
Abstract
Introduction
Arterial injury following total knee arthroplasty (TKA) can be life-threatening. There are some anatomical variations in the popliteal artery (PA) and its branches. In most cases, the PA branches into the anterior tibial artery (ATA) and posterior tibial artery (PTA), which are usually distal to the height of tibial resection in TKA. However, some cases show that the PA branches into the ATA and PTA proximal to the height of tibial resection in TKA. This study aimed to assess the distance from the posterior cortex of the proximal tibia to the anterior wall of the PA or ATA at the height of the tibial cut line, during TKA in the distal and proximal branch groups.
Methods
129 patients (6 patients in the proximal branch group and 123 patients in the distal branch group) were enrolled for this study. For prediction of the distance from the posterior cortex of the proximal tibia to the anterior wall of the PA or ATA, preoperative sagittal and coronal magnetic resonance images and postoperative radiographs were evaluated.
Results
The distance between the posterior cortex of the proximal tibia and the anterior wall of the PA or ATA at the height of the tibial cut line was 1.8 ± 1.1 mm in the proximal branch group and 6.1 ± 2.6 mm in the distal branch group, which was significantly closer in the proximal group (P < .05).
Discussion
The rate of proximal branching was 4.7%. This study clarified that the proximal branching of the ATA from PA significantly decreased the distance between the posterior cortex of the proximal tibia and the anterior wall of the artery.
Conclusions
The proximal branch group has a high risk for arterial injury as the artery may be close to the saw, and appropriate retraction should be performed.
Introduction
Knee osteoarthritis (KOA) is a degenerative joint disease characterized by the progressive erosion of the articular cartilage and one of the most common musculoskeletal diseases in 25,000,000 Japanese patients aged >40 years who have radiographic KOA.1,2 In end-stage KOA, total knee arthroplasty (TKA) alleviates pain and improves activities of daily living 3 ; the retractors and instruments are routinely placed near the posterior capsule of the knee, close to the vessels in TKA. 4 Therefore, neurovascular complications following knee surgery are rare, with an incidence rate between .02% and .05%, which may be underestimated.5,6 However, arterial injury can be a severe complication, with the risk of amputation of the affected limb. 7 The artery runs a course in close relation to the posterior tibial cortex, and the popliteal artery (PA) risks injury during orthopedic procedures. Several studies have focused on anatomic relationships at the level of the knee joint and the effect of the knee flexion angle, in addition to the presence of arthritis. 4
There are anatomical variations in the PA and its branches. In most cases, the PA branches into the anterior tibial artery (ATA) and posterior tibial artery (PTA), usually distal into the height of tibial resection in TKA. Conversely, the PA branches into the ATA and PTA proximal to the size of tibial resection in TKA in some cases. 8 There is a concern that the distance from the proximal tibia’s posterior cortex to the anterior wall of the ATA at the height of the tibial cut line in TKA is smaller than that of the distal branch because the ATA runs anteriorly to the PTA. Based on our recent literature search, no studies clarified how the ATA branching pattern affects the distance from the posterior cortex of the proximal tibia at the height of the tibial cut line to the wall of the artery during TKA. This study aimed to clarify how the branching pattern affected the distance from the posterior cortex of the proximal tibia to the anterior wall of the artery at the height of the tibial cut line during TKA.
Material and Methods
Patient Selection
The Clinical Research Ethics Committee approved this study of our institution (Receipt ID: 20-126). The Clinical Research Ethics Committee waived the requirement for written informed consent given the retrospective nature of the study. A total of 161 patients with KOA with varus knee met the indication for TKA and underwent preoperative magnetic resonance imaging (MRI), and TKA from May 2018 to June 2021 were included. The presence of TKA was diagnosed based on clinical findings, such as a decreased range of motion, decline in activity of daily living, and radiological findings according to the Kellgren Lawrence classification.
9
The exclusion criteria were history of TKA, high tibial osteotomy, and previous collateral and posterior cruciate ligament injury because of the potential effects of these conditions on PA location, and unclear PA or ATA on MRI. Of 159 patients, 30 were excluded (20 patients without MRI data and ten patients due to unclear PA or ATA on MRI), and 129 patients with clear PA or ATA on MRI were finally included (Figure 1). Diagram of this study.
