
Abstract
Objective
To assess the feasibility of the robot-assisted retractor. To compare the muscle injury of the two operation modes, intermittent retraction mode and continuous retraction mode in the robot-assisted retractor to find a better robot operation mode.
Methods
A new robot-assisted retractor experimental platform was developed. Three incisions were made on the backs of three beagles. The robot-assisted retractor was used to retract the muscle on both sides of the incisions in intermittent retraction mode and continuous retraction mode, and the operation of the robot system was observed. The muscle samples were stained with hematoxylin-eosin (HE) to observe the muscle injury. The difference between the muscle injuries of the two groups was statistically compared using paired t test.
Results
The robot-assisted retractor can precisely retract to the specified position without malfunction or dangerous actions. Histologic evaluation showed that fewer muscle injury was found in the intermittent retraction mode group of the robot-assisted retractor compared to the continuous retraction mode group.
Conclusion
The robot-assisted retractor offers a certain degree of feasibility and safety. The robot-assisted retractor is able to effectively reduce muscle injury with the intermittent retraction mode.
Introduction
In recent years, robotic technology has been introduced into various orthopedic subspecialties. Spine surgery has evolved considerably with the help of technological advances. 1 The robot has significant advantages in fine movements, in reducing operator fatigue or physiologic tremor, in reducing radiation exposure, in shortening the time for pedicle screw placement, and so on. 2
Posterior lumbar surgery is one of the most conventional methods for the treatment of lumbar diseases. Nevertheless, low back pain has been a persistent issue in postoperative patient. Studies have shown that postoperative low back pain and dysfunction may be related to paravertebral muscle injury and atrophy. 3 In addition, previous studies have shown that paravertebral muscles, especially multifidus, were involved in spinal stability and function.4,5 Injury and atrophy of the multifidus muscle may also lead to decreased trunk muscle strength and late-onset spinal instability.6,7 However, the most significant factor responsible for muscle injury is likely powerful self-retaining retractors. 8 Kawaguchi et al quantified the factors that definitely contribute to muscle necrosis after posterior lumbar surgery. They proposed that injury is caused by a crush mechanism. During the use of the self-retaining retractor, increased pressure results in reduced intramuscular perfusion.9–12 The severity of the muscle injury is related to the degree of the intramuscular pressure and the length of retraction time. They concluded that releasing the retractor intermittently during a long surgery, as well as a relatively long incision, can reduce the retractor pressure and thus muscle injury.13–15
If the surgical robot is applied in the surgical retractor and the muscle is retracted during the operation with the robot-assisted retractor, theoretically, not only the labor cost of the surgical assistant during the operation can be reduced, but also the displacement of the retractor and the detachment of the retracted muscle due to fatigue during the operation can be reduced by the precise control of the retractor by the robot. If the operation mode of the surgical robot can be used to intermittently relax the retractor, the purpose of reducing muscle injury can be achieved by adjusting the operation mode. However, as far as we know, research on robot-assisted retractors is still relatively limited. Therefore, this study developed an experimental platform for a robot-assisted retractor and compared the muscle injuries between the intermittent relaxation mode and the continuous retraction mode, as well as the operation of the robot through this platform, aiming to evaluate the feasibility and effectiveness of robot-assisted retractor, and find out a more minimally invasive robot-assisted retractor operation mode. It provides a theoretical basis for the subsequent development of robot-assisted retractor.
Materials and methods
Surgical procedure and operation mode
Three Beagles (at an average age of 0.9 years, 9.25 kg in weight) were provided by Beijing Marshall Biotechnology Co.,Ltd. A veterinarian ruled out spine disorders prior to the start of the study. The dogs were kept the ambient temperature (24 °C–26 °C) and humidity (30%–50%) constant. The dogs had free access to water and food. The study was conducted with the approval of the Ethics Committee.
Each dog was fasted for 12 h and was walked prior to each anesthetic episode and procedure. The animals were anesthesia by using a combination of ketamine (5 mg/kg intravenous) and dexmedetomidine hydrochloride (0.01 mg/kg intravenous). The animals were intubated and maintained under isoflurane (1.5 %) anesthesia.
The skin was disinfected and incised along the midline of the lumbar region. Three 4 cm median incisions was made in the dorsal fascia. Then the bilateral multifidus muscles were separated from the bony structures by utilizing an electrical scalpel and bluntness separation, similar to most posterior lumbar spine surgeries. The lamina was exposed using two different operation modes. (1) The intermittent retraction mode (Mode I): Every 15 min of retraction, the robotic arm moved back to the starting point to relax the retractor. After 3 min of relaxation, the robot retracted the muscle and then travelled back for 15 min before relaxing again, according to the method described by Kotil et al.
