
Abstract
Introduction
Knee surgery, including total knee arthroplasty (TKA), knee revision surgery, repair or resection of the posterior horn of the meniscus, posterior cruciate ligament (PCL) reconstruction surgery, and high tibial osteotomy, carry the risk of PA injury.1–4 The reported incidence rate of vascular injury in orthopaedic surgery ranges from 0.005% to 0.5%, although the incidence is relatively low,5,6 the potential consequences of such injuries are severe and cannot be underestimated, which may lead to infection or even amputation. 5 The pathological types of PA injury are diverse, among which thrombosis is the most common type of injury, accounting for about 67% of all types, followed by pseudoaneurysm at about 20%, intraoperative bleeding at about 7%, arteriovenous fistula at about 4%, and thrombus blockage and exogenous compression at about 1% each.7–9 Addressing these complications might necessitate vascular resection, vascular bypass procedures, prosthetic revisions, or even limb amputation. 10 Preoperative risk factors associated with vascular injuries during knee surgery encompass pre-existing peripheral vascular conditions like popliteal aneurysms, popliteal artery calcification, 5 and the presence of tumors in proximity to the popliteal artery. 11 A history of prior knee joint surgeries also increases the risk. 12
The causes of PA injury during knee surgery can be attributed to direct arterial injury by surgical instruments, arterial traction and compression, arterial thrombosis, and vascular embolism. 13 Among these, direct injury by surgical instruments is considered the most significant factor. In TKA, instrument-related PA injuries are more likely to occur during specific steps. (1) During tibial osteotomy, when the oscillating saw breaches the posterior joint capsule. (2) During the osteotomy of the posterior femoral condyle, when the oscillating saw penetrates the posterior joint capsule. (3) During the placement of posterior retractors, inadvertently puncturing or compressing the PA. (4) When addressing the posterior horn of the meniscus or the PCL. (5) While removing posterior osteophytes. (6) When the knee joint is overstretched after all osteotomies are complete but before prosthesis placement.13–16 Therefore, a comprehensive understanding of the location and general course of the PA around the knee is crucial for the success and safety of TKA and other knee surgeries.
Presently, research into the PA around the knee joint relies mainly on vascular ultrasound, MRI, and arteriography. Arteriography, while highly informative, is invasive and primarily employed in cadaveric studies. 13 However, the utility of vascular ultrasound is limited due to transducer positioning constraints. In contrast, MRI scans offer superior spatial resolution and clearer visualization of arterial structures, making them a valuable method for evaluating the location and course of the popliteal artery.
This study serves three main objectives. (1) To measure the relative position of the PA in three surgical planes (femoral osteotomy level, articular surface level, and tibial osteotomy level) during knee surgery using knee MRI. (2) To analyze the influence of factors such as age, gender, height, weight, (body mass index) BMI, and leg circumference on the relative position of the PA. (3) To compare and analyze the relative position changes of the PA in patients with osteoarthritis and non-osteoarthritis patients. The significance of this study lies in its potential to prevent PA injuries during knee surgery by precisely locating the PA position through knee MRI, thus improving patient safety and surgical outcomes.
Materials and methods
All participants provided their informed consent, the study was reviewed and approved by The First Hospital of Jilin University Ethics Committee, and all methods involving human subjects were performed out in accordance with the Declaration of Helsinki.
Patient criteria
Baseline patient demographics (N = 172 patients).
The subjects’ legs are shoulder width apart, and the weight is evenly distributed between the legs. The measurer places a tape measure at the transverse crease below the buttocks and measures the circumference horizontally, which is the thigh circumference; and the measurer places a tape measure at the thickest part of the calf and measures the circumference horizontally, which is the calf circumference.
MRI parameters
All patients were placed in supine position, with lower limbs relaxed and knees extended to the maximum extent. The examination equipment was a German SiemensAvanto 1.5T superconducting magnetic resonance scanner, which performed routine Se and FSE sequence scanning. The field of view was 350 mm and the matrix was 256 × 169 mm, T1WI: TR/TE = 520/15 ms, T2WI:TR/TE = 2100/100 ms, T2WI fat suppression sequence: TR/TE = 2100/100 MS, Ti = 155 Ms.
Analyzed factors
This study mainly analyzed the influence of patients’ height, weight, BMI, leg circumference, gender, age and osteoarthritis on PA distance in three levels.
