
Abstract
Background
Unicompartmental knee arthroplasty (UKA) is an effective treatment method for knee osteoarthritis. With the development and implementation of enhanced recovery after surgery, UKA is now increasingly performed in outpatient surgical centers. However, there is ongoing debate regarding the safety and effectiveness of performing UKA in outpatient settings.
Methods
The search was performed to retrieve randomized controlled trials and cohort studies on outpatient UKA from PubMed, Cochrane Library, EMbase, CNKI, and WanFangData databases. The search was conducted from the inception of the databases until August 31, 2023. After independent screening, data extraction, and risk of bias evaluation by two researchers, meta-analysis was performed using RevMan 5.4 software.
Results
A total of eight studies involving 18,411 patients were included. The results showed that the postoperative transfusion rate in the outpatient group was lower than that in the inpatient group [OR = 0.36, 95%CI (0.24, 0.54), p < 0.00001], and the difference was statistically significant. However, there was no significant difference between the two groups in terms of readmission rate, reoperation rate, surgical site infection, and periprosthetic fracture. The differences were not statistically significant.
Conclusion
Compared to the traditional inpatient route, the blood transfusion rate for single-condyle replacement in the outpatient operation center is lower, and there is no significant difference in readmission rate, reoperation rate, surgical site infection, and periprosthesis fracture. The outpatient approach to UKA is safe, feasible, and highly satisfactory for patients. However, the results have certain limitations, and a rigorous preoperative complication risk assessment can minimize the risk of UKA in outpatient surgery centers.
Trial registration
PROSPERO number CRD42023405373.
Background
Osteoarthritis (OA) is a prevalent degenerative joint disease that affects middle-aged and elderly populations worldwide. It commonly affects joints such as the knee, hip, and finger joints. 1 Knee osteoarthritis (KOA) is one of the most commonly affected joints, leading to knee pain, deformity, and disability in patients. This severely affects the quality of life of middle-aged and elderly populations and imposes a significant economic burden on patients and society. 2 Symptomatic conservative treatments are inadequate in preventing or reversing the progression of KOA. For patients with advanced KOA, knee joint replacement remains one of the most effective treatment options. 3 Currently, the primary methods of knee joint replacement are total knee arthroplasty (TKA) and unicompartmental knee arthroplasty (UKA). 4 Compared to TKA, UKA only replaces the articular surface of the affected compartment, preserving natural bone mass and cruciate ligaments, not disrupting the proprioception of the knee joint, having biomechanics closer to that of a natural knee joint, and offering advantages such as lower hospitalization costs, smaller surgical trauma, shorter operation time, lower mortality rate, and faster recovery of joint function. 5 With the increasing popularity of knee preservation concepts, more and more orthopedic surgeons prioritize UKA when formulating surgical plans. Additionally, research has shown that 85% of knee joint degeneration primarily accumulates in a single compartment, and the proportion of patients suitable for UKA exceeds 49%. 6
The concept of surgical accelerated rehabilitation aims to utilize evidence-based medical interventions to reduce surgical trauma and postoperative complications, shorten hospital stays, alleviate economic burden, improve surgical safety, patient satisfaction, and achieve the goal of accelerated recovery. 7 Orthopedics, as one of the earliest fields to apply this concept, has undergone years of development and improvement to shorten hospital stays, reduce costs, and improve patient satisfaction. Total hip and knee arthroplasty, including UKA, has been performed in outpatient surgical centers in many places, which has also garnered attention and discussion from orthopedic scholars. 8 Studies have shown that outpatient UKA is safe and feasible, does not increase the incidence of complications, and can improve patient satisfaction, surgical outcomes, and significantly save medical resources. 9 However, some scholars have expressed concerns about complications, postoperative pain, and infections in patients undergoing outpatient UKA, and studies have shown that 20% of patients undergoing outpatient UKA have extended hospital stays due to complications. 10 Currently, there is limited relevant clinical research and no published evidence from systematic reviews on the incidence of complications and revision rates of outpatient UKA, leading to ongoing debates. Therefore, this study aims to conduct a meta-analysis and systematic review of the safety and effectiveness of outpatient and traditional approaches to UKA, in order to provide evidence-based medicine for clinical practice.
