
Abstract
Objective
Periprosthetic fracture (PPF) is an uncommon but devastating complication after total knee arthroplasty (TKA). Anterior femoral notching (AFN) is one of a perioperative risk factor for PPF. The main purpose of this study was to compare between the rates of anterior femoral notching (AFN) and supracondylar periprosthetic femoral fracture (sPPF) of manual TKA and robotic arm-assisted TKA (RATKA). Meanwhile, blood loss, transfusion rates, inflammatory responses, complications, early clinical and radiological outcomes were also assessed.
Methods
This retrospective study included 330 patients (133 RATKA and 197 manual TKA). Differences in risks of inflammatory, blood loss, complications (periprosthetic fracture and periprosthetic joint infection), pre-operative and post-operative distal lateral femoral angle (LDFA), distal femoral width (DFW), prosthesis-distal femoral width (PDFW) ratio, AFN, femoral component flexion angle (FCFA), peri-operative and post-operative functional outcomes between the RATKA and manual TKA groups were compared.
Results
The operation time and postoperative CRP level in the RATKA group was significantly longer and higher than that in the manual TKA group (p < .001). However, there was no significant difference in postoperative WBC level (p = .217), hemoglobin loss (p = .362), postoperative drainage (p = .836), and periprosthetic fracture (p = 1.000). There was no significant difference in LDFA (p > .05), DFW(p = .834), PDFW ratio (p = .089) and FCFA (p = .315) between the two groups, but the rate of AFN in the RATKA group was significantly lower than that in the manual TKA group (p < .05). There was no significant difference in ROM between the two groups on POD3, POD 90 and 1 year (p < .05), but the FJS-12 score in the RATKA group was higher than that in the manual TKA group on 1 year (p = .001).
Conclusion
Robotic-assisted total knee arthroplasty can decrease the incidence of anterior femoral notching compared to posterior referenced instrumented total knee arthroplasty.
Introduction
Periprosthetic fracture (PPF) is an uncommon but devastating complication after total knee arthroplasty (TKA), with its incidence rates ranging from 0.3% to 2.5%. 1 Supracondylar periprosthetic femoral fracture (sPPF) is the most common type. 2 There is evidence which shows no increased incidence of periprosthetic fracture with anterior notching. 3 But, according to many studies, osteoporosis, advanced age, female gender, long-term use of steroid, neurological disorders, anterior femoral notching (AFN) and rheumatoid arthritis are perioperative risk factors for sPPF, among which AFN weakens the anterior surface of the femoral cortex and augment the local stress, and therefore it is considered as a predisposing factor for sPPF.4–9
In order to improve the accuracy of surgery, computer navigation and robotic arm assistive technology are widely used. Although it is still controversial whether it can bring better short-term outcomes to patients, a large number of studies have confirmed that computer navigation and robotic arm assistance can improve the accuracy of TKA in implant placement and mechanical alignment.10–13 However, there is no study comparing the rates of AFN and sPPF between manual TKA and robotic arm-assisted TKA. Therefore, the main purpose of this study was to compare the rates of AFN and sPPF between manual TKA and robotic arm-assisted TKA (RATKA). Meanwhile, blood loss, transfusion rates, inflammatory responses, early clinical and radiological outcomes were also assessed.
Methods
This study is a retrospective study including patients with osteoarthritis or rheumatoid arthritis who underwent manual or robotic arm-assisted primary TKA at our hospital from December 2020 to December 2021, with all procedures performed by a same experienced and trained surgeon, and patients with skin ulcers, malignancies, previous knee surgery, hip or ankle stiffness were excluded.
Preoperative planning and surgical technique
After admission, those patients decide to accept manual TKA or RATKA according to their own wishes. Then they were divided into manual TKA group and RATKA group according to whether they had accepted robotic arm assistance during the operation. All patients received general anesthesia and medial parapatellar approach. All patients in the RATKA group underwent TKA assisted by the MAKO robotic interactive orthopaedic arm system (Stryker Corp, Mako Surgical Corp, Ft. Lauderdale, FL). All patients took standard preoperative X-ray and CT scans. The CT scans were done with a slice space of 1 mm, and the CT data were transmitted to the MAKO planning module. Then, in use of the MAKO Robotic Knee System’s 3D template software, preoperative planning was performed for optimal bone resection, implantation and limb alignment.
