
Abstract
Objective:
To evaluate the medium-term outcomes of a posterior-stabilized mobile-bearing total knee arthroplasty (PS-MB-TKA) and the role of different prognostic factors.
Methods:
Patients indicated for a primary cemented PS-MB-TKA between 2002 and 2010 were included and prospectively evaluated using the Knee Society Scoring System (KSS) and the Hospital for Special Surgery (HSS) knee scores. The Knee Society Roentgenographic Evaluation form was used for the radiological evaluation. Different variables were collected and divided into patient- and surgery-related. Logistic regression was used to analyze the correlation between these variables and implants outcomes and survivorship.
Results:
In total, 149 cases were included (67.8% female, average age 70.4 years, SD ±9.4). The patella was resurfaced in 12.1% of the cases. All the implants were cemented. The average follow-up was 87.3 months (SD ±21.2). Postoperatively, there was a statistically significant improvement in all the scores. The cumulative survival was 96.2% (SD ±0.02%). At the regression analysis, female gender was associated to worse satisfaction KSS (OR = 0.26), functional KSS (OR = 0.22), and HSS (OR = 0.37) scores. Patellar resurfacing and subsequent contralateral procedures were associated to better functional KSS score (OR = 4.13, OR = 2.21), as well as varus preoperative alignment (OR = 2.12). On contrary, valgus preoperative alignment was associated to worse objective KSS score (OR = 0.23). No variables were correlated to failure or presence of radiolucent lines.
Conclusion:
Good medium-term outcomes were obtained using PS-MB-TKA, with a cumulative survivorship of 96.5%. Female gender and valgus preoperative alignment were associated to worse objective and subjective outcomes. Conversely, patellar replacement, subsequent contralateral TKA, and varus preoperative alignment were associated to better functional outcomes.
Introduction
The number of total knee arthroplasties (TKAs) will grow by 673% between 2005 and 2030. 1 Mobile-bearing TKA (MB-TKA) was designed with the aim to provide a more physiological range of movement, to reduce the bone-implant interface stresses and to minimize polyethylene wear. 2,3 Different theoretical advantages of MB-TKA have been described. MB interface should increase implant conformity and contact area without increasing stresses on fixation interface. Furthermore, a mobile surface should reduce the torsional stresses to the fixation interface. 4 MB-TKA also allows for increased sagittal plane conformity, improving anteroposterior (AP) translation control and reducing the paradoxical anterior femoral translation. 5 Because of these characteristics, some authors described a reduction in poly wear in knee simulator testing of a MB-TKA versus a fixed-bearing design. 6 Furthermore, MB-TKA allows for a “self-alignment” of the poly insert on the tibial tray, with the maintenance of a large, centrally located contact area during flexion, extension, and axial rotation of the knee, allowing for small correction of rotational malalignment. 7
Good outcomes are reported for MB-TKA, with a cumulative survivorship close to 98% at 10 years of follow-up. 8,9 However no better outcomes were demonstrated for MB compared to fixed-bearing TKA, despite the theoretical advantages of MB-TKA. 10,11
Despite the good results described in the literature, different authors reported a considerable amount of unsatisfied patients after a TKA. Baker et al. concluded that only 4959 (22%) out of 22,278 patients were completely satisfied with the procedure. Furthermore, the authors found the perception of symptoms improvement being the strongest predictors for patient’s satisfaction. 12 Similarly, different authors tried to identify the prognostic factors correlated to better TKA outcomes. Gandhi et al. evaluated 551 patients with an average follow-up of 3 years, concluding that old age, long follow-up, major co-morbidity, and a poor mental health state at time of surgery were correlated to low results. 13 Nuñez et al. in 2010 evaluated 60 patients at 12 months of follow-up, concluding that obese patients and number of complications after discharge, as well as number of co-morbidities and intraoperative difficulties were associated to a worse The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score. 14 Furthermore, Santaguida et al. in their systematic review on 64 studies on total hip and knee replacement concluded that there was three- to fivefold increased risk for revision in young or male patients. 15
However, most of the studies focusing on prognostic factors influencing TKA outcomes have a short-term follow-up (12 months to 3 years), and evaluated separately preoperative, intraoperative, and postoperative variables.
The aim of this study was to evaluate clinical and radiological medium-term outcomes of a posterior-stabilized (PS)-MB-TKA. Furthermore, different prognostic factors potentially associated to patient’s satisfaction, outcomes, and implant’s survivorship were evaluated.