Data and methodology
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 11 for design and implementation. The protocol for this review has been registered in PROSPERO (registration number CRD42023405373).
Retrieval strategy
We conducted a systematic search in Pubmed, EMbase, TheCochraneLibrary, CNKI, WanFangData, and VIP databases. The search strategy was as follows: ① “Ambulatory Surgery ” OR “Outpatient Surgery ” OR “ Outpatient Surgeries” OR “Surgeries, Outpatient” OR “Surgery, Outpatient” OR “Procedure, Ambulatory Surgical” OR “Procedures, Ambulatory Surgical” OR “Surgical Procedure, Ambulatory” OR “Surgical Procedures, Ambulatory” OR “Surgery, Ambulatory” OR “Ambulatory Surgeries” OR “Surgeries, Ambulatory” OR “Ambulatory Surgical Procedure” OR “Surgery, Office” OR “Office Surgery” OR “Office Surgeries” OR “Surgeries, Office” OR “Surgery, Day” OR “Day Surgeries” OR “Surgeries, Day” OR “Day Surgery”; ② “Unicompartmental Knee Arthroplasty” OR “Arthroplasty, Unicompartmental Knee” OR “Knee Arthroplasty, Unicompartmental” OR “Unicondylar Knee Arthroplasty” OR “Arthroplasty, Unicondylar Knee” OR “Knee Arthroplasty, Unicondylar” OR “Partial Knee Arthroplasty” OR “Arthroplasty, Partial Knee” OR “Knee Arthroplasty, Partial” OR “Unicondylar Knee Replacement” OR “Knee Replacement, Unicondylar” OR “Partial Knee Replacement” OR “Knee Replacement, Partial” OR “Unicompartmental Knee Replacement” OR “Knee Replacement, Unicompartmental”. The retrieval period is from the establishment of the database to August 2023, and relevant reviews and included references are traced to supplement the retrieval of relevant literature.
Research selection
Including the following criteria for the study: (1) Study design: Randomized controlled trials (RCTs), case-control studies, and cohort studies. (2) Study population: Patients with knee osteoarthritis (KOA) who underwent UKA, regardless of age, gender, race, nationality, and disease duration. (3) Intervention: Experimental group: UKA treatment through outpatient approach; Control group: UKA treatment through inpatient approach. (4) Outcome measures should include at least one of the following indicators: Primary indicators: ① Readmission within 90 days; ② Reoperation within 90 days; Secondary indicators: ③ Surgical site infection; ④ Perioperative blood transfusion; ⑤ Periprosthetic fracture. The following studies are excluded based on the following criteria: (1) Duplicate publications; (2) Literature with incomplete data or unable to extract data; (3) Systematic reviews, letters, comments, conference abstracts, case reports, and animal experimental studies.
Data extraction and quality assessment
The literature was independently screened and data were extracted by two researchers according to the inclusion and exclusion criteria. Any disagreements were resolved through discussion or consultation with the corresponding author. The extracted data included: (1) basic information of the included studies, such as study title, first author, publication date, study type, and follow-up time; (2) baseline characteristics of the study subjects and intervention measures; (3) key elements of bias risk assessment; (4) outcome measures of interest and data on outcome measurement. The risk of bias in the included randomized controlled trials was assessed using the Cochrane Collaboration tool. 12 The Cochrane Collaboration tool includes seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other sources of bias. Each domain is classified as low, high, or unclear risk of bias. The risk assessment of included non-randomized controlled trials was conducted using the Newcastle-Ottawa Scale (NOS). 13 The assessment scale includes three domains: selection of study groups, comparability, and exposure (case-control studies) or outcome (cohort studies). The score ranges from 0 to 9, and studies with a score of six or above are considered high-quality studies.
Statistical analysis
Statistical analysis was conducted using RevMan (version 5.4; Cochrane, Oxford, UK) and Stata (version 12.0; Stata Corporation) software. Odds ratios (OR) or risk ratios (RR) with 95% confidence intervals (CI) were utilized as statistical measures for analyzing complications in categorical variables. Mean differences (MD) or standardized mean differences (SMD) with 95% CI were used for continuous variables. A p-value less than 0.05 was considered statistically significant. The I2 statistic was used to assess the magnitude of heterogeneity (low <50%, moderate 50%–74%, high >75%). A p-value ≥0.05 and I2 < 50% indicated no statistical heterogeneity among studies. If heterogeneity was moderate or high, a random-effects model was employed. Subgroup analysis or sensitivity analysis was conducted to address significant clinical heterogeneity. If the source of heterogeneity could not be identified, only descriptive analysis was performed.