In manual TKA, femoral resection was carried out using intramedullary reference at a 5° valgus angle and 3° external rotation for the distal femoral cutting. Posterior referencing system was used and various femoral component sizes being implanted with a system which has 2.5 mm antero-posterior increment between sizes. Extramedullary referencing was used to carry out the tibial bone resection. In the coronal plan, the cutting block had a 3° anteroposterior slope in the sagittal plane and was perpendicular to the mechanical axis of the tibia. All patients in manual TKA group used posterior stabilized (PS) implant (Stryker, Triathlon; Zimmer, NexGen or Wright, Advance).
In RATKA, the registration pins were inserted during the operation, and the probe was used to touch the corresponding points on the surface of the femoral condyle and tibial plateau in order to complete the registration. Dynamic tracking markers were used to assess the flexion and extension gaps, alignment, and range of motion. Tibial and femoral bone resection were performed perpendicular to the tibial and femoral mechanical axes, respectively. According to the evaluation of flexion space and range of motion, the femoral component flexion and tibial slope were then adjusted as required. All patients in RATKA group used posterior stabilized (PS) implant (Stryker, Triathlon).
All patients received intravenous infusion of 120 mg/kg epsilon aminocaproic acid (EACA) mixed with 100 mL of normal saline. After prosthesis placement, 2 g EACA was injected into the joint cavity. All patients were placed with drainage tubes, which were removed the next morning, and the drainage volume was measured. Tourniquet were used during the operation.
Post-operative inpatient care
All patients adopted the same rehabilitation plan and started active range of movement (ROM) and weight-bearing exercise on the first postoperative day (POD1). They were discharged from hospital on the POD4. All patients received self-controlled analgesia and 50 mg of intravenous Flurbiprofen axetil twice a day. Intravenous infusion of 1 g cefazolin sodium was done for prophylactic anti-infective treatment (1 time during operation, 3 times after operation). For thrombosis prevention, low molecular weight heparin was used after operation and oral apixaban for 2 weeks after discharge.
Clinical assessment
Each patient should be followed up for at least 1 year. Data were collected by a specially trained surgeon and patient demographics included: age at surgery (years); sex (male/female); BMI (kg/m2); ASA grade; surgical site (right/left); comorbidities (rheumatoid arthritis, neurological abnormalities, chronic steroid use); complications (periprosthetic fracture and periprosthetic joint infection); operation time (min); preoperative ROM; preoperative WBC count (109), preoperative C-reactive protein (CRP) concentration (mg/L) and preoperative hemoglobin concentration (g/l); postoperative drainage volume; Postoperative WBC count (109), postoperative CRP concentration (mg/L) and postoperative hemoglobin concentration (g/l); ROM on POD3, POD 90 and 1 year; FJS-12 score on 1 year. Differences between the two groups are compared.
Radiological assessment
The collected radiological data included: preoperative distal lateral femoral angle (LDFA); postoperative LDFA, distal femoral width (DFW); prosthesis-distal femoral width (PDFW) ratio; AFN; femoral component flexion angle (FCFA); measured by referring to the method used by Pornrattanamaneewong et al. in a retrospective study.
14
The distal femoral joint line (DJL) is drawn by the line connecting the distal-most aspects of medial and lateral condyles of the distal femur or femoral component. The line connecting the two midpoints of the femoral shaft at 5 and 10 cm above the DJL was defined as the (anatomical femoral axis) AFA, and LDFA was the lateral angle between AFA and DJL. The DFW was considered the longest distance of the distal femur that parallel to the DJL. In addition, the PDFW ratio was the ratio of the medial-lateral width of the femoral component to the DFW. The line connecting the two midpoints of the femoral shaft 5 and 10 cm above the most distal part of the femoral component was defined as sagittal femoral axis (SFA). The FCFA was the posterior angle between SFA and the sagittal plane of the femoral component. The AFN was measured as the depth between anterior femoral cortex and the anterior cut line of the distal femur (Figure 1). Differences between the two groups are compared. The measurements of knee radiographic outcomes from (A) anteroposterior view (anatomical lateral distal femoral angle, LDFA; distal femoral width, DFW; and prosthesis-distal femoral width ratio, PDFW) and (B) lateral view (femoral component flexion angle, FCFA; and anterior femoral notching, AFN).