Materials and methods
Research design
The Institutional Review Board (IRB) of the author’s institution defined this study as exempt from IRB approval (prospective study on a well-established surgical procedure).
Inclusion criteria and data collection
All the patients who underwent primary TKA between January 1, 2002, and December 31, 2010, using the NexGen LPS-Mobile Bearing Knee ® (Zimmer, Warsaw) at our institution were enrolled in the study. All the available patients were clinically evaluated in December of 2015 and demographic, preoperative, and surgery data were collected. Demographic data included gender, age, and body mass index (BMI). Preoperative data included the objective evaluation (range of motion, alignment, and instability) and previous surgery on the operated knee. Surgery-related variables included subsequent contralateral TKA, patellar replacement, and time of surgery (Table 1). All the postoperative complications and/or failures (intended as revision surgeries) were also recorded.
Summary of outcomes and variables.

KSS: Knee Society Score; HSS: Hospital for Special Surgery knee score; BMI: body mass index.
Surgical technique
All surgical procedures were performed by the same surgeon (RR) using a PS-MB-TKA. A standard anteromedial approach with a medial parapatellar capsulotomy was performed in all the cases. The tourniquet was positioned but inflated only during the implant cementation. The tibial cut was performed perpendicularly to the tibial shaft in the coronal plane; the tibial slope followed the surgical technique of this implant. The distal part of the femur was resected with an attempt to achieve femoral–tibial alignment of 3–7° of valgus on the coronal plane. The flexion and extension gaps were carefully evaluated using both measured resection and gap balancing techniques in order to obtain symmetrical and equal spaces. If necessary, medial or lateral soft tissue releases were performed, according to the pie-crusting technique. 16 –18 All the components were cemented. The patella was selectively replaced in cases of maltracking and severe symptomatic osteoarthritis (grade 3 or 4). Postoperatively all patients were allowed for immediate full weight-bearing, and they began rehabilitation (including continuous passive motion machines) the day after the operation. Postoperative controls were planned at 3 months, 6 months, 1 year, and annually thereafter.
Outcome measures
Clinical evaluation
The Knee Society Scoring System (KSS) 19 and the Hospital for Special Surgery (HSS) knee scores 20 were used for the subjective and objective evaluation. Furthermore, a Visual analogue Scale (VAS) scale (0 to 100) was used to assess both the satisfaction from the surgery and the degree of function of the operated knee compared to the contralateral one.
Radiological evaluation
All the patients underwent pre- and postoperative weight-bearing X-rays including AP, lateral, long-leg view, and a merchant view for the patellofemoral joint. Limb alignment, component positioning, and presence of radiolucent lines were evaluated using the Knee Society Roentgenographic Evaluation System. 21 All the angles were measured by the same surgeon using a goniometer for printed X-ray, or dedicated instrumentation for digital images. The presence of radiolucent lines was evaluated by the same surgeon both on the AP and lateral views.
Data analysis
Descriptive statistic was used for all demographic, subjective, and objective outcomes. Data were collected with Excel® Microsoft, and presented with average and standard deviation (SD) and t test and χ 2 test were used to analyze differences in continuous and categorical variables, respectively.
Four main outcomes were identified: KSS score (divided in the single items), total HSS score, implant failure, and presence of both progressive and nonprogressive radiolucent lines. A satisfying KSS score was defined as greater than 70 points for the objective and functional sections, greater than 30 points for the satisfaction, and greater than 10 points for the expectations section. The total HSS score was considered good if greater than 80 points. These cutoff values were chosen based on literature data 19,20 or on the average scores obtained in this case series.
Different variables were identified and they were grouped into patient- and surgery-related (Table 1). Each variable was tested using simple logistic regression to evaluate any association to each single outcome. To reduce the overfitting phenomenon, all the correlations with p value greater than 0.1 were removed from further statistical analysis. All the remaining variables were tested for each single outcome using a multiple logistic regression to evaluate any significant correlation (p < 0.05). The statistical software Medcalc® (Ostend, Belgium) was used to perform the regression analysis.
