to the distinct samples under scrutiny, implying that individuals undergoing LSS may possess physiological conditions distinct from the general population. Secondly, our analysis revealed that the comorbid group exhibited a higher prevalence of alcohol abuse (refer to Table 3), a known risk factor for respiratory illness. 18 At the same time, our data show that smoking is not the cause of the higher incidence of respiratory complications in the depression and anxiety group (refer to Table 1). Notwithstanding, we mitigated this potential confounding factor by incorporating alcohol abuse into our analysis. Nevertheless, to ascertain the intricate relationship between anxiety, depression, their combination, and respiratory complications, further experimental studies are imperative.
Subsequently, our findings revealed elevated ORs for postoperative delirium in patients across the three psychiatric comorbidity groups, indicating that anxiety and depression might be independent risk factors for postoperative delirium in LSS patients. This association may be attributed to depression-induced behavioral inactivity, consequently leading to heightened inflammation in the body—an established factor associated with an increased risk of delirium. 19 Furthermore, our results revealed elevated ORs for angina pectoris, congestive heart failure, other thrombophilia and myocardial infarction among patients across the three psychiatric comorbidity groups. Various pathophysiological mechanisms, such as alterations in hypothalamic-pituitary-adrenal axis regulation, platelet activation, and inflammation, have been proposed to elucidate these relationships. Prior studies have reported that psychological disorders correlate with an augmented risk of cardiovascular diseases.18,20 Additionally, the three psychological illness groups exhibited heightened ORs for pneumonia and UTI, suggesting that both anxiety and depression independently might serve as risk factors for pneumonia and UTI in LSS patients. We posit that this outcome may be linked to decreased or suppressed immunity, as both depression and anxiety are known to exert an immunosuppressive effect. 21
Interestingly, we noticed that pulmonary embolism (PE) was strongly associated with anxiety but not to the other psychiatric disorders. For this result, we provide a possible explanation. To develop venous thromboembolism (VTE), several pathophysiological studies posit that the presence of one or a combination of factors from Virchow’s triad—venous wall injury, stagnation of blood flow, and hypercoagulability—is essential.22,23 Furthermore, stress and an elevated sympathetic nervous system activity can induce an increase in hypercoagulability.24,25 The stress-driven pathophysiological alterations may support the association of anxiety disorders with hypercoagulability. In line with our findings, a previous study has demonstrated a significant correlation between anxiety and the risk of PE. 26 However, in terms of the outcome of depression, we noticed that the statistical results of two retrospective cohort studies showed depression had no significant correlation with the risk of VTE after total hip arthroplasty, and revision total joint arthroplasty.27,28 Their results were similar to ours. Therefore, in future studies, data or cases of LSS patients with long-term follow-up can be designed for further exploration.
Furthermore, heightened susceptibility to anemia among patients with depression was identified in our study, consistent with findings from a previous study. 29 Depressed patients often have unhealthy eating habits that can lead to deficiencies in vitamins such as B12 and folic acid, ultimately contributing to anemia. 30 Additionally, the prevalence of alcohol abuse in the three psychological illness groups was notably higher compared to the control group (refer to Table 3), suggesting that some psychiatric disorders among patients could be attributed to substance use, such as alcohol. Alternatively, some psychiatric patients may use alcohol to relieve psychological distress. Notably, alcohol, the most abused substance, constitutes a significant risk factor for hypertension. 31
Beyond complications, our study highlighted the association between anxiety and depression disorders and postoperative pain. The outcomes revealed a higher prevalence of pain-related symptoms among patients with concurrent psychiatric comorbidities following LSS. Anxiety and depression emerged as independent risk factors for migraine or hemicrania in LSS patients, consistent with previous findings. 32 Furthermore, anxiety, depression, and their combination were identified as independent risk factors for lumbago or low back pain in LSS patients, potentially attributable to mental distress and pressure, as suggested in an earlier review. 33 Additionally, anxiety and depression were identified as independent risk factors for unspecified backache, aligning with prior research, possibly due to a lack of understanding of pain in patients with depression and anxiety, leading to a heightened fear. 34 Worse still, the back pain might induce disability according to a review, 35 which merits more attention and further researches.