Radiological Evaluation of Branch Location
Classification of Popliteal Artery Branching
Classification of PA branching was first described by Lippert and Pabst in 1985 and modified by Kim et al in 1989, 10 consisting of three primary types. Type I, the most common, encompasses all PA divisions below the knee-joint level. Type II, the “high divisions,” includes all divisions of the PA at/or above the knee-joint level. Finally, type III consists of all cases of hypoplasia or aplasia in any of the branches. Type I was the most common branching pattern and had a total prevalence of 91.4%, and type II was the second most common, with a combined majority of 5.0%. 11 In most cases, PA branches into the ATA and PTA, usually distal to the height of tibial resection in TKA 12 (classified as group D). However, there are some cases in which the ATA branches from PA proximal to the height of the tibial cut line in TKA (classified as group P).
Radiological Evaluation of Popliteal Artery Branch Location Using Magnetic Resonance Imaging
The MR images were scanned on a 3T MRI System (Siemens, Echelon, Germany). MRIs were performed in patients who visited the outpatient clinic with knee problems before surgery. The sagittal and coronal plane along the tibial bone resection was evaluated using MRI of the knees in extension.
8
The full extension of the knee was maintained in the standard surface coil with a good pillow, to prevent flexion of the knee. According to a study, the sagittal and coronal plane images were obtained using the following protocol to investigate the location of the PA in the knee extension using MRI
13
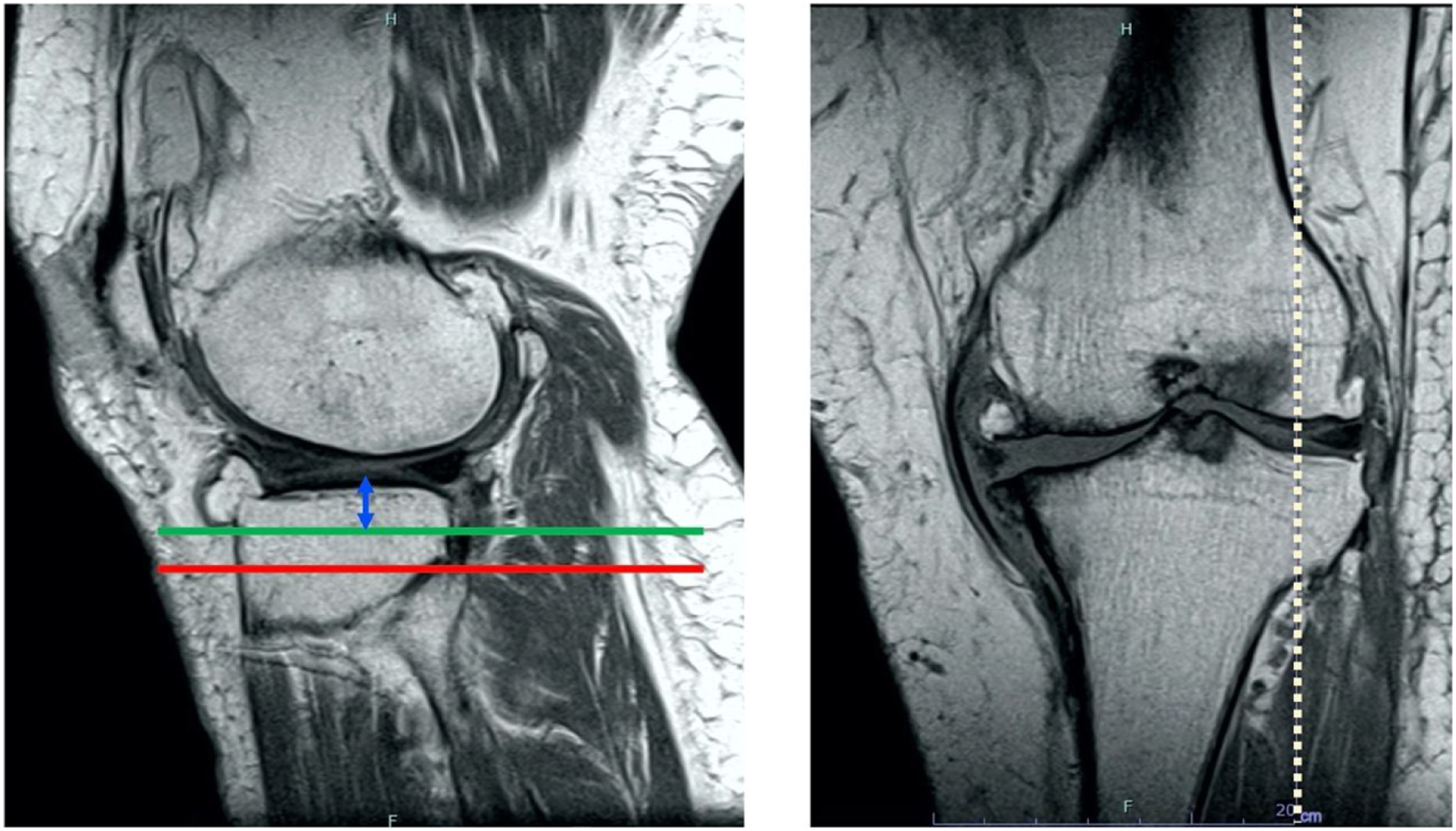
and proton density-weighted images with fat suppression. Each section was 5 mm thick with a .5 mm intervening spacing and had a 512 × 512 matrix. Two musculoskeletal radiologists, who were part of this study, read all MRIs. Cohen’s kappa coefficient was used to measure inter-rater reliability to determine if PA, ATA, and PTA were clearly shown as 1.0, thus indicating a perfect agreement. MRIs were performed not only for this study but also for routine preoperative evaluation before TKA. The tibial posterior tilt angle was measured from the postoperative radiograph (Figure 2). The rear tilt angle line was drawn in the MRI sagittal slice that matched the