
Abstract
Background
The occurrence of prosthesis-related complications after total shoulder arthroplasty is devastating and costly. The purpose was to determine the incidence and risk of in-hospital prosthesis-related complications after total shoulder arthroplasty utilizing a large-scale sample database.
Methods
A retrospective database analysis was performed based on Nationwide Inpatient Sample from 2010 to 2014. Patients who underwent total shoulder arthroplasty were included. Patient demographics, hospital characteristics, length of stay, economic indicators, in-hospital mortality, comorbidities, and peri-operative complications were evaluated.
Results
A total of 34,198 cases were capture from the Nationwide Inpatient Sample database. There were 343 cases of in-hospital prosthesis-related complications after total shoulder arthroplasty and the overall incidence was 1%, with a more than 2.5-fold decrease from 2010 to 2014. Dislocation was the most common category among prosthesis-related complications (0.1%). The occurrence of in-hospital prosthesis-related complications was associated with significantly more total charges and slightly longer length of stay while less usage of Medicare. Risk factors of prosthesis-related complications were identified including younger age (<64 years), female, the native American, hospital in the South, alcohol abuse, depression, uncomplicated diabetes, diabetes with chronic complications, fluid and electrolyte disorders, metastatic cancer, neurological disorders, and renal failure. Interestingly, advanced age (≥65 years) and proprietary hospital were found as protective factors. Furthermore, prosthesis-related complications were associated with aseptic necrosis, rheumatoid arthritis, rotator cuff tear arthropathy, Parkinson’s disease, prior shoulder arthroscopy, and blood transfusion.
Conclusions
It is of benefit to study risk factors of prosthesis-related complications following total shoulder arthroplasty to ensure the appropriate management and optimize consequences although a relatively low incidence was identified.
Keywords
Background
Total shoulder arthroplasty (TSA) has been developed into a new stage, where TSA is a reliable optional for reducing shoulder pain and restoring function in patients for whom nonoperative management for glenohumeral arthritis has failed.1–3 In the past decades, the prevalence of TSA and increased from 0.013% in the year 1995 to 0.197% in 2017. 4 Whereas, implant failure and revision total shoulder arthroplasty procedures may occur commonly as a result of prosthesis-related complications (PRCs), such as dislocation, periprosthetic joint infection (PJI), periprosthetic fracture (PPF), and mechanical loosening of prosthetic joint.5,6
PRCs are catastrophic complications that lead to heavy burdens on the patients as well as healthcare system. 4 Early studies have demonstrated that PRCs are associated with severe pain, disability, longer length of stay (LOS), increased rates of readmission, and higher mortality.7,8 Most PRCs will cause revision surgeries. Although great advancements in surgical techniques and implant design these years, the demand for shoulder arthroplasty revision procedures continues to rise. 9 It was estimated that more than 10,000 revision procedures were performed in 2017 in the United State, with a direct medical cost nearly $205 million. 4
The reported incidence of PRCs after TSA are different largely determined by the category and follow-up time of specific adverse events, such as dislocation (0.1%-5.6%), mechanical loosening (0.7%–2.19%), PJI (0.8%–7.27%), and PPF (0.449%–6.99%).10–16 Therefore, with the purpose of optimizing postoperative outcomes and reducing the requirement for revision procedures after TSA, it is imperative to determine preoperatively whether patients are at high risk of early PRCs. Numerous risk factors for the above complications have been reported by prior studies.7,9–13,15–28 Previously reported risk factors for PRCs after TSA include male gender, smoking, renal failure, depression, diabetes, and overall higher Charlson Comorbidity Index were at increased risk of TSA.5,15
However, there is no study currently investigating the incidence and risk factors of the in-hospital PRCs after TSA, based on a large-scale national sample. Consequently, the objective of this study was to investigate the incidence and risk factors of in-hospital PRCs following TSA, using a nationwide database.
