
Abstract
Purpose
This study aimed to evaluate the effect of distal blocking screws on the stability and healing of ulnar diaphyseal fractures treated with intramedullary (IM) nails. The primary research question was whether the addition of distal blocking screws enhanced fracture stabilization and promoted faster healing than the standard IM nailing techniques.
Methods
This retrospective study reviewed medical records of 30 patients with ulnar diaphyseal fractures treated from February 2018 to September 2023. The patients were divided into two groups: those treated using IM nails alone (n = 17) and those treated with using IM nails with distal blocking screws (n = 13). The surgical time, medullary canal space, fracture healing time, and complications were assessed. Functional outcomes were evaluated using the Grace and Eversmann rating system, the DASH scores, and the VAS scores.
Results
The addition of distal blocking screws resulted in a slightly longer surgical time (56 min vs 47 min). However, the group with distal blocking screws had smaller medullary canal space and showed significantly faster fracture healing times (2.3 months vs 3.9 months; p = .036). There were no reported complications of nonunion, nerve injury, or infection in the distal blocking screw group, whereas the IM nail-only group had one case of nonunion (5.7%).
Conclusion
The use of distal blocking screws in conjunction with IM nails for ulnar diaphyseal fractures improves fracture stability and promotes faster healing.
Keywords
Introduction
Fractures of the radius and ulna are common upper extremity injuries in adults. The reported annual incidence of these fractures is approximately 10 cases per 10,000 individuals. Moreover, forearm fractures require robust anatomical internal fixation to maintain axial and rotational alignment.
Most surgeons opt for open reduction and internal fixation by using plates to treat forearm fractures. 1 However, even with the latest advancements, such as the limited contact dynamic compression plate, there are inherent disadvantages such as periosteal stripping and excessive cortical contact. These factors may impede blood the supply and elevate the risk of delayed union.2,3 Furthermore, there are inevitable disadvantages of open reduction such as long incisions and hardware irritation. To circumvent these challenges, intramedullary (IM) nailing has emerged as an alternative treatment for forearm fractures. 4
Initial attempts using Kirschner wires (K-wires), Steinmann pins, or Rush rods have resulted in unsatisfactory outcomes, including a high incidence of nonunion, mainly due to distraction at the fracture site and rotational instability. 5 Subsequent advancements in IM nail designs featuring pre-contoured shapes matching bone anatomy and fluting for enhanced rotational stability have sought to address these issues. 6 While pre-contoured IM nails remain a popular choice for ulnar diaphyseal fractures, concerns persist regarding nonunion due to instability at the distal end and malunion from torsional deformities. 7
Successful bone healing through relative stability requires controlled movement at the fracture site since too much motion could result in delayed healing or non-union. Most designs of ulnar IM nail do not incorporate distal interlocking screws. We expect that blocking screws could provide a third point of stabilization by reducing medullary space and restrict rotational and multidirectional movement at the nail tip.
The efficacy of blocking screws has been well-established as a mechanism for augmenting stability for femoral and tibial diaphyseal fractures. Moreover, blocking screws can be strategically placed before nailing to serve as guides, ensuring centralization of the nail upon insertion. 8 The effectiveness of blocking screws is not limited to the femur and tibia; encouraging outcomes have been reported for humeral IM nails augmented with blocking screws. 9 Therefore, this study aimed to investigate the potential enhancement in stability achieved by the addition of distal blocking screws in ulnar diaphyseal fractures treated with IM nails.
Materials and methods
Study population and design
This study was approved by our Institutional Review Board (2023-11-013) on November 16, 2023. Data from all the patients treated during the study period are available for review and analysis. All the participants provided informed consent before data collection. This study used a convenience sample of individuals attending clinics at our university hospital with patients who met the inclusion criteria being invited to participate in the study.
We retrospectively reviewed the radiographs and medical records of 30 patients with both forearm bone diaphyseal fractures. 17 patients admitted from March 2018 to February 2022 underwent closed reduction and internal fixation using IM nails and 13 Patients admitted after February 2022 until and September 2023 underwent IM nail fixation using blocking screws for ulnar fractures.
The inclusion criteria were as follows: (1) age >18 years; (2) both forearm bone and ulnar diaphyseal fractures, including open Gustilo and Anderson type I, II, IIIA, and closed fractures without neurovascular deficit; and (3) closed fractures with poor overlying skin, severe swelling, and extensive soft tissue damage. The exclusion criteria were as follows: (1) fractures involving injuries at elbow, such as Monteggia, and Galeazzi fractures; (2) osteoporotic bone and pathologic fractures; and (3) segmental comminuted fractures. All patients were followed up for a minimum of 12 months post operatively through questionnaire and radiological examination.