Radiological outcomes were measured twice, once by the specially trained surgeon and once by a blinded surgeon. The intraclass correlation coefficient (ICC) was measured to be > 0.8, indicating good reproducibility.
Statistical analysis
Mean and range represents the continuous variables while categorical variables are represented by frequency and constituent ratio. The homogeneity of variances and data’s normality was examined and evaluated. When the parametric test assumptions were met after the examination of distributions of all variables, the Student t-test was used in independent groups and Mann–Whitney U-test was used if the data are not ordinarily distributed. Chi-square test and Fisher’s exact test was used for categorical variables. p < .05 means the difference is statistically significant. Statistical analysis and graphing were performed using SPSS version 25 (IBM Corporation, Armonk, New York, USA).
Results
Demographics
Demographic characteristics of the study groups.

ASA: American Society of Anesthesiologists RA:rheumatoid arthritis.
aFisher’s exact test.
Surgery and blood testing
Pre-operative and post-operative blood test.
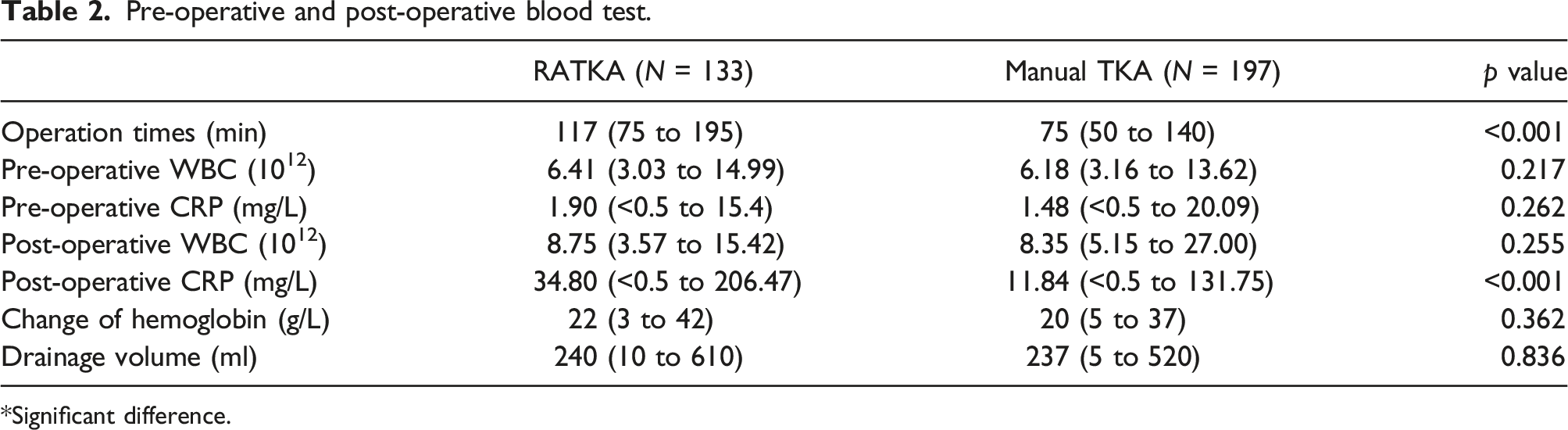
*Significant difference.