Methods
Data source
The data source of this study was from the Nationwide Inpatient Sample (NIS) database, which was conducted by the Healthcare Cost and Utilization Project and sponsored by the Agency for Healthcare Research and Quality. On behalf of the largest all-payer database of hospital admissions in the United States, NIS collects a stratified sample from more than 1000 hospitals, of approximately 20% of the hospitalizations in the United States each year.9,29 The information, including patient demographics (age, sex, and race), hospital characteristics (type of admission and payer, and bedsize, ownership, teaching status, location, and region of hospital), LOS, total charges, in-hospital mortality, preoperative comorbidities, and diagnostic and procedural codes from International Classification of Diseases (ninth revision) Clinical Modification (ICD-9-CM) were provided by this database. This observational study used deidentified publicly available data, hence it was deemed exempt.
Data collection
Prior to 2010, reverse shoulder arthroplasty (RSA) and anatomical TSA shared a common ICD-9-CM procedural codes (81.80).27,30 That is the 2010 years of the NIS database represents the first year that a separate ICD-9-CM procedural code was used to differentiate RSA (81.88) from anatomical TSA (81.80). Besides, data after the year of 2015 were not included as this was when the ICD-10 codes were first used, which may have introduced some unintended heterogeneity.
31
Thus, data of this study was limitedly extracted from NIS database from 2010 to 2014. Patients undergoing anatomical TSA were identified according to ICD-9-CM procedural codes of 81.80 (n = 34,268). In-hospital PRCs were defined by ICD-9-CM diagnostic codes including dislocation (996.42), PJI (996.66/996.67/998.5/998.51/998.59), PPF (996.44), mechanical loosening (996.41/996.43/996.45), and other prosthesis-related complications (996.40/996.46/996.47/996.49/996.77/996.78/996.79). Patients who were less than 18 years old, lacked data of age, had osteomyelitis, or had pathologic fracture of humerus were excluded (n = 70) (Figure 1). Process to screening data.
Variables entered into the logistic regression analysis. Between line 118 and line 119.

Data analysis
All the statistical analyses were performed utilizing the statistical software, R version 3.5.3 (The R Foundation Inc., Auckland, New Zealand). Significant differences between two groups were determined by Wilcoxon rank test for continuous data and chi-square test for categorical data. To identify independent risk factors of PRCs, multivariate logistic regression with the stepwise method was performed. All variables, including demographics, hospital characteristics, type of payer, and comorbidities providing by the NIS, were entered into the regression analysis (Table 1). Univariate and multivariate logistic regression models were constructed to evaluate the association of additional comorbidities or perioperative complications with PRCs. An alpha level of p < .05 represented statistical significance.
Results
Incidence of in-hospital PRCs in patients undergoing TSA
Patient characteristics and outcomes of PRCs after TSA (2010–2014). Between line 151 and 152.

PRCs: prosthetic-related complications; TSA: total shoulder arthroplasty; LOS: length of stay.

Annual incidence of in-hospital prosthesis-related complications following total shoulder arthroplasty. This indicates that the incidence of in-hospital PRCs which include periprosthetic joint infection, mechanical loosening, dislocation, periprosthetic fracture, and others, decreases from 2010 (1.62%) to 2014 (0.59%).

Incidence of specific categories among prosthesis-related complications following total shoulder arthroplasty. This shows that dislocation (0.1%) was the most common PRCs followed by periprosthetic joint infection (0.09%), periprosthetic fracture (0.06%), and mechanical loosening (0.03%) except for the miscellaneous (0.74%).
Patient demographics of two groups
Patients affected by in-hospital PRCs were 2 years younger (66 years vs 68 years) compared to the nonaffected population (p < .0001) (Table 2). Consistently, there was significant difference of the age distribution between the two groups. PRCs after TSA were 12.13% more likely to occurrence among patients younger than 64 years (46.36% vs 34.23%, p < .0001) (Table 2). Meanwhile, a significant difference was detected in races, with the White occupying smaller proportions (87.09% vs 90.38%) while the Native American taking slightly larger proportions (1.32% vs 0.36%) in the PRCs (p = .03) (Table 2). However, no significant difference was observed in genders between two cohorts at our defined level (p = .06) (Table 2).