Result
Literature Screening Process and Results
According to the above retrieval strategy, a total of 1308 relevant articles were obtained (including 200 articles from PubMed, 656 articles from Cochrane Library, 446 articles from Embase, and six articles through other sources). After removing duplicate articles, 1212 articles were obtained. After reading the titles and abstracts, 1170 studies were excluded. Finally, after reading the full text, eight retrospective cohort studies14–21 were included. All articles can be subjected to quantitative analysis, with a total of 18,411 subjects (based on the number of knees). The literature screening process and results are shown in Figure 1. Literature screening process and results.
Basic characteristics and bias risk assessment results included in the study
The Characteristics of the included studies and quality assessment results of the included studies.
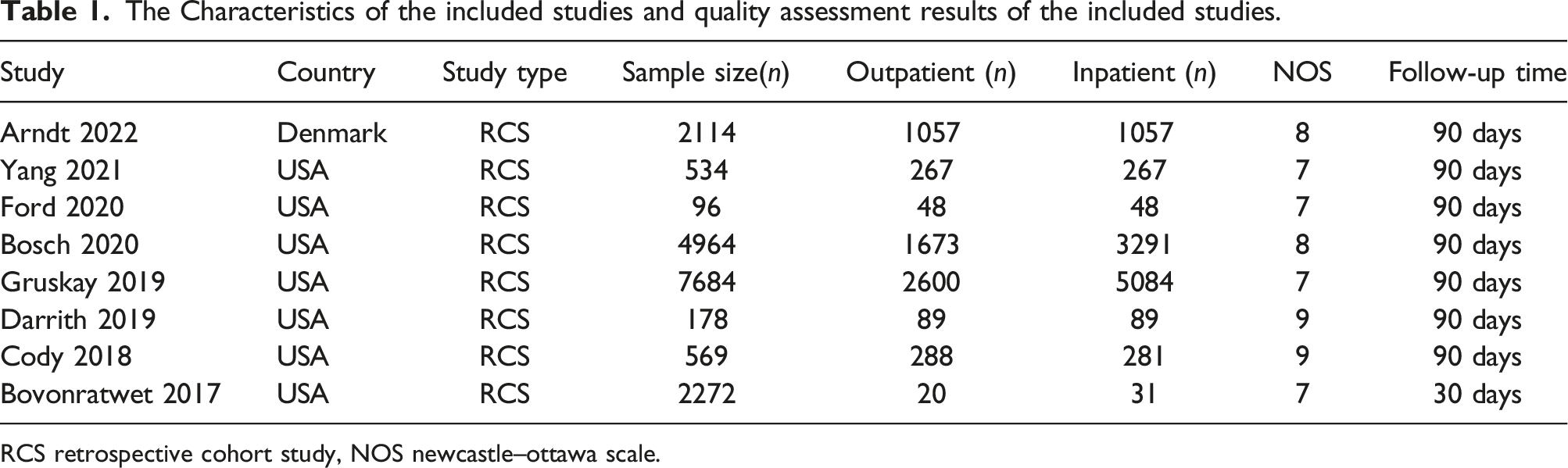
RCS retrospective cohort study, NOS newcastle–ottawa scale.
Meta-analysis results
Readmission rate
A total of seven queue studies were included.14–20 Statistical heterogeneity of the included studies was assessed using tests based on the values of P and I2. I2 = 46%, p = 0.09, indicating low heterogeneity among the results of the included studies (I2 < 50%). The random effects model was used to evaluate the results. The results showed no statistically significant difference in rehospitalization between the outpatient group and the inpatient group [OR = 1.02, 95%CI(0.72,1.44), p = 0.96] (Figure 2). Forest plot of Readmission rate.