Radiological results
There was no significant difference in LDFA (90.56 vs 89.56, p > .05), DFW (83.01 vs 83.16, p = .834), PDFW ratio (0.90 vs 0.88, p = .089) and FCFA (89.75 vs 90.80, p = .315) between the two groups, but the rate of AFN in the RATKA group was significantly lower than that in the manual TKA group (2.26% vs 7.61%, p = .036), and the AFN depths in the RATKA group were all < 3 mm (Figure 2), while 4 cases (20%) in the manual TKA group had AFN depths≥3 mm (Figure 3). Table 3 covers these radiological findings. Case of notching in RATKA group. Case of notching depths≥3 mm in manual group. Radiographic outcomes. NA: not applicable. *Significant difference.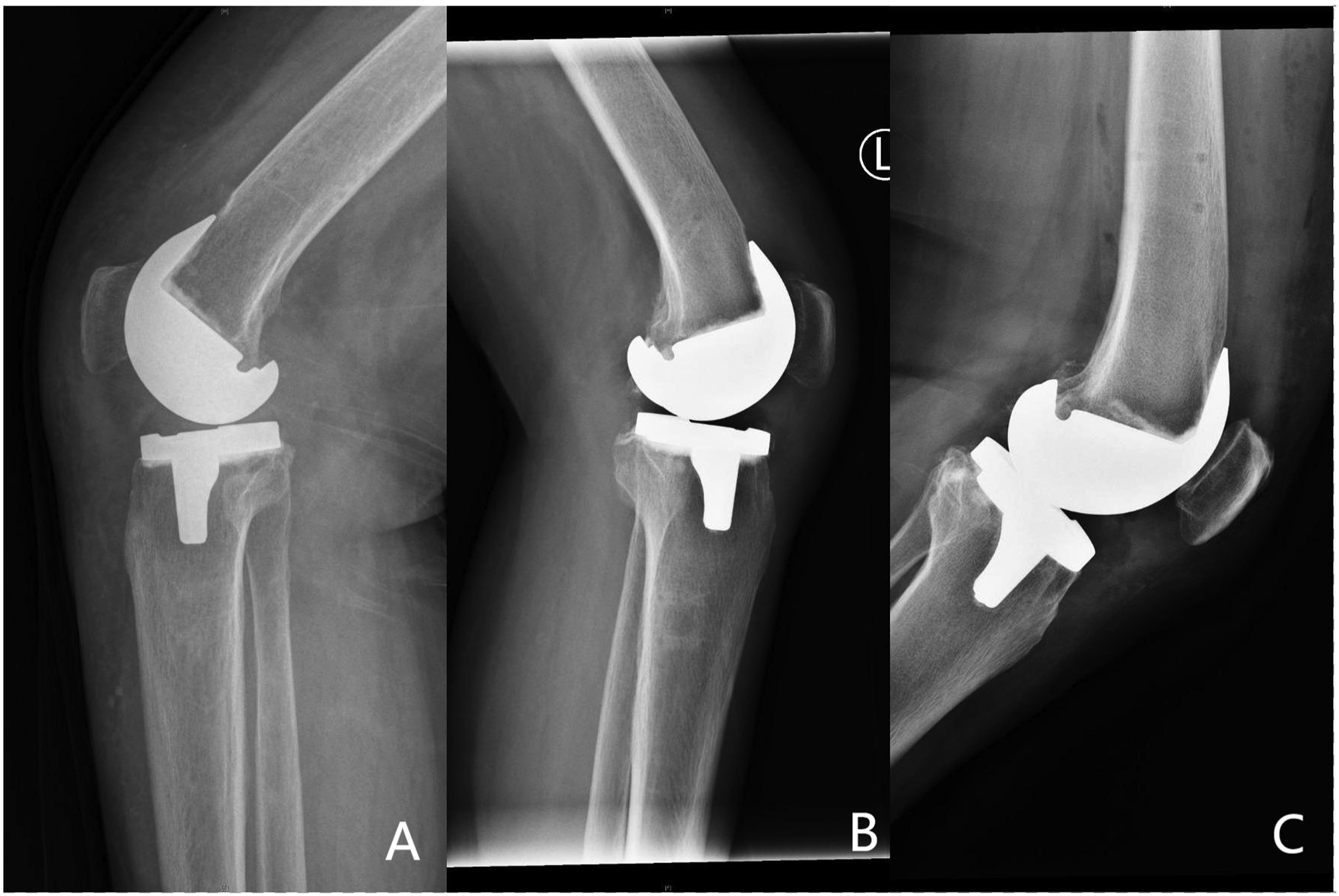


Clinical outcome
There was no significant difference in ROM between the two groups on POD3, POD 90 and 1 year (p > .05), but the FJS-12 score in the RATKA group was higher than that in the manual TKA group on 1 year (p = .001). During the follow-up period, there was one patient developed sPPF in the manual TKA group and then treated with locking plates (Figure 4). No patient developed PJI in both two groups. There was no significant difference in the rate of sPPF between the two groups. Table 4 generalizes the comparison of these clinical outcome. Case of supracondylar periprosthetic femoral fracture in manual group. Clinical outcomes. aFisher’s exact test. *Significant difference.