Surgical procedures
All surgical procedures were performed by the same surgeon one or 2 days after trauma. First-generation cephalosporins were administrated for prophylaxis. Under general anesthesia, the patients were positioned using a tourniquet in the supine position such that the injured forearm was in a neutral position and the elbow was at 90° flexion.
In patients with both forearm bone fractures (n = 21), the anterior approach was used to expose radius and midshaft volar radius plate (Acumed®, Hillsboro, Oregon, USA) was applied with at least three biocritical screws in each main fragment.
For all ulna fractures, IM nail fixation was performed using titanium-alloy ulna nail with 10° prebent and fluted design from Acumed. After making a 1 cm longitudinal incision at the tip of the olecranon, a reamer was inserted down the ulna and the nail length was measured directly from the reamer. Depending on the size of medullary canal at the isthmus, the diameter that will pass down the canal with minimal reaming was chosen as either 3.0 mm or 3.6 mm. Blocking screws were placed in the distal fragment prior to nail insertion to serve as a guide and facilitate smoother fracture reduction in challenging cases. Interlocking screws were inserted at the proximal end and for type C fractures, one or two extra blocking screws were placed to enhance overall stability. Well-molded long arm cast was applied, and 2 weeks after surgery, a hinged elbow brace was applied with the initiation of active range-of-motion exercise of the elbow.
Patient evaluation
All patients were followed up using forearm AP and lateral radiography 1, 3, 6 and 12 months postoperatively to evaluate bone healing. Radiological bone union was defined as periosteal callus formation and the absence of callus formation after 6 months was considered nonunion (Figure 1). X-ray images of a 45-year-old male patient admitted to emergency room with both forearm diaphyseal open fracture with distal radioulnar joint instability: (a) showing initial X-ray of both forearm bone fracture, (b) 1 month follow up X-ray showing callus formation at the fracture of both forearm bones, and (c) 1 year follow up X-ray showing complete bone union.
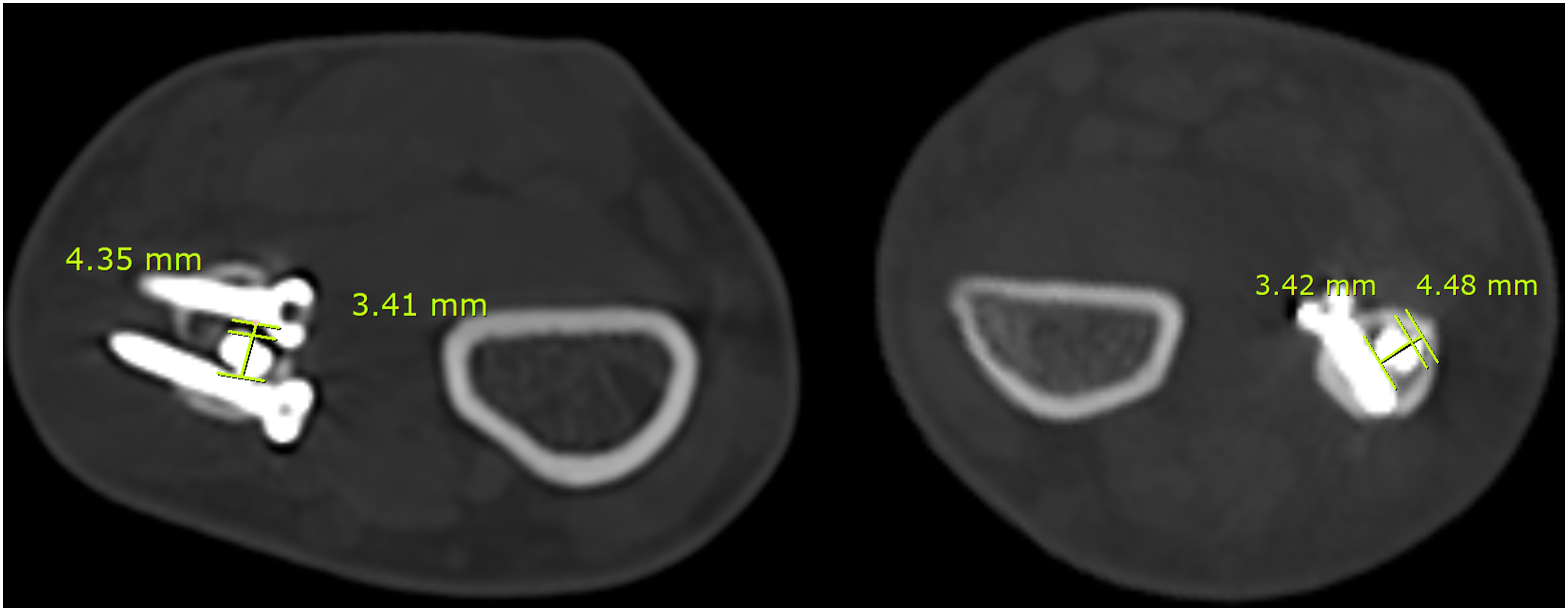
Two weeks postoperatively, stitch-out and subsequent CT imaging was performed. In the group without blocking screws, an axial cut was made 2 cm proximal to the IM nail tip to measure the shortest intramedullary canal space (Figure 2). In the group with blocking screws, measurements of the medullary space between the nails were recorded and the diameter of the IM nail was subtracted (Figure 3). Schematic diagram showing radiological evaluation procedure for medullary canal space. Using axial image of CT scan, total space of medullary canal (a) is subtracted by the diameter of IM nail (b). Example of CT scan images of two patients. Image on the left side is a case using two blocking screws medially and laterally and the second image is showing usage of blocking screws unilaterally.