Measurement standard
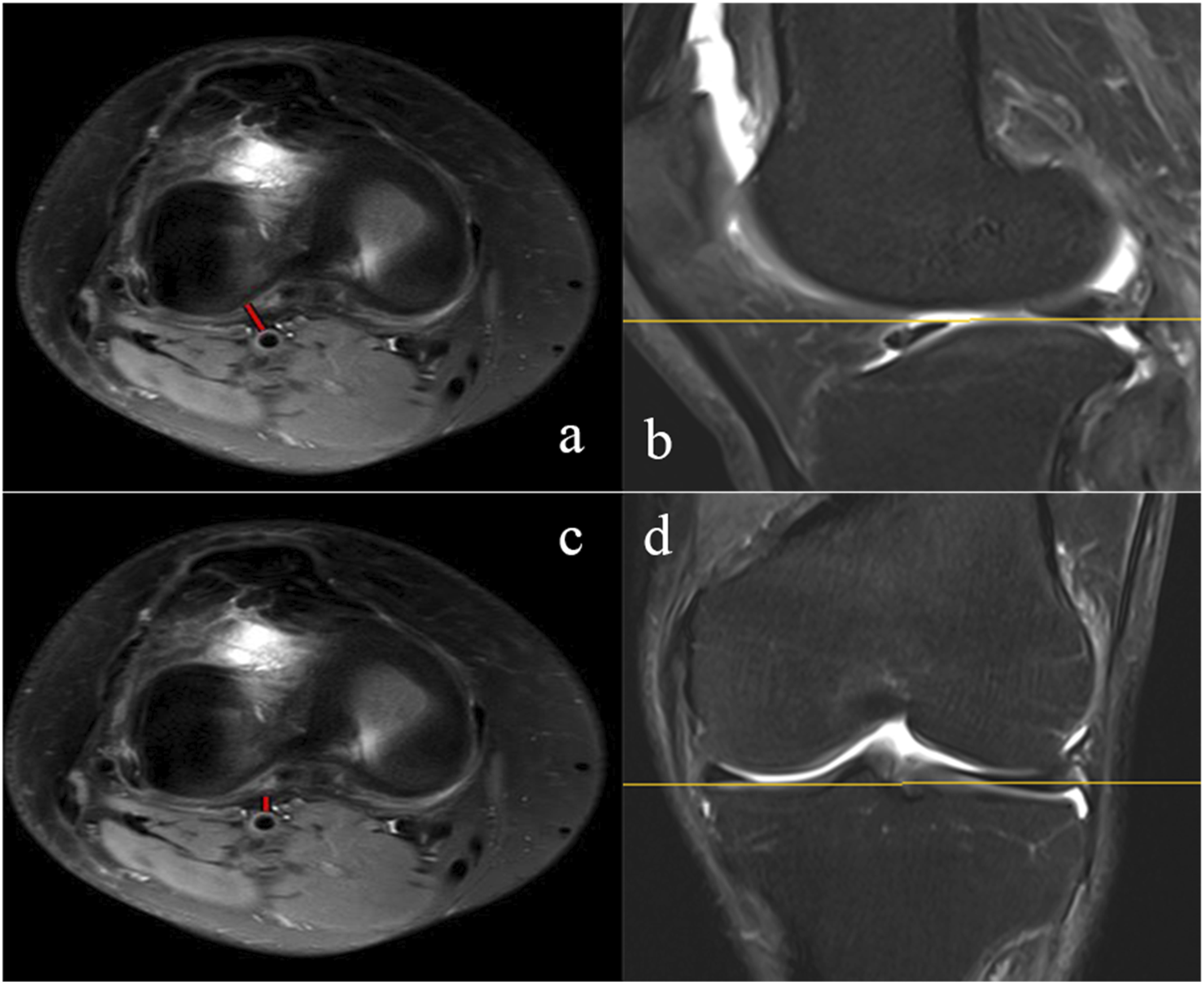
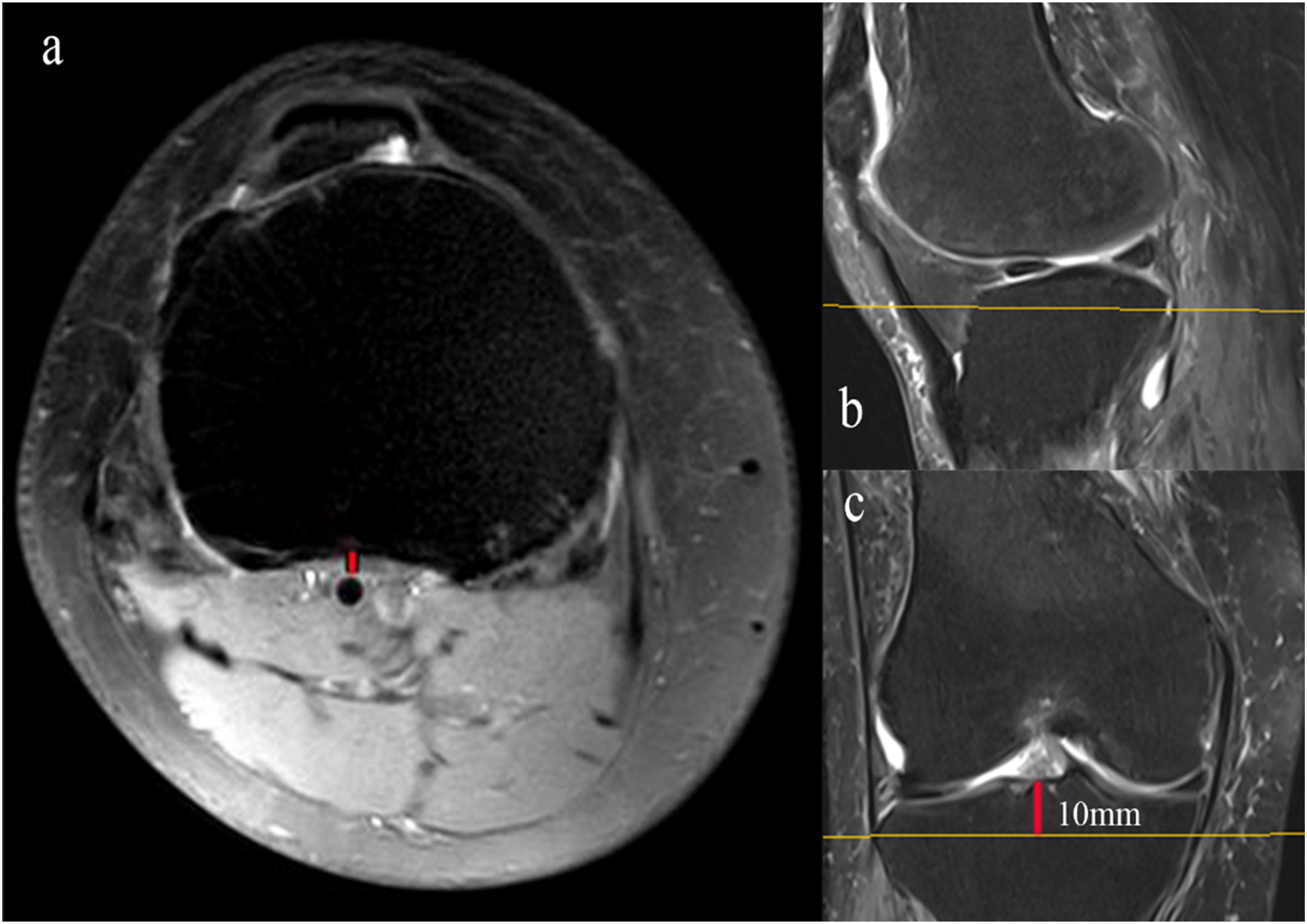
In this study, considering the potential risk of vascular injury during the surgery around knee, we conducted measurements on MRI axial views at three different levels to ascertain the shortest distance from the PA to anatomical landmarks. (1) At the femoral level, we measured the closest distance between the PA and the posterior femoral condyle (PFC). (Figure 1) (2) At the level of the articular surface, we determined the closest distances of the PA from the posterior horn of the lateral meniscus (PHLM) and the posterior wall of the joint capsule (JC). (Figure 2) (3) 10 mm below the articular surface, we measured the closest distance between the PA and the posterior tibial cortex (PTC) (Figure 3). The closest distance between the PA and the PFC (a, red line), at the level of the line connecting the internal and external collateral ligaments in the coronal view (c, yellow line), the anteroposterior diameter of the femoral condyle was the largest in the sagittal view (b, yellow line). (a) axial views. (b) sagittal view. (c) coronal view. The closest distances of the PA from the PHLM (a, red line) and the JC (c, red line) at the level of the articular surface in axial views. (a, c) axial views. (b) sagittal view. (d) coronal view. The closest distance between the PA and the PTC (a, red line) at 10 mm below the articular surface (c, red line). (a) axial views. (b) sagittal view. (c) coronal view.