X-ray mediolateral view and left on the monitor (red line) (Figure 3). Then, we measured the amount of lateral tibial cut line from the tibial plateau (blue arrow) and drew a line parallel to the posterior tilt angle line (green line) (Figure 4). The lateral tibial cut line was referred from the surgical record, and the virtual tibial cut line was illustrated on the MRI sagittal plane on the lateral tibial joint. In the slice where the PA or ATA appears in the sagittal image while leaving that line, we measured the distance between the intersection of the tibial cut line and the surface of the posterior cortex of the proximal tibia and anterior wall of the PA or ATA (pink arrow)
14
(Figure 5). On postoperative radiographic ML) view, the tibial axis was drawn (yellow line), and the posterior tilt angle (red line) was measured. Abbreviation: ML, Mediolateral. On magnetic resonance imaging sagittal slice that matched the radiographic ML view, the posterior tilt angle line was drawn and left on the monitor. Abbreviation: ML, Mediolateral. On magnetic resonance imaging sagittal images of the lateral tibial plateau, the amount of lateral tibial cut line from the tibial plateau (blue arrow) was measured, and a line parallel to the posterior tilt angle line (green line) was drawn. On the sagittal slice where PA or ATA appears, the distance between the posterior cortex of the tibia and anterior wall of the PA or ATA, respectively, was measured (pink arrow). ATA, Anterior tibial artery; PA, Popliteal artery.


Statistical Analysis
The mean difference in distance between the posterior cortex of the tibia and PA or ATA was measured and compared. All data were presented as mean ± standard deviation. A P-value < .05 was considered statistically significant. A priori power analysis was performed using G*Power v.3.1 (Franz Faul, Kiel, Germany). 15 There were 6 cases in group P and 123 in group D, and the sample size was calculated to have an effect size of 1.2 with a power of .8. All statistical analyses were performed using the EZR software. 16
Results
Patient Characteristics.

Abbreviation: KL, Kellgren Lawrence.
Mean Age, Sexuality, Hip Knee Angle, Posterior Tilt Angle, Amout of Lateral Tibial Osteotomy, Distance Between Posterior Cortex of Proximal Tibia to Anterior Wall of Artery, and Groups P and D.