16
The cycle was repeated until the total retraction time reached 90 min (2) The continuous retraction mode (Mode C): After the robot retracted the muscle tissue, it continued the retraction for 90 min without any relaxation process (Figure 1) (Supplemental Figure 1). Position of the robot-assisted retractor system and the Beagle dog.
Equipment information
The robot-assisted retractor experimental platform consists of a robotic arm system (LBR Med. 14 R820, KUKA Robotics Co., Ltd, Germany) with KUKA control unit and accessories, a retractor and a self-designed control program. The control program is compiled on Sunrise Workbench and then transferred to the control unit to control the robotic arm (Figure 2). The realistic scene of the robot-assisted retractor system and the KUKA robotic arm system. 1 KUKA robotic arm; 2 smartPAD; 3 KUKA control unit; 4 the shape of the retractor.
Sample preparation and HE staining
After the operation, the muscle sample obtained in each patient was excised from the retractor–muscle contact surface, and it was 10 × 10 × 1 mm in size. The samples were separated and fixed in 10% neutral buffered formalin. After fixation, the specimens were dehydrated with gradient alcohol, transparentized, soaked in paraffin and embedded to be prepared into paraffin block. Each paraffin block was sliced into 3-4 sections (5 μm thick) using the paraffin slicing machine and baked at 70°C for 60 min, followed by deparaffinisation, hydration, HE staining, dehydration, transparency and sealing with neutral balsam. After staining, the sections were observed under an optical microscope (200×) and the lesion site was photographed using the photography system.
Quantitative analysis
The area of muscle injury, including degeneration, bleeding, necrosis, and inflammation, according to the classification described by Hu et al. 17 The total cross-sectional area were determined in the samples using Image-pro plus 6.0 (Media Cybernetics, Inc., Rockville, MD, USA). The muscle injury area is calculated by summing together different sorts of injury areas. Histopathological changes in muscle tissue were scored according to the percentage area of the muscle injury.
Statistical analysis
All quantitative data are expressed as the mean ± standard deviation. Parametric test statistics (paired samples t test) were used to identify differences in muscle injury caused by the two types of retracting. Prior to analysis, data normality was tested by the Shapiro-Wilk test. We considered p-values of <0.05 to be significant. All statistical analyses were performed using GraphPad Prism v9.0.0 (GraphPad, California, USA).
Results
Operation of the robot
The robot-assisted retractor experimental platform was able to precisely retract the muscle into the intended retraction position in both operating modes and hold it stably in the retraction position. During the retraction process, the retractor did not shift and the retracted muscle did not protrude from the retractor. No malfunctions or dangerous actions were detected during operation of the experimental platform.
Histology of the retracted muscle
Histological evaluation showed that the muscle fiber structure in the intermittent retraction mode group was generally normal, while a few were slightly abnormal. The arrangement of muscle fibers was also generally normal, while a few were slightly disordered. No significant degeneration of muscle cells was observed and a small amount of red blood cells was observed in the muscle interstitium as indicated by the black arrows (Figure 3). Photomicrograph of the paravertebral muscle tissue in the intermittent-retraction mode group (Mode I) , HE 10 × 20.
In the continuous retraction mode group, the muscle fiber structure was generally highly abnormal, with disordered arrangement of muscle fibers, necrosis, cytolysis and disappearance of extensive muscle fibers, and only uniformly stained red structures were visible, as indicated by the red arrow. The surrounding muscle fibers atrophy, as indicated by the yellow arrows. Hemorrhages and neutrophil infiltrations were also visible, as shown by the black arrows (Figure 4). In some specimens, the muscle cells were pathologically calcified. Photomicrograph of the paravertebral muscle tissue in the continuous-retraction mode group (Mode C) , HE 10 × 20.