Complications were recorded during postoperative hospitalization, such as wound site infection and nerve injury, and during outpatient ward visits for contractures and nonunion. Functional evaluation was done using Grace and Eversmann rating system, based on fracture union and forearm rotation measured using forearm goniometer. Additionally, the Disabilities of the Arm, Shoulder, and Hand (DASH) score was used with 0 points indicating perfectly functioning upper extremity and100 points indicating a complete impairment. The Visual Analogue Scale (VAS) score was also used to assess the pain level of patients, ranging from 0 indicating no pain to 10 indicating extreme pain.
Statistical analysis
The measurement data were presented as mean ± SD and analyzed using an independent sample t test. The chi-square test was used to analyze the enumeration data. Pearson’s correlation coefficient was used to examine the relationship between the callus formation period and medullary canal space. Descriptive statistical analyses were performed using SPSS (version 23.0; IBM Corporation, Armonk, NY, USA). Statistical significance was set at p < .05.
Results
The results demographic variables
Demographic and fracture related variables.

Results of intraoperative and postoperative variables and relationship between medullary canal space and fracture healing time
Intraoperative and post-operative variables with complication distribution.


Linear regression model graph showing relationship between fracture healing time (months) and medullary canal space (mm). Correlation coefficient of determination was 0.33 representing positive correlation between the two variables.
Complications of nonunion within the group using IM nail only
Complication rates were low across both groups, with no occurrences of nonunion, nerve injury/radioulnar synostosis, or infection reported in the blocking screw group and one case of nonunion reported in the IM nail-only group (5.9%).
Results showing functional scores
The Eversmann criteria scores for surgical outcomes were predominantly “excellent” across both groups with 69% in the blocking screw group and 85% in the IM nail-only group. The remainder were distributed between “good,” “acceptable,” and “poor” with no significant differences. DASH and VAS scores for pain showed no significant difference between the groups (DASH: 16.1 vs 14.6, p = .712; VAS: 3.5 vs 3.9, p = .421).
Discussion
This study aimed to evaluate the effects of distal blocking screws on ulnar diaphyseal fractures treated with IM nailing. Blocking screws, also known as poller screws, are used to provide additional mechanical stability to the medullary canal, particularly in complex or unstable fracture patterns. This technique, initially adopted for the treatment of long bones such as the femur and tibia, has shown promising results in enhancing stability and promoting healing. Our study extends this concept to the treatment of ulnar diaphyseal fractures.
Our results indicated a slightly longer surgery duration in the blocking screw group than in the IM nail-only group. This finding is consistent with the notion that blocking screws require additional procedural steps. However, the increase in the operative time was marginal and should be weighed against the potential benefits of blocking screws.
A significant finding of our study was the accelerated radiological fracture healing in the blocking screw group compared with that in the IM nail-only group. Our results for the IM nail-only group are consistent with those in the previous literature; the mean time for union was reported to be approximately 3 months in one study and slightly less 2.9 months in a recent study, with another suggesting a mean time of 3.3 months10–12 The blocking screw group had a mean healing time of 2.3 months which was shorter than the previously reported values. This finding is consistent with the theory that the incorporation of blocking screws contributes to increased stability at the fracture site, which is a key factor in expediting the bone healing process. The role of stability in fracture healing is supported by evidence suggesting that a well-fitted IM nail within the medullary canal can significantly enhance the primary stability and achieve better bone healing in lower limb IM nail fixation. 13
Furthermore, the positive correlation between medullary canal space and fracture healing time further supports the effectiveness of blocking screws in reducing the medullary canal space, which in turn enhances stability and potentially accelerates the healing process. The relationship between the medullary canal space and fracture healing time, particularly in the context of IM nailing, has been previously documented using biomechanical principles and clinical observations. A lower filling ratio of the nail to the medullary canal has been associated with excessive motion and loss of cortex-to-cortex apposition in trochanteric hip fractures. 14
Functional outcomes, as measured using the Grace and Eversmann criteria and the DASH and VAS scores, were similar between the groups. The functional outcomes, as indicated by the Grace and Eversmann criteria scores, were predominantly categorized as “excellent” for both treatment groups. This high rate of excellent outcomes in both the blocking screw group (69%) and the IM nail-only group (85%) suggests that both surgical methods are effective in restoring forearm functionality. This result suggests that the addition of blocking screws does not adversely affect the overall functional recovery.