Hospital characteristics of two groups
It was found that the occurrence of PRCs was more likely in government or private hospital (collapsed category) (36.76% vs 24.76%, p < .0001), however, less likely in voluntary hospital (private, not-for-profit) (41.47% vs 53.32%, p < .0001) and proprietary hospital (private, investor-owned) (10.88% vs 12.01%, p < .0001) (Table 2). In terms of the region of hospital, in-hospital PRCs tended to occur in the South and West, whereas less likely in the Northeast and Midwest or North Central (p = .003) (Table 2). Nevertheless, there was no statistical difference between two groups regarding to type of admission (p = .31), bedsize of hospital (p = .95), teaching status of hospital (p = .69), and location of hospital (p = .12).
Consequences of in-hospital PRCs after TSA
There was statistical significance in the median LOS between two cohorts (2 days vs 2 days; p < .0001) (Table 2). The median LOS was equal, but the interquartile range in the PRCs groups (1 day to 3 days) was still larger than the control group (1 day to 2 days), suggesting that the occurrence of PRCs slightly prolonged hospitalization (Table 2). As expected, PRCs increased medical expenditure despite the slightly longer LOS. There was a significant increase of $7727 in total hospital charges, with the presence of in-hospital PRCs ($56,677 vs $48,950, p < .0001) (Table 2). With regard to the type of payer, the Medicare was observed to occupy a smaller proportion (53.06% vs 64.08%) while Private insurance (34.99% vs 29.62%) and other type (8.75% vs 3.68%) took a larger proportion in the PRCs group (p = .0005) (Table 2). Fortunately, patients undergoing TSA had quite low in-hospital mortality which was not affected by the presence of PRCs (Table 2).
Risk factors of in-hospital PRCs after TSA
Risk factors of PRCs after TSA (2010–2014). Between line 181 and line 182.

PRCs: prosthetic-related complications; TSA: total shoulder arthroplasty; OR: odds ratio; CI: confidence interval.
Only significant comorbidities are presented.
Additional comorbidities and complications associated with in-hospital PRCs after TSA
Additional comorbidities associated with PRCs after TSA (2010–2014). Between line 196 and line 197.
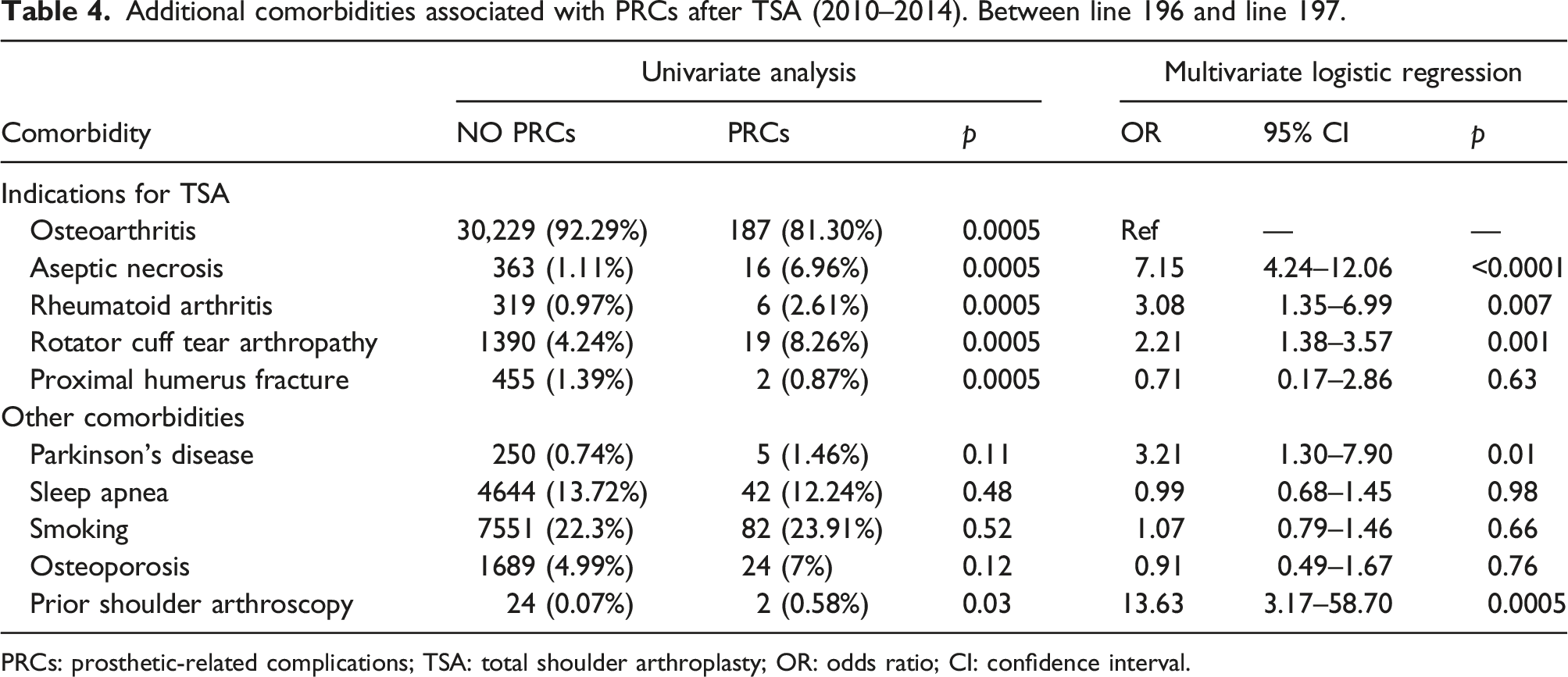
PRCs: prosthetic-related complications; TSA: total shoulder arthroplasty; OR: odds ratio; CI: confidence interval.
Complications associated with PRCs after TSA (2010–2014). Between line 207 and line 208.

PRCs: prosthetic-related complications; TSA: total shoulder arthroplasty; OR: odds ratio; CI: confidence interval.