Discussion
To our knowledge, this study is the first to compare the rates of AFN and PPF in robotic-arm-assisted and conventional total knee arthroplasty. Although previous research has acknowledged robot-assisted surgery improves precision in bone-cutting, our research demonstrates the advantages of robot-assisted TKA from a new aspect.10,15–17 In this retrospective study, baseline characteristics were not significantly different, and we have several other important findings. First, RATKA can significantly reduce the rate of AFN. Second, compared with manual TKA, although RATKA increased the operation time and postoperative CRP level, there was no significant difference in the rate of sPPF and PJI between the two groups. Finally, compared with manual TKA, we found that patients undergoing RATKA had no statistically significant difference in ROM on POD3, POD 90 and 1 year. Although the FJS-12 score in the RATKA group was higher than that in the manual TKA group on 1 year, it may not be clinically significant.
sPPF after TKA are relatively rare but have devastating consequences. Even after treatment, related complications will also increase and the patient’s functional activity will decrease.18,19 Although there is evidence which shows no increased incidence of periprosthetic fracture with anterior notching, multiple studies have concluded that AFN is closely related to sPPF.3,20–23 Stamiris et al. 20 concluded that the risk of sPPF significantly increased in patients with AFN depth ≥3 mm compared with AFN depth <3 mm or no AFN. When AFN depth ≥5 mm was found intraoperatively, the surgeon should consider using a stemmed femoral component to stabilize the damaged distal part of the femur. In a study on 42 patients with PPF after primary TKA, Zainul-Abidin et al. 2 found that AFN was closely related to the occurrence of PPF after primary TKA. In a multicenter study, Hoffmann et al. 9 analyzed 36 patients with periprosthetic supracondylar femoral fractures treated with locked periarticular plate fixation. They found that nine of the 36 patients (25%) were radiographically diagnosed with notching of the anterior femoral cortex. Therefore, they suggested notching of the anterior femoral cortex should be avoided. In addition, multiple biomechanical studies have also found that AFN can lead to a significant reduction in the torsional strength of the femur, which may lead to the occurrence of sPPF.8,22,23 If the occurrence of AFN can be avoided, the devastating complication will be reduced. Lee et al. 24 concluded that the prevalence of anterior femoral notching by conventional TKA was 5.7%, and that for navigated TKA was 16.7%. In our study, the rate of AFN was lower in the RATKA group (2.26%) than in the manual TKA group (7.61%). Our study clearly demonstrates that the use of robotic arm assistance can significantly reduce the rate of AFN, thus reducing the devastating consequence of sPPF.
This study found that the operation time and postoperative CRP level in the RATKA group were significantly higher than those in the manual TKA group, but there was no significant difference in hemoglobin loss and the rate of PJI between the two groups, and there was no blood transfusion in the two groups after surgery. However, large registries, such as Australian, showed an increased incidence of infection in robotic arm-assisted TKA. Kayani et al. 25 found that robotic TKA was associated with a transient reduction in the early postoperative inflammatory response, decreased iatrogenic periarticular soft tissue injury, reduced femoral and tibial bone trauma compared with conventional TKA. In a prospective study, Li et al. 26 found that the operation time in the RATKA group was significantly longer than that in the manual TKA group, but there was no significant difference in postoperative CRP levels between the two groups. Kayani et al. 27 reported in a prospective study that although the operative time in the RATKA group was longer than that in the manual TKA group, the difference was not statistically significant, and they also found that the RATKA group lost significantly less hemoglobin than the manual TKA group. At present, there are differences between relevant conclusions. Operation time is affected by many aspects.28,29 It may not be appropriate to simply compare the operation time. The sample size of this study is larger than that of the other two studies, but we consider that the sample size is still relatively small.