Quantitative analysis
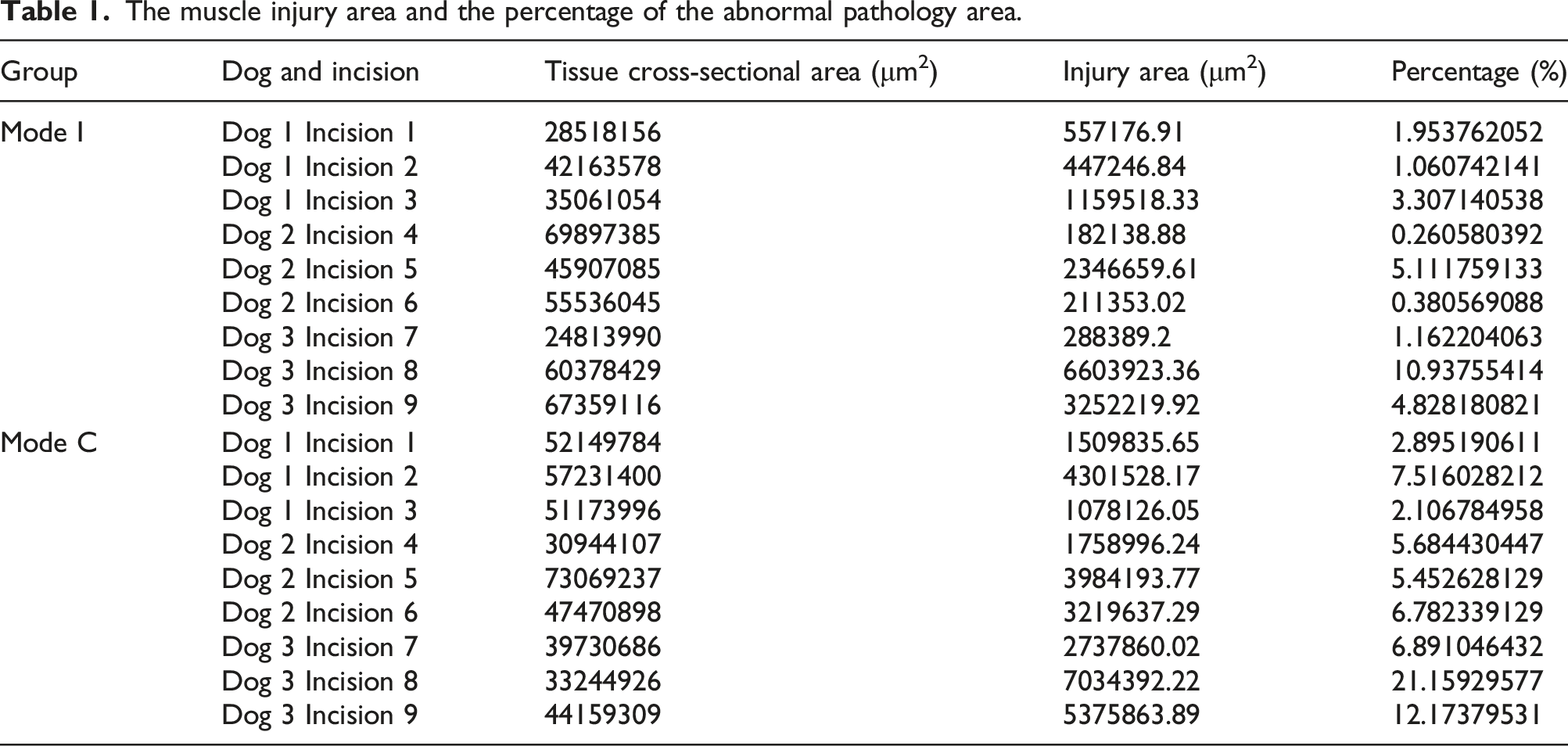
The muscle injury area and the percentage of the abnormal pathology area.
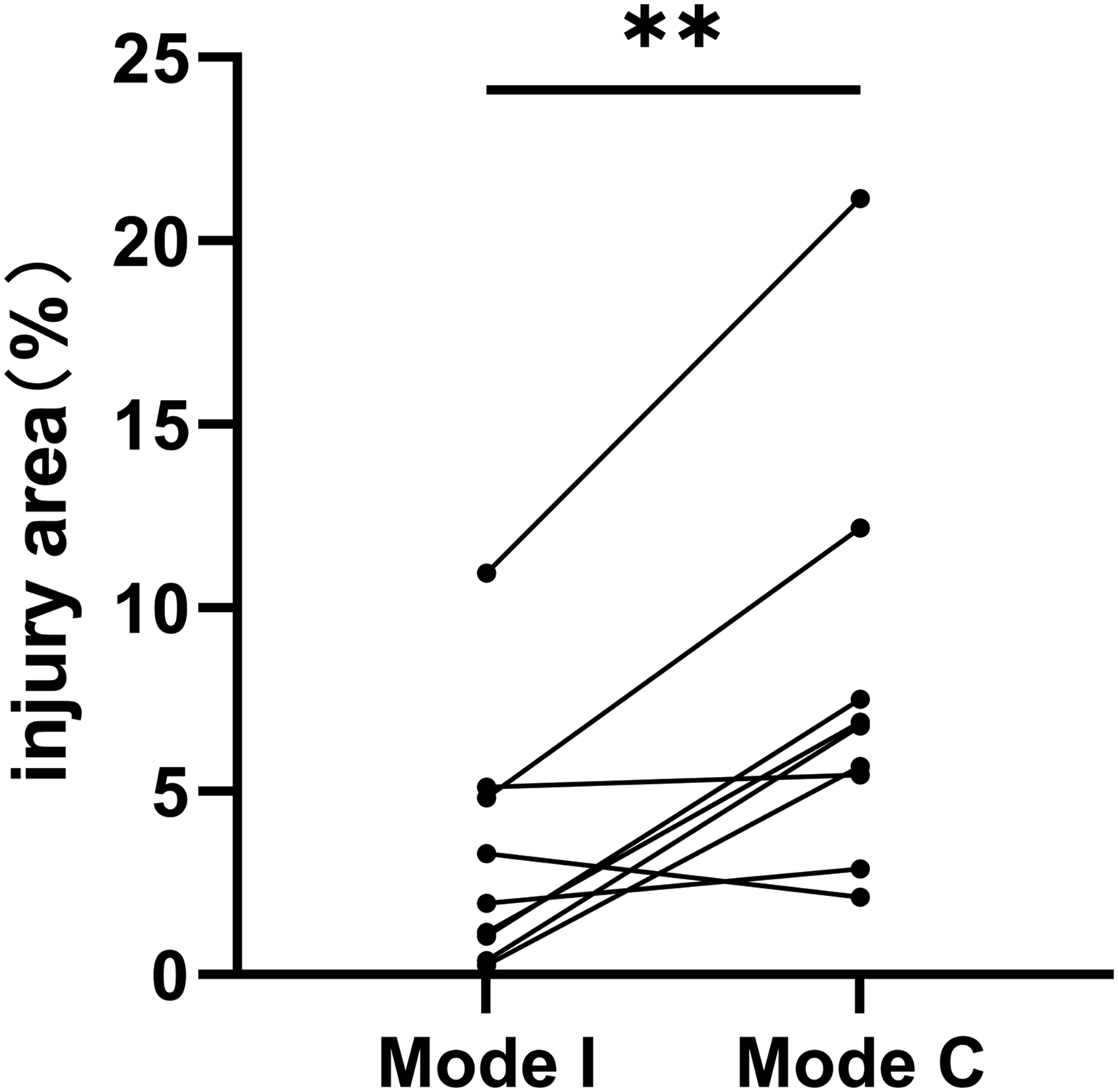
The percentage of the muscle injury area in intermittent-retraction mode group (Mode I) and continuous-retraction mode group (Mode C).
Discussion
Spine robotics has so far primarily been used for pedicle screw fixation. As several studies have demonstrated, one benefit of spine robotics is its ability to increase pedicle screw fixation accuracy. 18 The prerequisites for retracting the muscle during spine surgery, however, are not met by the spine robotic systems that are currently in use. Throughout the clinical practice of our center, we found that surgical assistants still have a lot of auxiliary work to perform during spine surgeries, and one of the most crucial ones is muscle retraction. Long-term retraction state maintenance by assistants can wear them out, which can compromise the retraction’s stability and cause the retractor to move. Additionally, the assistant’s posture during the procedure obstructs their best view, which results in poor control of the retractor and a lack of visual position information. This can cause the retractor to become displaced, which can affect the operation process by causing the retracted tissue to extrude outside of it.
Consequently, this study proposed a new idea of a robot-assisted retractor system, designed a feasible robot-assisted retractor experimental platform and a robot retraction operation mode that reduced muscle injury, and proved through the animal experiments that: the use of intermittent-retraction mode in the robot-assisted retractor could reduce the muscle injury, and had the advantages of precise positioning and stable operation. At the same time, the robot could reduce the workload of surgeons during the surgery process, improving the comfort and efficiency of the surgery.
A first aim of this study was to verify the feasibility and safety of the robot-assisted retractor system. The robot-assisted retractor is still merely at the conceptual stage, and no pertinent studies have been conducted to assess its viability and safety. Our group created an experimental platform for robot-assisted retractors in order to conduct further research on the technology and confirm its viability and efficacy in animal trials for surgical procedures. Accordingly, our study demonstrates that the robot-assisted retractor system is capable of precisely retracting the muscle back to its predefined position and keeping it there steadily without experiencing any malfunctions or other events that could jeopardize surgical safety. This suggests that robot-assisted retractors demonstrate a degree of feasibility and safety, and have potential for future comprehensive investigation.