aAny medical complication: patients with more than one complication are counted only once.
bSurgical complication: patients with more than one complication are counted only once.
Discussion
Analyses of de-identified NIS database data were conducted in this retrospective cohort study. Using the publicly available NIS database, you can accurately estimate 95% of all inpatient treatment in hospitals in the United States based upon a 20% stratified sample of all discharges. The tests for statistical differences were considered to be of little value because of the large sample size and the probability that even small, clinically insignificant differences would have been detected due to the high power associated with the high sample size. The databases were compared by absolute differences, because the magnitude of differences is of greater clinical importance. The present study provides a large-scale as well as health-economic analysis of in-hospital PRCs after TSA. With more attention on improving surgical techniques and component design, the incidence of PRCs following TSA decreased from 2010 to 2014 with an exceeding 2.5-fold reduction (Figure 1). With the introduction of new and clinically relevant ICD-9-CM diagnosis and procedure codes in October 2005, this reduction may have been explained in part by the hospital coders raising awareness of these complications during 2010–2014.38,39 Moreover, with an increase in doctors’ awareness of postoperative prosthesis complications, perioperative management has become more adequate, surgical techniques have become more sophisticated, and prosthesis design has become more rational. As a result of the factors listed above, the incidence of prosthesis complications is decreasing year after year. An overall incidence of 1% of in-hospital PRCs after TSA was firstly identified in this study because previous studies mainly focused on the specific categories of PRCs. Interestingly, this overall incidence of in-hospital PRCs following TSA was lower than that following total hip arthroplasty (THA) (1.96%) while higher than that following total knee arthroplasty (TKA) (0.69%).40,41 It was found that the dislocation of prosthetic joint was the most common PRCs, followed by PJI, PPF, and mechanical loosening (Figure 2), which were to a large extent consistent with the previous studies on implant failure after shoulder arthroplasty.10,14,15,32 Coincidentally, the prior study conducted by our authors found the same results that dislocation was the most common PRCs, followed by PJI, PPF and mechanical loosening after THA. 40 This consistency between TSA and THA reflect the similarity of these two procedures.