Reoperation rate
A total of five queue studies15,16,18–20 were included. Statistical heterogeneity of the included studies was assessed using tests based on the values of P and I2. I2 = 0%, p = 0.41, indicating low heterogeneity among the results of the included studies (I2 < 50%), and a fixed-effect model was used to evaluate the results. There was no statistically significant difference in reoperation between the outpatient group and the inpatient group [OR = 1.21, 95%CI(0.76, 1.94), p = 0.56] (Figure 3). Forest plot Reoperation rate.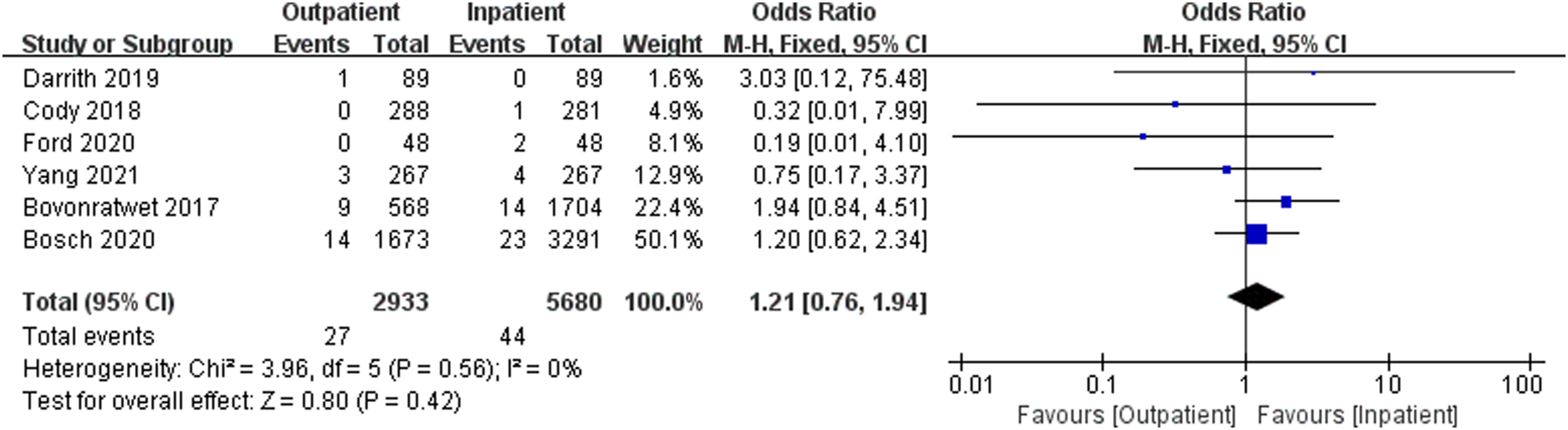
Surgical site infection
A total of six queue studies15–18,20,21 were included. Statistical heterogeneity of the included studies was assessed using tests based on the values of P and I2. I2 = 0%, p = 0.84, indicating low heterogeneity among the results of the included studies I2 < 50%), and a fixed-effect model was used to evaluate the results. There was no statistically significant difference in reoperation between the outpatient group and the inpatient group [OR = 1.36, 95%CI(0.97, 1.91), p = 0.07] (Figure 4). Forest plot Surgical site infection.
Transfusion rate
A total of three queue studies17,20,21 were included. The statistical heterogeneity of the included studies was evaluated using tests based on the values of P and I2. I2 = 31%, p = 0.24, indicating low heterogeneity among the results of the included studies (I2 < 50%), and a fixed-effect model was used to evaluate the results. The results showed that the postoperative transfusion rate in the outpatient group was lower than that in the inpatient group, and the difference was statistically significant [OR = 0.36, 95%CI(0.24, 0.54), p < 0.00,001] (Figure 5). Forest plot Transfusion rate.
Periprosthetic fracture
A total of four queue studies15,16,18,19 were included. The statistical heterogeneity of the included studies was evaluated using tests based on the values of P and I2. I2 = 0%, p = 0.51, indicating low heterogeneity among the results of the included studies (I2 < 50%), and a fixed-effect model was used to evaluate the results. There was no statistically significant difference in the incidence of deep vein thrombosis between the outpatient group and the inpatient group [OR = 0.41, 95%CI(0.12, 1.42), p = 0.16] (Figure 6). Forest plot Periprosthetic fracture.