Moreover, the study indicated that the three psychological illness groups exhibited significantly greater ORs for chronic pains. These findings align with previous researches.5,36,37 In a longitudinal study by Kroenke et al., an interactive relationship between chronic pain and depression was identified, indicating that the presence of depression could diminish the efficacy of pain therapy. This association can be physiologically explained by the involvement of norepinephrine and serotonin in both the pathophysiology of mood disorders and the gate control mechanism of pain. 38 Moreover, research from Nature Reviews Neurology 39 and the European Heart Journal 40 highlights a strong correlation between multisite chronic pain and an increased risk of dementia. The downstream pathophysiological processes related to chronic pain conditions can significantly impact cardiovascular function, underscoring the importance of preoperative diagnosis of psychiatric comorbidities before LSS procedures. Our ORs of complications and symptoms related to pain further support anxiety as a risk factor for chronic disease in LSS patients, in line with prior studies. 41 Similarly, the ORs of symptoms related to pain from our research underscore that mental diseases can independently contribute to the onset of pain symptoms following LSS. These pains may potentially affect patient satisfaction with LSS and health-related quality of life. 42 Additionally, according to experts, depression has been linked to stimulation of the compensatory anti-inflammatory response system and a low-grade, chronic inflammatory response. Hence, individuals with mental illness should adhere to a balanced diet rich in vegetables, fruits, whole grains, fish, and legumes. This dietary pattern has been linked to lower levels of inflammatory markers such as CRP and IL-6 in the blood. 43 In our research, LSS patients with anxiety and depression demonstrated a higher incidence of postoperative complications, greater burdens of comorbidities, and increased risks for pain, and further studies are imperative. This issue also suggests that physicians should give extra attention to patients with psychiatric disorders when determining their suitability for discharge. 44
Psychological factors, including depression and anxiety, exert not only a discernible impact on treatment success and recovery, 5 but also contribute to prolonged hospital stays, increased hospitalization costs, and elevated risks for postoperative complications and pain-related symptoms. Therefore, medical workers should prioritize the psychological well-being of patients and attach importance to address psychological issues in postoperative recovery. Additionally, mental evaluations before LSS can offer significant benefits for both patients and clinical professionals. Therefore, both clinical practitioners and patients should notice that, with a comprehensive preoperative assessment and management of mental health, the likelihood of preventing postoperative complications and pain-related symptoms increases. Furthermore, according to research, 45 preoperative physical therapy has been found to alleviate postoperative pain and improve mental health, as well as increase postoperative activity levels. Therefore, it is recommended that patients with mental illness undergoing lumbar spine surgery undergo preoperative physical therapy and rehabilitation to mitigate the potential negative impact of postoperative adverse outcomes on their health.
Our study aimed to investigate whether anxiety and depression disorders independently function as risk factors for postoperative complications and pain-related symptoms. In contrast to previous studies, our research transcends geographical limitations and patient quantity constraints, utilizing the extensive NIS database, the largest inpatient database in the United States. This database encompasses categorized collections of patient information from diverse geographic areas and hospital types, minimizing sampling error and enhancing the generalizability of our findings. Furthermore, the decade-long span of patient records enabled us to illustrate comprehensive trends in the morbidities of psychological diseases among LSS patients. Moreover, our study incorporated a rich set of research indices, providing a thorough depiction of the associations between psychological illnesses, postoperative complications, and the occurrence of pain. These findings hold valuable reference value for further clinical trial research and medical treatment practices.
Undoubtedly, our study has some inherent limitations. One notable constraint is the inability to distinguish between codes for preoperative and postoperative anxiety due to the constraints of the NIS database and ICD coding. However, it’s worth noting that anti-anxiety drugs are typically excluded from postoperative care. 7 While this may result in a potential underestimation of the number of patients diagnosed with anxiety immediately after surgery, we consider that the overall impact of postoperative anxiety on this extensive sample study is relatively minimal. Additionally, being a cross-sectional study, we acknowledge that we cannot fully capture the long-term changes and dynamic processes of the population. However, this study used a large sample of data to investigate the influence of psychiatric patients on postoperative complications and pain. The findings offer valuable insights for future research.
Conclusion
In general, our findings suggest that LSS patients with psychiatric disorders, including anxiety, depression, or both, may face elevated risks of postoperative complications and pain episodes, particularly chronic pain, experiencing heavier economic burdens and prolonged hospital stays, but exhibiting lower in-hospital mortality. Orthopedic surgeons need to remain vigilant to this population and further research to investigate their long-term effects and perioperative management are merited.
Supplemental Material
Supplemental Material - Anxiety and depression as risk factors for postoperative complications and pain in lumbar spine surgery: A national database study
Supplemental Material for Anxiety and depression as risk factors for postoperative complications and pain in lumbar spine surgery: A national database study by Ruimin Wu, Pengcheng Gao, Shuxia Liu, Qinfeng Yang, Jian Wang, Fangguo Liang, Yuhang Chen and Lin Yang in Journal of Orthopaedic Surgery.
Supplemental Material
Supplemental Material - Anxiety and depression as risk factors for postoperative complications and pain in lumbar spine surgery: A national database study
Supplemental Material for Anxiety and depression as risk factors for postoperative complications and pain in lumbar spine surgery: A national database study by Ruimin Wu, Pengcheng Gao, Shuxia Liu, Qinfeng Yang, Jian Wang, Fangguo Liang, Yuhang Chen and Lin Yang in Journal of Orthopaedic Surgery.
Footnotes
Author contributions
RW, PG and SL contributed to the study design, data acquisition and analysis, interpretation of results, and writing and revising the manuscript. QY and JW contributed to data acquisition, and data analysis. LY, YC and FL contributed to the study design, interpretation of results, and reviewing the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
This study is based on data provided by Nationwide Inpatient Sample (NIS) database, part of the Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality. The NIS database is a large publicly available full-payer inpatient care database in the United States and the direct web link to the database is ![]() . Therefore, individual or grouped data cannot be shared by the authors.
. Therefore, individual or grouped data cannot be shared by the authors.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.