Results
Demographic
Between January 1, 2002, and December 31, 2010, 179 patients underwent a total of 189 TKA (10 bilateral) using the NexGen LPS-Mobile Bearing Knee® (Zimmer, Warsaw) at our institution. Of these patients, 30 patients were dead (8 bilateral implants) and 10 patients were not available for the evaluation (2 bilateral implants) at the time of follow-up. Excluding these patients, 149 cases (129 patients, 20 bilateral) were enrolled in the study. There were 87 female patients (67.4%). The average age was 70.4 years (SD ±9.4), with 35.6% of patients more than 75 years old. The average BMI was 27.4 kg/m2 (SD ±3.8). Considering the World Health Organization (WHO) cutoff for BMI, 22.1% were considered obese (BMI greater than 30 kg/m2).
The average follow-up was 87.3 months (SD ±21.2 months). 118 cases (79.2%) were clinically evaluated while the remaining 31 cases were not available to come to the hospital for the visits. These patients underwent a telephonic subjective evaluation, and they were excluded from the objective analysis.
Clinical preoperative evaluation and surgery related data
In 75.8% of cases, the diagnosis was primary idiopathic knee arthritis, and in 12.1%, it was rheumatoid arthritis. The remaining cases were distributed into hemophilic patients, osteonecrosis or post-traumatic arthritis. Thirty-five patients (27.1%) underwent a previous surgery on the operated knee. Only 27 cases (18.1%) had a physiological lower limb alignment; 55.7% and 26.9% of the cases had a varus or valgus alignment, respectively. The average preoperative knee flexion was 108° (SD ±18.9°), with 45 patients (34.8%) having a flexion contracture with an average of 10.7° (SD ±7.3); 64.4% of patients preoperatively had a moderate mediolateral instability.
The mean length of surgery was 95 min (SD ±22.9), and in 65.1% of the cases, it was longer than 90 min. The tourniquet was inflated only during the cementation, with an average time of 22 h and 43 min (SD ±9.3). In 18 cases (12.1%), the patellar replacement was performed. All the components were cemented. In 46.3% of the cases, a subsequent contralateral knee replacement was required.
Clinical postoperative results
The average objective KSS score increased from 45.3 points (SD ±17.8) to 80 points (SD ±15.1) at the last follow-up, with a statistically significant improvement and 76.5% of patients obtained a score greater than 70 points. The average postoperative flexion was 111.4° (SD ±14.5°). Only 6 patients had postoperative moderate medial–lateral instability. At the logistic regression, the only variable correlated to the KSS objective score was the presence of a preoperative valgus alignment. Patients with a valgus alignment had a lower probability to obtain a better objective KSS (OR = 0.23, p = 0.022). The results of the regression analysis are summarized in Table 2.
Summary of prognostic factors related to subjective–objective outcomes.

BMI: body mass index; KSS: Knee Society Score; HSS: Hip Society Score; AP: anteroposterior; ML: mediolateral; N/A: not applicable.
Italic values represent statistical significant result (p < 0.05).
The average satisfaction KSS significantly improved from 10.7 points (SD ±3.7) to 30.2 points (SD±10.2) (p < 0.0001). Furthermore, 87.9% of patients were satisfied or very satisfied with the procedure. At the regression analysis, female patients resulted having a lower probability to obtain a high KSS satisfaction score (OR = 0.26, p = 0.003, Table 2).
The average postoperative expectation KSS score was 9.75 points (SD ±2.9). In the multiple regression analysis no variables showed a significant correlation to higher expectation score (Table 2).
The average functional KSS score increased from 45.4 (SD ±18.6) to 64.9 points (SD ±25.4) (p < 0.0001). The regression analysis revealed that female patients had a lower probability to obtain a high functional score (OR = 0.22, p = 0.0003). Conversely, different prognostic factors resulted associated to high functional outcomes: preoperative varus alignment (OR = 2.12, p = 0.046), patellar replacement (OR = 4.1, p = 0.021), and subsequent bilateral TKA (OR = 2.21, p = 0.034).
The average total HSS score significantly increased from 41.3 (SD ±10.1) to 81.1 points (SD ±15.5, p < 0.001). At the regression analysis, female gender resulted associated to a worse HSS total score (OR = 0.37, p = 0.01).
Radiological postoperative evaluation
The postoperative radiological evaluation was available for 110 cases; 8 patients were excluded from the radiological analysis because of inadequate X-rays. In 73 cases (66.4%), at least one nonprogressive radiolucent line could be detected. The percentage decreased to 20.9% considering only the lines greater than 2 mm. In five patients at least one progressive and significant radiolucent line could be detected; all these cases underwent a TKA revision. As shown in Table 3, no variables were correlated to the presence of both nonprogressive or progressive radiolucent lines.