A second aim was to demonstrate the potential of the robot-assisted retractor system in minimizing surgical invasiveness through the implementation of suitable operating modes. Multiple investigations have demonstrated that the utilization of self-retaining retractors has the potential to induce paravertebral muscle injury, typically characterized by the presence of low back discomfort and dysfunction.3,8,13–15 By implementing a rational operation mode on the robot-assisted retractor, it becomes feasible to achieve automated functionality, resulting in reduced labor requirements and mitigated risk of muscle injury. Consistent with prior findings, it has been observed that periodically releasing the retractor during surgical procedures helps mitigate muscle damage.11,16,19,20 This study presents empirical evidence indicating that histological evaluation reveals a lower presence of structural abnormalities, disordered arrangement, degeneration, hemorrhage, and neutrophil infiltration in the group subjected to the intermittent-retraction mode. We also endeavored to assess the magnitude of the muscle injury by determining the fraction of muscle injury areas present on each specimen. The mean percentage of muscle injury sites in the intermittent-retraction mode group was 3.22% ± 3.41, which was significantly lower than the continuous-retraction mode group with an average percentage of 7.85% ± 5.77 (p = .006). The findings suggest that the intermittent-retraction mode employed by the robot-assisted retractor system is capable of reducing muscle injury. The utilization of the robot-assisted retractor demonstrates the potential benefits it offers, such as the ability to conduct minimally invasive and precise surgery through precise program control and the flexible capabilities of the robotic arm.
However, this study is in its early stages, and has some limitations. Currently, because to the preliminary nature of our research, the robot-assisted retractor experimental platform developed in our study does not possess the level of maturity required for direct utilization in surgical procedures. This tool is primarily intended for preliminary study pertaining to retractors supported by robots. The existing experimental platform is limited in its ability to perform only pre-determined operational modes for studies. It exhibits a lesser level of automation when compared to well-established surgical robots. Additionally, its functionality requires improvement as it lacks optimization for real-world clinical scenarios. In forthcoming endeavors, we intend to enhance both the hardware and software design in order to attain heightened levels of precision and intelligence in control mechanisms. We aim to further investigate the possibilities of robot-assisted spinal surgery, thereby expanding our understanding of its potential. In the future, it will be necessary to create an enhanced security mechanism for the robot system in order to ensure increased security redundancy. Additionally, due to facility constraints, we only collected samples immediately post-surgery and did not raise or collect experimental animals for a period following surgery, leading to limited study on the regeneration of the damaged muscles. We will investigate the regeneration of the damaged muscles in future studies on muscle injury in robot-assisted retractor surgery to improve the comprehensiveness of our research.
Currently, the focus of this project lies in the development of a robot-assisted retractor system specifically designed for posterior spine surgery. Nevertheless, there is potential for the expansion of its practicality to include spine surgery and even orthopedic surgery, as there are notable commonalities between these fields. Both spine surgery and orthopedic surgery typically require the retraction of muscles in the surgical site during the procedure. This implies that the robotic technology possesses considerable potential for applicability in various other orthopedic surgical procedures.
In conclusion, the findings from the studies conducted on beagle dogs provide first validation for the precision and safety aspects of the robot-assisted retractor. This study offers crucial evidence to support the further advancement of research on robot-assisted retractors and their potential clinical implementation in the future. This study provides concurrent validation of the efficacy of utilizing the intermittent-retraction mode in the robot-assisted retractor for the purpose of mitigating muscular injury resulting from the use of retractors. This study serves as a valuable resource for informing the development of future modes of operation for robot-assisted retractor systems.
Supplemental Material
Supplemental Material - Robot-assisted retractor in spine surgery: Preliminary evaluation of its feasibility and two operation mode in beagles
Supplemental Material for Robot-assisted retractor in spine surgery: Preliminary evaluation of its feasibility and two operation mode in beagles by Yuzhen Jiang, Lei Xiang, Da He and Wei Tian in Journal of Orthopaedic Surgery
Footnotes
Author contributions
Protocol/project development, conduction of experiments, data collection and management, data analysis, manuscript and figure writing: Yuzhen Jiang. Conduct of experiments, data collection and management: Yuzhen Jiang and Lei Xiang. Critical revision to the original manuscript: Da He. Protocol/project development and supervision: Wei Tian. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (U1713221) and Chinese Academy of Medical Sciences Innovation Project for Medical and Health Science and Technology (2021-I2M-5-007).
Ethics approval
Ethical approval was obtained from the Ethics Committee of Beijing Jishuitan Hospital (approval number: 2022-08-008). All methods were carried out in accord-ance with relevant guidelines and regulations. The study was carried out in compliance with the ARRIVE guidelines.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.