Data analyses
Graphpad Prism 9.5 was used to analyze the experimental data. Continuous variables were expressed as mean ± SD, which met the normal distribution. The statistical analysis between two groups of data was performed by t test. The comparison between multiple groups of data was performed by one-way analysis of variance. Spearman rank correlation coefficient was used to study the association between any two continuous variables. When p < 0.05, it was considered statistically significant.
Results
The distance between popliteal artery and meaningful landmarks of knee.
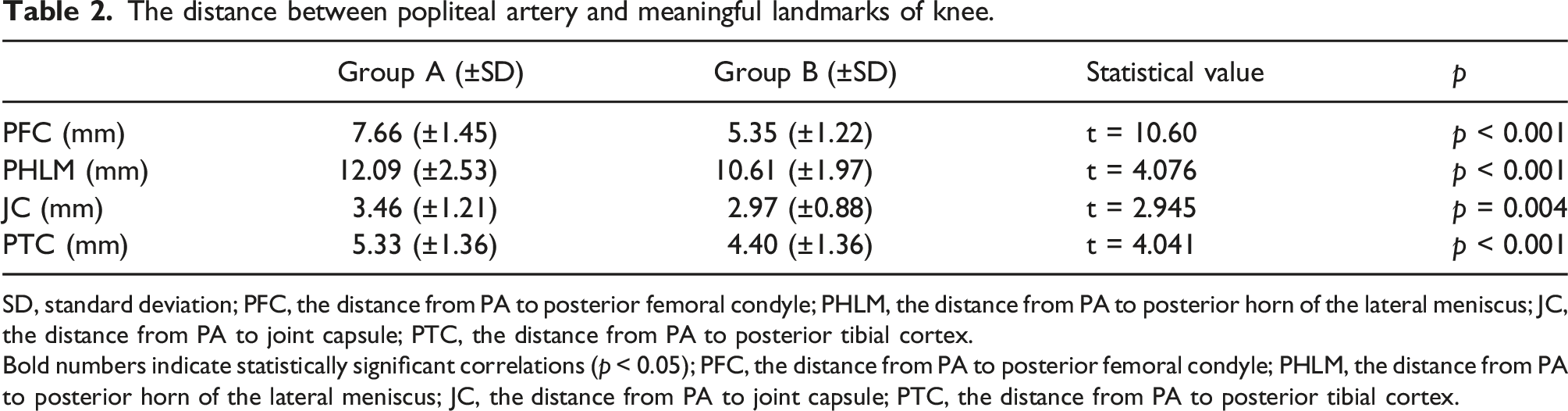
SD, standard deviation; PFC, the distance from PA to posterior femoral condyle; PHLM, the distance from PA to posterior horn of the lateral meniscus; JC, the distance from PA to joint capsule; PTC, the distance from PA to posterior tibial cortex.
Bold numbers indicate statistically significant correlations (p < 0.05); PFC, the distance from PA to posterior femoral condyle; PHLM, the distance from PA to posterior horn of the lateral meniscus; JC, the distance from PA to joint capsule; PTC, the distance from PA to posterior tibial cortex.
Correlations between two variables.