Summary of prognostic factors related to radiolucent lines and failure.

BMI: body mass index; AP: anteroposterior; ML: mediolateral; N/A: not applicable; OR: odds ratio; CI: confidential interval.
Using the Knee Society Roentgenographic Evaluation System, 21 all the implants were well positioned. The average α-angle was 95.1° (SD ±3.4°), the β-angle was 88° (SD ±3.4°), the γ-angle was 4.2° (SD ±2.5°), and the δ-angle was 84.9° (SD ±8.8°).
Complication and failures
In 29 cases, a complication was detected (19.5%). Postoperative fever spontaneously resolved was the most common complication (10 cases). In 5.4% of cases, there was a moderate postoperative stiffness, resolved with intensive rehabilitation, while in 1.3% of cases, there was a severe stiffness requiring arthroscopic adhesion removal. Furthermore, 2% of cases had a severe postoperative anemia, 2% had deep venous thrombosis, with one case of pulmonary embolism, one case of intraoperative patellar tendon rupture, and one case of acute infection treated with debridement, irrigation, and polyethylene substitution.
Five patients underwent TKA revision: in four cases, the diagnosis was aseptic failure while the last case was due to instability. The cumulative survivorship was calculated using the Kaplan–Meier method, and it was equal to 96.5% at 140 months (SD ± 0.02, Figure 1). In the logistic regression analysis, no variables were associated to the implant’s failure (Table 3).
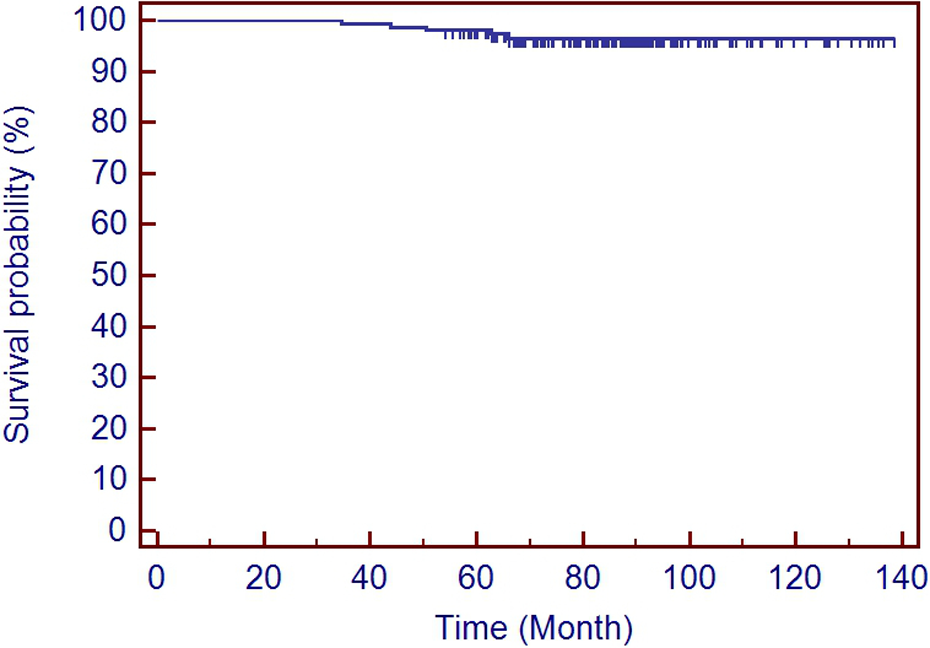
Cumulative survivorship calculated using the Kaplan–Meier method.
Discussion
This is a prospective study on 129 patients who underwent 149 TKAs using a MB-PS implant, with an average follow-up of 87.3 months (SD ±21.2). In 75.8% of cases, the diagnosis was primary idiopathic knee arthritis, and in 12.1%, it was rheumatoid arthritis.