A previous literature reported that male was a significant risk factor for revision shoulder arthroplasty, nonetheless in this study, female was identified as a risk factor of PRCs in logistic regression analysis. 6 This disparity may be due to that our study was the analysis of in-hospital PRCs after TSA which was an early stage or even unsure to be the demand of revision. Besides, female patients undergoing shoulder arthroplasty were associated with receiving blood transfusion which was at high risk of PRCs in this study. 27 Furthermore, female was reported to be susceptible to suffer from depression which was also a risk factor of PRCs in our results. 42 Patients with PRCs were 2 years younger than those without. Besides, regarding to age distribution, patients younger than 64 years occupied a greater proportion in the PRCs group. In addition, in logistic regression analysis, advanced age (≥65 years) was identified as a protective factor of PRCs. On the contrary, younger age (<64 years) could statistically be determined as a risk factor of PRCs. To a great extent, this is consistent with previous studies which identified younger age as an independent predictor of PJI, failure or revision after shoulder arthroplasty.5,13,15,17,19,25 The etiology underlying this finding is unclear, but this can be used to educate patients, inform surgeons when counseling younger patients regarding their risks, and serve as an impetus for further investigation. 19 Reasons for the Native American patients more likely and risky to experience PRCs are unknown and likely multifactorial. It is possibly that these minority populations have lower levels of cultural and healthy literacy. Therefore, these patients tend to receive lower-quality care or have difficulty understanding and complying with postoperative instructions.38,43 One possible explanation is that older patients are less mobile than younger patients and further place less cumulative stress on the implant, bone, and soft tissue interfaces over many years, which may lead to less chance of PJI or mechanical loosening. 44 As a potential explanation for reports of PRCs in government or private hospitals, it may be that patients in these facilities with are always challenging with complex comorbidities. A further benefit of these hospitals is that the patients there may have comparatively simple physical conditions, fewer complications, and a better perioperative care experience. 45
Compared with the Northeast region of the United States, hospital in the South was associated with an increased likelihood of PRCs, similar to our prior findings discussing about the PRCs following THA. 40 Combined with the univariate analysis and multivariate analysis, patients in voluntary hospital were less likely and risky to experience PRCs. However, the reasons for these two hospital characteristic remain unclear and require further research.