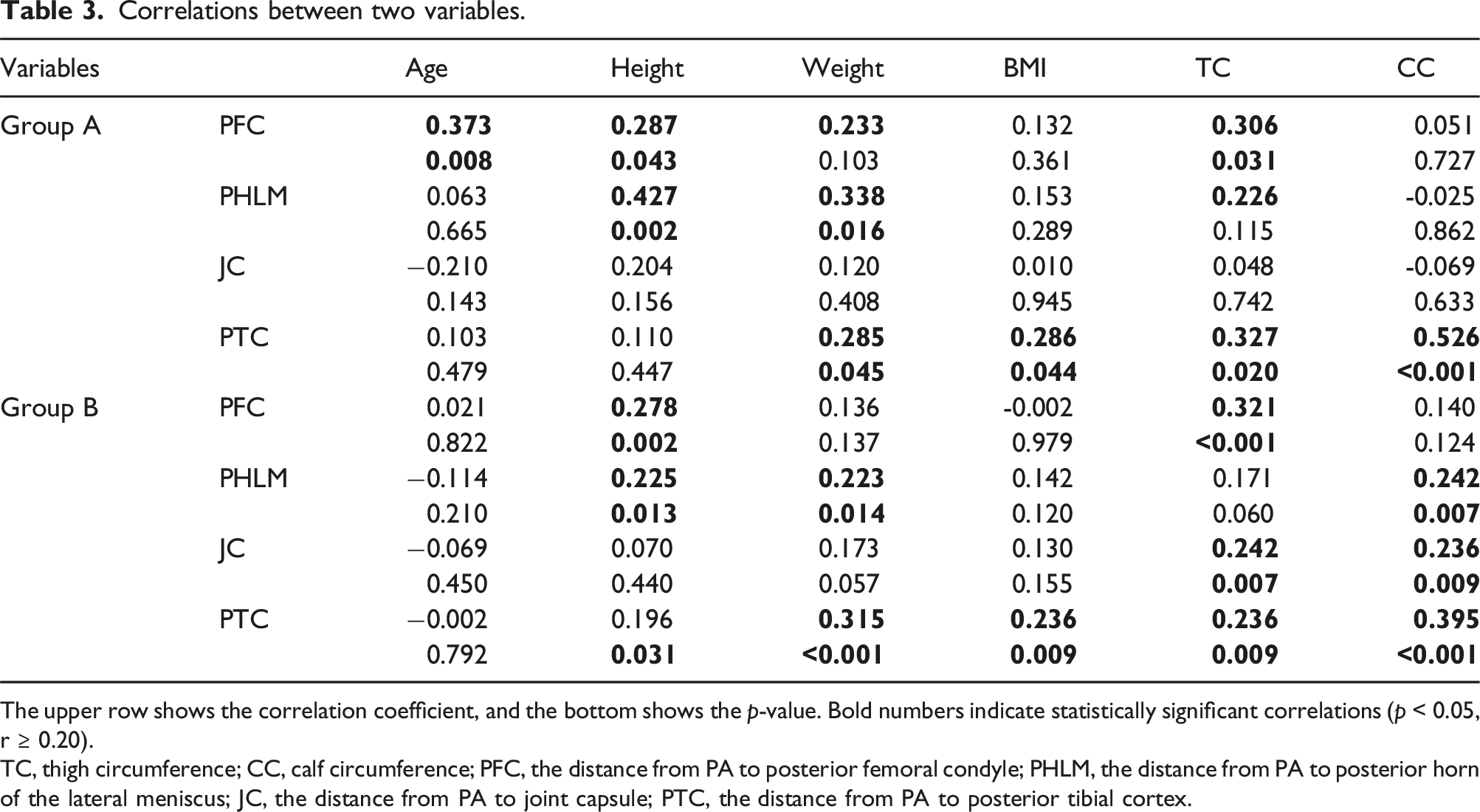
The upper row shows the correlation coefficient, and the bottom shows the p-value. Bold numbers indicate statistically significant correlations (p < 0.05, r ≥ 0.20).
TC, thigh circumference; CC, calf circumference; PFC, the distance from PA to posterior femoral condyle; PHLM, the distance from PA to posterior horn of the lateral meniscus; JC, the distance from PA to joint capsule; PTC, the distance from PA to posterior tibial cortex.
Discussion
The findings of this study have unveiled significant insights into the position of the PA in relation to the knee joint, particularly with regard to patients with osteoarthritis. Additionally, several influencing factors on the PA position were identified, shedding light on their importance in surgical planning. Firstly, it was observed that the distances between the PA and the knee joint were significantly increased in patients with osteoarthritis compared to non-osteoarthritis patients. This suggests that the presence of osteoarthritis is a critical factor influencing the proximity of the PA to the knee joint. For the increase of PA distance in the Group A, we speculate that it may be related to the following points. (1) Bone cortex defect. (2) The soft tissue around the knee joint is hypertrophic and the joint capsule is thickened. (3) Patients with osteoarthritis generally lack exercise, resulting in thickening of the arterial lumen wall.17–19 These factors may become more pronounced with advancing age, which aligns with the positive correlation between age and distance observed in osteoarthritis group. The study also noted that the distance from PA to posterior femoral condyle in both osteoarthritis and non-osteoarthritis patients is positively correlated with age, height, and thigh circumference. Ishii et al. found that the distance between PA and the posterior condyle of the femur is positively correlated with weight, and Chang et al. measured that the distance between PA and the knee joint is positively correlated with thigh circumference, which is consistent with our results.20,21 and imply that individuals with larger bony structures, such as taller individuals, tend to have greater distances from PA to posterior femoral condyle. Similarly, weight, BMI and calf circumference were positively correlated with the distance from PA to posterior tibial cortex, we speculate that the tibial plateau diameter is larger in patients with larger calf circumference, while obese patients have more hypertrophic soft tissue.