Discussion
Compared to total knee arthroplasty (TKA), unicompartmental knee arthroplasty (UKA) only replaces the joint surface of the affected compartment, without entering the bone marrow cavity and preserving the cruciate ligament. UKA offers advantages such as reduced surgical trauma, less intraoperative bleeding, faster recovery of joint function, fewer postoperative complications, improved proprioception, and lesser joint awareness.22,23 As joint prostheses have improved, surgical techniques have been updated, and indications have been better understood, the functional outcomes of UKA have significantly improved. The survival rate of implants has gradually increased, and UKA is now considered the ultimate solution for end-stage osteoarthritis involving only the affected compartment. 24 As UKA has developed and improved, its application proportion in KOA patients has gradually increased. 25 In recent years, reducing the cost and complications of UKA while improving patient satisfaction has become a research hotspot. Enhanced recovery after surgery in orthopedics has attracted attention and promotion worldwide due to its advantages, including improving patient satisfaction, reducing perioperative complications, and saving medical resources. This approach has been successfully applied in many surgical fields. 26 As one of the earliest fields to implement enhanced recovery after surgery, the orthopedic field has achieved a significant reduction in hospitalization time and cost, as well as a continuous improvement in patient satisfaction after surgery. Some clinical research centers have performed hip and knee arthroplasty, including UKA, in outpatient surgery centers. 27 However, there is still controversy surrounding the safety and effectiveness of UKA in outpatient surgery centers. This study aims to compare the safety and effectiveness of UKA in outpatient surgery centers and traditional inpatient approaches. The study will include indicators such as readmission rate, reoperation rate, surgical site infection, transfusion rate, deep vein thrombosis, postoperative pneumonia, myocardial infarction, and periprosthetic fracture. These indicators will reflect the early surgical outcomes of UKA under different approaches, providing reliable data for evaluating the safety and effectiveness of the two different surgical approaches.
The readmission rate and reoperation rate are crucial indicators for evaluating the safety and effectiveness of outpatient UKA procedures. Higher readmission and reoperation rates can negatively impact surgical outcomes and postoperative recovery, reduce patient satisfaction, and increase the economic burden on patients. Our study results indicate that there is no statistically significant difference in readmission and reoperation rates within 90 days after surgery between the outpatient and inpatient groups. This suggests that the impact of outpatient UKA on early readmission and reoperation is not significant. However, the length of hospital stay is directly related to the patient’s treatment costs. Studies have shown that outpatient UKA can reduce costs by approximately 50%, 28 thereby reducing the economic burden on patients and society, decreasing bed occupancy, and facilitating the allocation and utilization of medical resources.
Surgical site infection is one of the most concerning complications in joint replacement surgery, causing fever, pain, and prosthesis loosening. This increases the risk of further surgery, treatment costs, and medical resource utilization. 29 Our study found no statistically significant difference in surgical site infection incidence between the outpatient and traditional groups. This suggests that outpatient UKA does not increase the risk of surgical site infection, possibly due to perioperative single-dose antibiotic prophylaxis. Despite new infection prevention strategies, antibiotic prophylaxis remains crucial for postoperative surgical site infection prevention. 30 CodyCW et al. 31 showed that outpatient UKA patients receiving single-dose antibiotic prophylaxis before skin incision had a similar infection incidence as hospitalized patients receiving 24-h prophylaxis. This demonstrates that single-dose intravenous antibiotic prophylaxis is a safe practice for outpatient UKA, consistent with our study results.