The first finding of this study is that PS-MB-TKA provided good objective, subjective, and radiological outcomes at medium-term follow-up. The cumulative survivorship in this study, using revision surgery as definition for failure, was 96.5% at the final follow-up (SD ±0.02). These results are consistent with those previously reported on literature with this implant. 8,9,22 MB-TKA has different theoretical advantages over fixed-bearing surfaces. First of all, there is an increased implant conformity without increasing the interface stresses, resulting in aseptic loosening. 4 In the sagittal plane, the increased conformity may allow for a more predictable AP motion while, in the coronal plane, it may prevent polyethylene stresses in presence of a femoral condylar lift-off. 5,6 Furthermore, the “self-alignment” properties of the MB-TKA may allow for small correction of component malrotation, facilitating the patellar tracking. 23,24
The radiographic analysis revealed 20.9% of patients having a radiolucent line greater than 2 mm in at least one zone, as described by Ewald et al. 21 However, in only five cases there were progressive symptomatic radiolucent lines, suggestive for failure. All these patients underwent TKA revision during the study. Nonprogressive radiolucent lines were more common revealed behind the proximal flange of the femoral component in the lateral projection and underneath the tibial plateau in the AP view. Similar results were reported by different authors using the same implant. 8,9
To our knowledge, this is the only study evaluating both demographics, surgical, and objective variables potentially associated to either subjective, objective, or radiological outcomes and failure.
Female gender was associated to worse satisfaction, functional KSS score, and total HSS score (OR = 0.26, 0.22, and 0.37, respectively). This result is consistent with other studies. 25 –27 However, Liebs et al, in a study on almost 1000 patients, concluded that female patients had greater improvement in WOMAC pain and function in the early period, but no differences can be detected after 12 months of follow-up. 28
There was no association between BMI (greater than 30 kg/m2) and all the outcomes evaluated. However, other studies reported an association between obesity and increased morbidity and mortality, as well as worse outcomes, after TKA. 29 Spicer et al. evaluated the outcomes of 285 obese patients in comparison with 371 nonobese patients. The authors concluded that patients with a BMI greater than 40 kg/m2 had a 5-fold increased rate of focal osteolysis. 30 Other authors demonstrated an increased rate of morbidity and mortality for obese patients. 31 Furthermore, Franklin et al. evaluated 8050 patients concluding that poor functional result was associated with old age, BMI over 40 kg/m2 and poor quadriceps strength. 32
The preoperative alignment may also affect the outcomes. In this study, having a preoperative valgus alignment was associated to low KSS objective score. This may be partially explained by the higher complexity of these cases compared to varus aligned knees. 18 Conversely, having a varus preoperative alignment was associated to high functional KSS score (OR = 2.12). This result may also be related to the postoperative tibial component alignment (β angle), which was equal to 88° (SD ±3.4°). The correlation between better outcomes and slight under-correction of preoperative varus deformity was previously demonstrated by Vanlommel et al. 33
The KSS functional score was also influenced by patellar replacement and bilateral subsequent TKA. Both these factors were associated to better functional score, with OR 4.13 and 2.21, respectively. Chen et al. published a meta-analysis of randomized controlled trial about outcomes after patellar resurfacing or not during primary TKA. Despite no definitive conclusion about the benefit of patellar resurfacing can be drawn by the existing literature, the authors observed that patellar resurfaced patients showed better KSS scores in long-term follow-up (5 or more than 5 years). 34
Few authors also evaluated the association between poor mental health state or depression and TKA outcomes. All of these studies concluded that depression is a major risk factor to obtain worse outcomes after primary TKA. 35–36 All the studies describing prognostic factors affecting TKA outcomes are reported in Table 4.
Summary of the literature on prognostic factors in TKA outcomes.

IOD: degree of intraoperative difficulty; TKA: total knee arthroplasty; BMI: body mass index; KSS: Knee Society Score; IOD: intraoperative difficulty; WOMAC: The Western Ontario and McMaster Universities Osteoarthritis Index.
This study has several limitations. First we have not a control group (i.e. fixed-bearing implants) to compare our outcomes with. Second, almost 20% of patients were not clinically evaluated, potentially creating a bias in the objective evaluation. However, these patients were excluded from both the objective outcomes and from the analysis of prognostic factors. Finally, this is a medium-term follow-up study (average follow-up, 81.7 months), so no definitive conclusion regarding outcomes and survivorship can be drawn.
Conclusion
Good objective and subjective outcomes can be achieved using MB-PS implant, with 96.5% of cumulative survivorship at medium-term follow-up. Preoperative alignment influenced the outcomes, with valgus alignment being associated to worse objective outcomes. Female gender was associated to both low postoperative satisfaction and functional outcomes. Furthermore, having a replaced patellar or bilateral TKA shown association with better functional outcomes. There was no association between all the tested variables and presence of radiolucent lines or failures.
Footnotes
Declaration of conflicting interests
Roberto Rossi is a teaching consultant for Zimmer Biomet ®. The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.