Both the median LOS was 2 days no matter whether the in-hospital PRCs occurred, which is in line with prior studies that also found an mean LOS of approximate 2 days in patients undergoing TSA.29,35 Although the interquartile range of LOS presented statistical significance between two groups, this small difference was not obvious and might not be clinically important or meaningful. 42 Luckily, the occurrence of in-hospital PRCs after TSA did not incur patients to death in this study, totally unlike to our previous findings in terms of THA and TKA, suggesting that TSA is safer as well as less traumatic to individuals compared with the other two procedures.40,41 Even so, the presence of PRCs still increased total charge during hospitalization, due to the costly treatments and cares of these complications.8,13
To moderate these costly events and further reduce the need for revision, preoperative identification of patients at increased risk of in-hospital PRCs after TSA is essential.46,47 Logistic regression was performed and several risk factors of in-hospital PRCs following TSA were identified (Tables 3–5). Similar to our prior study on PRCs after THA, patients with alcohol abuse were at high risk of PRCs after TSA, probably because excessive alcohol consumption is associated with weakened immune system and mechanisms, impaired phagocytic function, or induced cytokine abnormalities which may have a relationship with PJI.21,40 Depression has previously been reported to be associated with a series of adverse outcomes, such as PJI, sepsis, wound complications, return to the operating room for irrigation and debridement, extended LOS, readmission, revision surgery, and greater health care utilization after TSA, in-hospital PRCs after THA and TKA. 48 Although the relationship between depression and in-hospital PRCs after TSA may seem obscure, imbalance of immune system inducing PJI likely explain this. Psychological distress produces a systemic state of inflammation leading to dysregulation of the immune system and a resultant susceptible host state. 48 Additionally, depression itself may influence T-cell phenotype, and antidepressant medications have been shown to have negative immunoregulatory effects, further causing immune susceptibility. 42
Diabetic patients with vulnerable defenses against bacteria, or impaired wound healing because microangiopathic changes could reduce the tissue concentrations of antibiotics as well as cause local tissue ischemia, consequently are susceptible to PJI, and in-hospital PRCs following TSA, THA and TKA.40,41,49 In concordance with our previous results, metastatic cancer in this study conferred the highest OR value (Table 3). This severe comorbidity possibly predisposes patients to PJI because of immunosuppressive conditions.40,41 Patients with either neurological disorders or Parkinson disease were at increased risk of PRCs likely because of the increased tone of the shoulder girdle musculature, the difficulties with rehabilitation, and stretching of the rotator cuff-capsule arthrotomy site, particularly the rotator interval. 15 Besides, patients with Parkinson’s disease lack complete volitional muscular control and have asynchronous motor function, they appear to place the shoulder at high risk for instability.15,41 Additionally, constant tremors may result in implant loosening, which further increases the dislocation risk. 15 Intriguingly, fluid and electrolyte disorders not only increase the odds of PRCs after THA and TKA, but also had an increased risk of PRCs after TSA.40,41 Renal failure has been reported as a significant risks factor for surgical site infection and revision following TSA.5,8 Patients with these two comorbidities to some degree may reflect the weakened status and insufficient immune function, and hence surgeons should be more cognizant of perioperative nephrotoxic medications, intraoperative hypotensive anesthesia, and postoperative fluid management in this complex patient population. 50
As expected, patients with indications for TSA such as AN, RA, or RCTA had higher odds of PRCs compared with osteoarthritis. Consistently, AN has been associated with a significantly increased risk for postoperative infection, dislocation, fracture, and revision surgery after TSA. 16 Despite our authors previously reported that RA was associated with in-hospital PRCs following THA, it was firstly found in this study that patients RA undergoing TSA were risky to experience in-hospital PRCs. 41 Corticosteroid therapy, alcohol abuse, immunosuppressive conditions, or posttraumatic poor soft tissue bed may partially explain the association of in-hospital PRCs with AN and RA.8,16,17,32,41 Patients with RCTA commonly underwent prior soft tissue mobilization and rotator cuff manipulation, which are thought to affect prosthetic implant stabilization and may play a role in the increased dislocation, infection, and bleeding rates. 25