Due to the minimal blood loss and small trauma associated with UKA, the use of tourniquets during surgery can result in ischemia-reperfusion injury and the release of a significant amount of inflammatory factors, leading to abnormal coagulation function and a decrease in postoperative hemoglobin due to hidden blood loss. 32 Blood transfusion is a common treatment measure for patients with low hemoglobin levels, but it can also cause various adverse reactions such as transfusion-related hemolysis, fever, and allergies, which can harm the patient’s health and even threaten their life. 33 Blood transfusion for patients undergoing knee arthroplasty, whether autologous or allogeneic, increases costs, carries the risk of disease transmission and transfusion reactions, and is associated with an increased incidence of periprosthetic infection. 34 Our research results indicate that the transfusion rate in the outpatient group is lower than that in the inpatient group during the 90-days follow-up after surgery. This finding can reduce the occurrence of adverse reactions in patients caused by blood transfusion, promote rapid postoperative recovery, and reduce treatment costs for patients. However, the different surgical approaches do not affect the surgical process and hemostasis measures. The lower transfusion rate in the outpatient group in this study may be attributed to two possibilities. First, patients who require blood transfusion in the outpatient surgical approach may be transferred to inpatient treatment. Second, it is possible to detect postoperative invisible blood loss in the inpatient approach, including residual blood in the knee joint, blood seepage into tissues, and blood loss caused by hemolysis. 35
Periprosthetic fractures have a significant impact on hospitalization duration, with a readmission rate exceeding 20% within 90 days after occurrence. 36 The incidence of periprosthetic fractures following UKA is relatively low, accounting for approximately 2% of UKA failures. This may be attributed to postoperative lower limb alignment, implant position, and osteotomy level. 37 Our study findings indicate that there is no statistically significant difference in the incidence of periprosthetic fractures between the outpatient and inpatient groups. This suggests that outpatient UKA does not increase the risk of periprosthetic fractures.
Due to its advantages of minimal trauma, short operation time, and rapid recovery, unicompartmental knee arthroplasty (UKA) results in mild postoperative pain for patients. Research has indicated that patients experience peak pain on the third day after surgery, which gradually decreases to normal levels. In cases where postoperative oral analgesia is required, only one out of 56 patients needed to be readmitted due to pain, and over 90% of patients expressed satisfaction with UKA. 38 Furthermore, studies investigating patient satisfaction after outpatient UKA surgery found that 76.2% of patients expressed complete satisfaction, while the remaining 23.8% expressed general satisfaction. Additionally, 90.5% of patients who underwent UKA reported that they would prefer outpatient surgery to in-hospital arthroplasty if they had to undergo the procedure again. 39
Research statistics indicate that the cost of outpatient treatment for UKA in the UK is $20,500 less than the average cost of inpatient treatment. This cost difference can be attributed to the lower cost of outpatient surgical facilities. 28 Another study found that the cost of UKA in outpatient clinics was significantly lower ($11,723.04 ± 8097.19) than that of inpatients ($14,209.20 ± 10,265.77). 21 An increasing number of studies demonstrate that outpatient UKA practice can significantly reduce treatment costs for patients, thereby alleviating economic pressure and enabling more patients to seek timely medical attention. Furthermore, outpatient UKA practice can also improve the efficiency of ward bed utilization, allowing us to serve more patients.
Our research findings suggest that there is no significant difference in the early safety and efficacy between outpatient and traditional approaches for UKA, indicating that the outpatient approach is a safe and feasible option. Patients who undergo UKA through the outpatient approach can be discharged on the same day of surgery, resulting in lower costs and higher satisfaction. However, the outpatient approach may not be suitable for all patients due to variations in their health conditions. 40 Therefore, it is crucial to evaluate the risk of complications in patients before surgery and before discharge to minimize perioperative risks. The primary challenge in promoting outpatient UKA is how to screen and assess the potential risks of postoperative complications in patients.
Limitations of this study
The limited research on UKA performed through outpatient approaches both domestically and internationally in recent years has resulted in the exclusion of RCTs and a small number of included studies, which may introduce bias to the results. The follow-up time in the included literature of this study was within 90 days after surgery, and a large sample size and high-quality long-term follow-up are still needed to evaluate the effectiveness of the two surgical approaches. Although a large number of patients were included in this study, differences in age, gender, country/region, medical conditions, and postoperative recovery among the studies, as well as incomplete reporting of all baseline characteristics in each study, made it impossible to conduct corresponding subgroup analysis and analysis of heterogeneity sources, which may affect the accuracy of the conclusions.
Conclusion
In summary, current evidence suggests that, apart from a lower blood transfusion rate in the outpatient group compared to the inpatient group, there is no significant difference in the safety and efficacy of outpatient and traditional routes for UKA. The outpatient route for UKA is both safe and feasible, with lower costs and higher patient satisfaction. However, it is important to note that there are certain limitations to these findings. Prior to surgery, the degree of risk for complications must be thoroughly evaluated. Furthermore, for patients with varying health conditions, further multi-center, large-sample, high-quality research is necessary to determine the suitability of outpatient condylar replacement.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Gansu Province (NO.20JR10RA358).