Previous studies have suggested that younger patients and female patients have a higher risk of PA injury during knee surgery, which is related to the shorter distance between neurovascular bundle and the bony landmarks behind the knee joint.22,23 We have confirmed this concept through measurements. Besides, we have found that female patients, particularly those with shorter stature, lower weight, and thinner leg circumferences have closer distances from PA to posterior horn of the lateral meniscus, which is a high-risk group for PA injury during knee surgery, especially lateral meniscus surgery. 24
Furthermore, the study discovered that the distances from PA to joint capsule were positively correlated with thigh and calf circumferences in non-osteoarthritis patients but not in osteoarthritis patients. This distinction may be attributed to the thickening of the joint capsule in patients with osteoarthritis, highlighting the importance of considering pathological changes in surgical planning.
Ishii et al reported that PA gradually approaches the posterior aspect of the knee joint from proximal to distal, 20 but we found through actual measurement that on the horizontal plane connecting the termination points of the medial and lateral collateral ligaments, the distance between PA and the posterior lateral condyle of the femur is the closest at the entire femoral segment. And this level is shown by the yellow line on the MRI coronal view. (Figure 1(c)). In the sagittal view, the protrusion of femoral condyle at this level is more pronounced towards the back (Figure 1(b)), which may be the reason for the closest distance. With the gradual downward movement of the PA, the distances between PA and the posterior lateral condyle gradually increase. Therefore, when performing operations near the termination point of the medial and lateral collateral ligaments, such as removing the osteophyte of the posterior condyle or releasing the posterior joint capsule, it is necessary to be alert to the risk of PA injury.
Among the four measured distances, the average distance between PA and the posterior wall of the joint capsule is the shortest, only 2.97 (±0.88) mm in the Non-Osteoarthritis Group. Although this distance has increased in the Osteoarthritis Group, it is only 3.46 (±1.21) mm. Therefore, when operating at the joint surface level, once the posterior joint capsule is penetrated, PA is easily damaged.
There is still no clear answer to whether knee flexion can increase the distance of PA. Ninomiya et al.'s cadaveric study showed that when the knee is in the flexion position, the artery extends backward, thus protecting the PA from direct injury to a certain extent. 13 Oehler, Keyurapan, Farrington, et al. also proved the above point through knee flexion 90° MRI.23,25–27 However, some researchers found through ultrasound that the PA distance did not increase during knee flexion.28–31 It is worth noting that this study did not include the cases involving periarticular masses like Baker’s cysts in the study group. Keser et al. demonstrated that periarticular masses of the knee would affect the location of PA and increase the risk of vascular injury. Surgeons are encouraged to clarify the specific PA route before surgery in such cases. 11
Several limitations of this study should be acknowledged. First of all, the retrospective nature of the study limited the collection of knee MRI data to the knee extension position, while many knee surgeries are performed with the knee in flexion. We will further verify the position change of PA in flexion position. Secondly, limited by the retrospective study, the influencing factors of this study are derived from the hospital database, not measured by the same person, and there may be measurement error. (Each patient undergoing examination in the radiology department will be recorded their basic information such as height, weight, and leg circumference by nurses and uploaded to the hospital database. This task was completed by several nurses, not just one.) Thirdly, the measurement is too theoretical and simple, and there are many factors affecting knee surgery in reality, such as increasing the amount of osteotomy when the tibial plateau defect is large, and reducing the amount of osteotomy in shorter patients, which cannot be fully covered. Fourth, the study’s data was derived from a single hospital, which has regional uniqueness and may limit its generalizability to a broader population.
Conclusion
Our study has the following clinical significance. The distance between the PA and the posterolateral condyle of the femur at the level of the line connecting the internal and external collateral ligaments is the closest distance of the femoral segment, and the surgeon should be cautious when performing surgical operations near this level; The average distance between the PA and the posterior wall of the joint capsule at the level of the articular surface is very short, making it susceptible to PA damage once the joint capsule is breached. Female patients with short stature, light weight and thin leg circumference are at high risk of PA injury; The risk of PA injury in younger patients with osteoarthritis is higher than older patients, and non-osteoarthritis patients have a higher risk of PA injury during knee surgery than osteoarthritis patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jilin Province Development and Reform Commission; 2023C039-4.