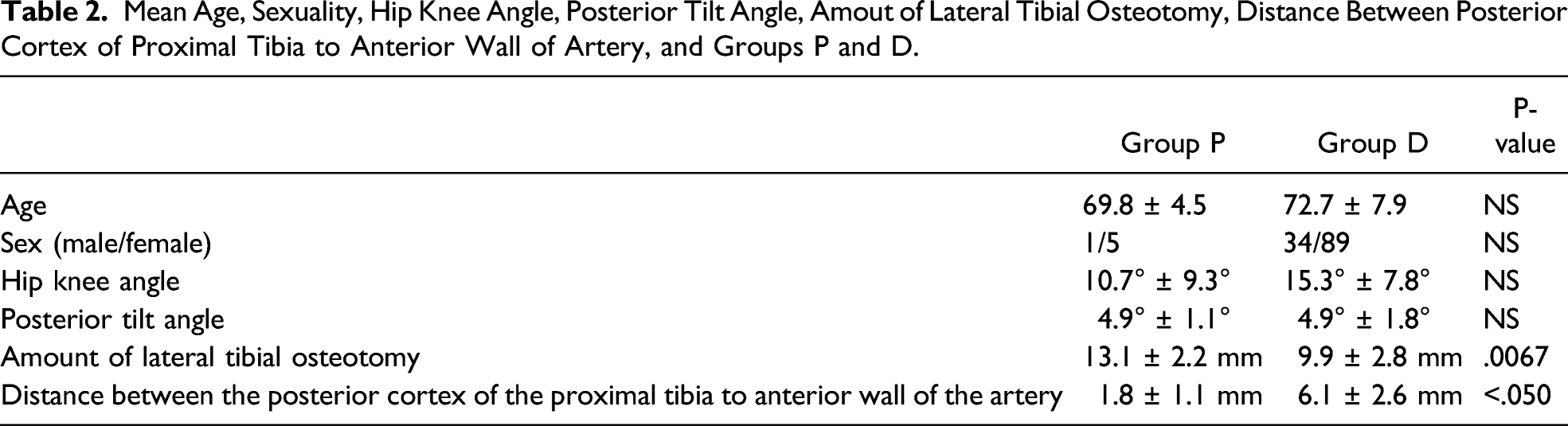
The distance between the posterior cortex of the proximal tibia to the anterior wall of the PA or ATA at the height of the tibial cut line was 1.8 ± 1.1 mm in group P, and 6.1 ± 2.6 mm in group D. The distance between the posterior cortex of the proximal tibia to the anterior wall of the ATA was significantly smaller in group P than that to the anterior wall of the PA in group D (P < .050) (Table 2).
Discussion
This study is the first English study to clarify how the proximal branching of ATA from the PA affected the distance between the posterior cortex of the proximal tibia to the anterior wall of the artery at the height of the tibial cut line TKA. Although MRIs are not routinely performed before TKA, this study alerted the surgeon to the artery being very close to the saw and encouraged appropriate retraction. In addition, it clarified that the proximal branching of the ATA from the PA is associated with the anterior wall of the ATA being near the posterior cortex of the proximal tibia at the site of the surgical cut during TKA.
The rate of proximal branching in our study was 4.7%, comparable with that of a previous study. 11 Calisir et al evaluated the anatomical variations in PA branching of 636 limbs that underwent peripheral computed tomography angiography using 64-slice multidetector computed tomography of the lower extremity. They reported that the rate of type II branching was 5.0%. 11 Day et al analyzed the PA’s branching patterns using angiography and described that 94.2% of limbs had an average level of PA branching, whereas the remaining had a high division of the PA at or above the status of the tibial plateau. 17 Adachi et al performed a cadaveric study of Japanese subjects in East Asia. The rate of proximal branching in their study was 2.7%. 18 By reviewing knee MRI data, Klecker et al. described that aberrant ATA might be at greater risk of injury in the orthopedic procedure. 8 They also found that proximal branching of the ATA is a potential risk factor for vascular damage in patients with KOA who underwent TKA. We evaluated the amount of lateral tibial cut line, tibial posterior tilt angle, and distance between the posterior cortex of proximal tibia to the anterior wall of PA or ATA for each case, using the operative record and preoperative MR images. This methodology was in line with similar studies.8,14,19 The novelty of this study is that we compared the distance between the proximal and distal branches in patients who underwent TKA.
Limitation
There were also several limitations in this study. First, the viewer who measured the distances was not blinded when the measurement was performed because the PACS system and surgery record, as available in the electronic patient medical record, were used in this study. Second, inter-rater reliability among musculoskeletal radiologists was not evaluated. Third, MRI was performed with only the knee extension position. Nevertheless, other studies have reported that flexion of the knee at 90° does not significantly increase the arterial–tibial distance than full extension, 20 and there is no reliable fall back of the popliteal artery in the knee flexion in a revision total knee situation. 21 Further studies in a primary complete knee situation will be performed. Fourth, the distance was measured using a copy and paste method of MRI acquisition. Fifth, all patients involved in this study were East Asian, and our results cannot be generalized to other ethnicities. Sixth, the mean lateral tibial cut line in the proximal branching group was more significant than the distal branching group. However, the lateral tibial cut line was determined not by branching location but by adequate extension bony gap. Also, most ATA branches from PA averaged 50.9 mm distal to the tibial plateau surface; therefore, the difference in the mean amount of the lateral tibial cut line between the two groups might not affect the distance between the posterior cortex of the tibia and anterior wall of the artery. 22
Conclusions
Proximal branching of the ATA from PA was a potential risk factor of arterial injury at TKA. However, surgeons need to perform a preoperative MRI of the knee to detect the branching pattern of the ATA from PA, and attention should be paid to the vessels for subsequent anomaly. Regardless, placing a retractor on the bone posteriorly is a prerequisite for safe surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.