Arthroscopic intervention for shoulder osteoarthritis has been used as a measure to temporize pain or mechanical symptoms in order to delay joint arthroplasty and expedite time to return to recreational activities and physically demanding jobs. 17 However, it was found that patients with history of PSA were risky to PRCs after TSA, similar to our prior finding that prior knee arthroscopy conferred high risk of PRCs after TKA. 40 Furthermore, PSA has also been reported to be associated with a higher risk of infection after shoulder arthroplasty. 17 On the basis of this association, surgeons should proceed with increased caution before performing an arthroplasty procedure in a patient with a history of PSA, and consider a lower threshold to rule out infection as well as the perioperative usage of antibiotic. 17 It has been shown that blood transfusion confers increased risk of PJI and mechanical complications within 2 years after shoulder arthroplasty and is associated with in-hospital PRCs after THA or TKA.27,40,41 Consistent with previous literatures, blood transfusion was the only one factor in this study significantly associated with in-hospital PRCs following TSA among the perioperative complications. Specifically, allogeneic blood transfusion may have an immunomodulatory effect that may lower the threshold for PJI through several mechanisms.27,41
The main strengths of our study include its large-scale sample and national representativeness with the power to investigate rare events, and the application of multivariable regression modeling to reduce confounding.31,35,40 However, several limitations still require mention, mainly inherent to the use of the NIS database. First, discrepancy or misclassification in the process of coding and documentation may occur as with any large administrative data.16,17,35,40,41 Second, only in-hospital information of each patient is recorded, meaning any complication or outcome that occurs after discharge such as readmission, functional status, and long-term follow-up can not be captured in this database. This limitation may cause underestimating the incidence of PRCs because only early period cases during hospitalization were analyzed.8,9,29,35,38,40,41 Furthermore, only variables provided by the NIS database could be assessed. There are other potential procedural and component characteristics that might influence PRCs were unavailable in the NIS database, such as surgical approach, length of surgery, type of anesthesia, amount of blood loss, cemented or uncemented components, and implant design.7–9,16,40,41,50
Conclusion
In-hospital PRCs are disastrous and costly complications occurring after TSA with a total incidence of 1%. The annual incidence of PRCs decreased from 2010 to 2014 with a surpassing 2.5-fold reduction. Dislocation was the most common PRCs, followed by PJI, PPF, and mechanical loosening. Several risk factors of PRCs after TSA were identified in our study including younger age (<64 years), female, the native American, hospital in the South, alcohol abuse, depression, uncomplicated diabetes, diabetes with chronic complications, fluid and electrolyte disorders, metastatic cancer, neurological disorders, and renal failure. Advanced age (≥65 years) and proprietary hospital were found as protective factors. Meanwhile, the information of implants selection is not available in the NIS database. In addition, PRCs were associated with other indications for TSA (AN, RA, and RCTA), Parkinson’s disease, prior shoulder arthroscopy, and blood transfusion. Patients with PRCs after TSA demonstrated significantly more total charges and slightly longer LOS while less usage of Medicare. Although there are some risk factors that cannot be changed before surgery, For example, younger age (<64 years), female, the native American, hospital in the South, alcohol abuse, depression, neurological disorders and metastatic cancer. To prevent or reduce the occurrence of PRCs following TSA in patients with these conditions, surgeons may be able to counsel patients on informed consent and perform more careful treatment management of high-risk patients with PRCs after TSA during the perioperative period. Additionally, disordered fluid and electrolyte balance, diabetes, and renal insufficiency are risk factors that can be modified, to some extent. Patients with one or more of these comorbidities can be appropriately optimized for better selective TSA, for example, effective managemnet of fluid and electrolyte balance, blood sugar regulation in diabetic patients, hemodialysis for those with renal failure. Consequently, these findings have important and beneficial implications for the treatment of PRCs following TSA.
Supplemental Material
Supplemental Material - Incidence and risk factors of in-hospital prosthesis-related complications following total shoulder arthroplasty
Supplemental Material for Incidence and risk factors of in-hospital prosthesis-related complications following total shoulder arthroplasty by Huishan Lu, Enyou Jin, Hao Xie, Jinlang Fu, Xianhui Chen, Wenqian Liu, Qinfeng Yang and Fang Yu in Journal of Orthopaedic Surgery.
Footnotes
Acknowledgments
We express our sincere gratitude to Goodwill Hessian Health Technology Co. Ltd (100007, Beijing, China.) for providing consultation and guidance on statistical analysis in this study.
Author contributions
H.L. contributed to the study design, data acquisition and analysis, interpretation of results, and writing and revising the manuscript. E.J. and H.X. contributed to the study design, interpretation of results, and reviewing the manuscript. J.F. and X.C. contributed to data acquisition, data analysis, and reviewing of the manuscript. W.L., Q.Y. and Y.F. contributed to the study design, interpretation of results, and reviewing the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.