Common complications of ulnar IM nailing include superficial infection, radioulnar synostosis, and nonunion. One study reported a nonunion rate of 7% in a cohort of 137 forearm fractures treated with a specific type of nail, whereas another study reported a 6.2% nonunion rate using a different nail design for firm fixation. 15 The results of our investigation represented a lower incidence of complications compared to those of previous studies. In particular, the cohort treated with blocking screws exhibited no nonunion, whereas the group treated with IM nails alone reported a single case (5.8%). This difference underscores the efficacy of blocking screws in mitigating the risk of nonunion by providing additional stability. While there was no peri-implant fracture from cortical screw insertion in our study, it is a common complication, especially in smaller bones such as the ulnar. Surgeons should be aware that larger thread sizes may increase the risk of peri-implant fractures and avoid blocking screws in osteoporotic patients. 16
In the case of nonunion, a patient who initially sustained both forearm bone fractures underwent surgical treatment with radial fixation using a plate and ulnar fixation using an IM nail. After a year of follow-up, hypertrophic nonunion was observed at the ulnar fracture site. Consequently, the patient underwent a second surgery in which minimal incisions were made near the fracture site and distal portion of the ulna, as shown in Figure 5. Then, a pair of blocking screws was applied proximally and distally to the fracture site and at the tip of the ulnar IM nail to limit the motion of the IM nail. No additional manipulations, such as fracture site curettage or bone grafting, were performed. This intervention proved to be effective as, after another year of follow-up, the fracture gap had reduced and there was evidence of callus formation. While distal insertion of blocking screws is recommended as a routine procedure, extra blocking screws can be placed in diaphysis near the fracture site in cases of nonunion. X-ray images of a 30-year-old male patient with nonunion complication: (a) postop X-ray after initial surgery, (b) X-ray after addition of distal blocking screws and blocking screws proximal and distal to the fracture site, and (c) evidence of bone union and callus formation 1 year after the second surgery.
Despite the promising results seen with IM nailing in the ulna, this technique is not adopted as the standard of care by many surgeons, who often prefer plate fixation due to its more established role in providing rigid stability. Plating allows for direct fracture visualization, better anatomical alignment, and consistent compression across the fracture site, which may lead to a higher level of confidence in achieving union. However, ulnar IM nails with the addition of blocking screws can provide more robust stability and further advancements in nail technology will result in widespread use of ulnar IM nails.
Recent designs of ulnar IM nails have incorporated distal locking screws. One study used an ulnar IM nail featuring transverse grooves at the distal end to facilitate distal locking, resulting in a delayed union rate of 2.3% (18). Another study explored the efficacy of distal interlocking screws complemented by a compression screw, yet the reported rate of nonunion was 4.8%. 17 While new ulnar IM nails have embraced the use of interlocking screws at the distal end, most of the designs are bulky. Our investigation reveals that blocking screws not only augment stability at the distal fracture site but also serve as a reduction tool, guiding nails for more accurate alignment. 18 Additionally, new nail designs such as Acumed’s Ulna Nail 2 System™, which offers an optional distal locking screw, has limited availability outside the United States and the higher cost associated with this new design is comparable to adding a few extra blocking screws.
Although this study provides valuable insights, it has some limitations. The retrospective design and relatively small sample size may limit the generalizability of the results. Future prospective studies with larger sample sizes are required to validate our findings. Additionally, long-term follow-up studies are needed to assess the durability of these outcomes and evaluate late-onset complications.
Conclusion
Our study suggests that the use of distal blocking screws in the treatment of ulnar diaphyseal fractures with IM nails can enhance fracture stability and promote faster healing with a low complication rate compared to using IM nails alone. While a compression plate remains a standard of care for ulnar fractures, IM nailing with blocking screws may serve as a valuable addition to the surgeon’s option for treating forearm fractures.
Footnotes
Author contributions
Conceptualization: Author 1,2. Data curation: Author1. Formal analysis: Author1, Author 1,2. Methodology: Author1,3. Writing - original draft: Author1. Writing - review & editing: Author1,2.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.