Distal femoral preparation and sizing are important for overall balancing and function. Femoral sizing and subsequent osseous resections can be performed with use of either an anterior or a posterior referencing technique. With the anterior referencing technique, notching of the anterior femoral cortex can be avoided, but it is more difficult to control posterior condylar offset and the size of the flexion gap. 30 With the posterior referencing technique, the size of the flexion gap and posterior condylar offset usually can be controlled, but the risk of anterior notching or overstuffing is increased. 31 The rate of anterior notching when posterior referencing is used has been reported as high as 30% to 40%.21,32 But, in this study, the rate of anterior notching is less than 10%. It may be affected by the skills and experiences of surgeons.
The MAKO Total Knee Robotic Interactive Orthopedic Arm System utilizes the patient’s preoperative knee computed tomography and 3D modeling to determine the size and orientation of the implant prior to bone resection. However, in this study we found no significant difference in postoperative radiological assessment between the RATKA group and manual TKA group. Our conclusion is also supported by other studies, Li et al. 26 reported no significant differences in radiological or functional outcomes between RATKA and conventional manual TKA. In a prospective random study with a follow-up lasting more than 12 years, Cip et al. 33 reported that no significant difference in all X-ray assessments between RATKA and manual TKA. But there are also many studies reporting that RATKA has higher accuracy of bone cuts and implant alignment.11,12 Ruangsomboon et al. 34 reported that although RATKA likely results in higher radiologic accuracy than manual TKA, there is probably no clinically important difference in clinical outcomes between RATKA and manual TKA. One of the reasons for the different conclusions is that the occurrence of surgical errors is becoming lower and low as the experience of the surgeon accumulates, and a relatively small sample size might affect the results, as a result, a larger sample study is needed.
In addition, we also found that the FJS-12 score in the RATKA group was higher than that in the manual TKA group on 1 year. Although there is a numerical difference, the difference from 36.5 to 38 may not be clinically significant. In a multicenter study using Mako surgical system, Joo et al. reported that there were significant gradual improvements in FJS-12 scores from baseline preoperatively to 1–2 years and then to>2 years of follow-up. 35 In a study on 73 patients undergoing RATKA with a short-term 2-years follow-up during which FJS-12 assessment was conducted, Ward et al. 36 found that patients using RATKA were more likely to forget their artificial joint. However, other studies have come to different conclusions. Yamamoto et al. revealed that RATKA did not show any improvement in FJS-12 scores at 1 to 2 years postoperatively compared to the manual TKA. 37 In a randomized controlled trial with at least 10 years of follow-up, Kim et al. 38 found no difference in functional outcome scores, prosthetic survival rate, and complications between RATKA and conventional TKA. Our study demonstrates that in the short term, compared with manual TKA, RATKA cannot make it easier for patients to forget their artificial joints, but the difference in the medium and long term after surgery is not clear and needs to be supplemented by long-term follow-up studies.
There are still some limitations in this study. First, this is a retrospective review and not a prospective randomized study. This study design may allow for the inadvertent introduction of selection bias but there were no differences between the two groups with respect to age, sex, BMI, comorbidity and ASA scores. Second, due to the low rate of sPPF and PJI, small sample size and short follow-up time in this study, only one patient developed sPPF and no patient developed PJI in both two groups. We cannot prove that RATKA can reduce the rate of sPPF. A small sample size also leads to a decrease in the credibility of the conclusion. In the future, medium and long-term follow-up studies with larger samples will be needed. Third, we did not compare postoperative pain levels, knee function scores, and patient satisfaction between the two groups, which may lead to the masking of the advantages of robotic surgery. Finally, there were fewer obese patients in this study. 15% and 13% of the patients in the RATKA and manual TKA groups had a BMI >30 kg/m2 respectively. No patients had a BMI >40 kg/m2. Obese patients may have difficulty determining the exact location of the prosthesis. Such patients tend to be better candidates for RATKA, so this study cannot show the advantages of robotic surgery in this regard.
Footnotes
Author contributions
All authors contributed to conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing, review and editing, and visualization.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grants from the Shandong Provincial Natural Science Foundation, China [Grant No. ZR2021MH090] and supported by Young Elite Sponsorship Program of Shandong Provincial Medical Association [Grant No. 2023_LC_0267].
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.