
Abstract
Purpose:
The aim of this study was to assess differences in clinical outcomes and postoperative cartilage repair between opening wedge high tibial osteotomy (OWHTO) and closed wedge HTO (CWHTO) for medial osteoarthritis (OA) of the knee.
Methods:
A total of 90 knees of 76 patients who underwent OWHTO (45 knees of 40 patients) and CWHTO (45 knees of 36 patients) was followed-up for 2 years. Cartilage repair at the medial compartment was arthroscopically classified into the following stages: Stage 1 (no reparative change); Stage 2 (partial coverage with white cartilaginous tissue); and Stage 3 (full coverage with white cartilaginous tissue). Clinical outcomes were assessed using Knee Society scores, and radiographic assessment was carried out by anatomical femorotibial angle (aFTA).
Results:
Regarding preoperative OA grade, varus alignment, and function score, CWHTO patients showed more advanced OA status than OWHTO patients. Knee scores and function scores were significantly improved after surgery with both HTO procedures (P < 0.05), with no significant difference between the two procedures. Cartilage repair of stage 2 or 3 was found in more than 80% of the subjects in the medial femoral condyle and more than 60% in the medial tibial condyle. However, there were no significant differences between the two HTO procedures. Multivariate logistic regression analysis showed that preoperative International Cartilage Repair Society (ICRS) grade was the only factor affecting cartilage repair.
Conclusions:
CWHTO improved clinical outcomes and cartilage status as much as OWHTO. Although the effects of cartilage repair on clinical outcomes are unknown, HTO is an effective treatment option even for severe medial OA of the knee.
Introduction
Osteoarthritis (OA) of the knee is one of the most common diseases affecting the adult knee and is associated with a progressive loss of articular cartilage. Valgus high tibial osteotomy (HTO) is an established procedure in medial compartmental OA of the knee. Proper overcorrection provides pain relief and subsequent improvement of knee function. 1,2 Two commonly used procedures are the closed wedge HTO (CWHTO) and the opening wedge HTO (OWHTO), and excellent clinical outcomes have been reported with both techniques. 3,4
Articular cartilage has high elasticity, load buffering capacity, and durability, but it has poor regeneration ability. It is well known that spontaneous repair of articular cartilage is difficult in OA of the knee. However, previous studies have shown that a regenerative response of articular cartilage was observed in several cases after HTO. 5 –12 These reports involved either OWHTO or CWHTO, and to the best of our knowledge, no study has directly compared postoperative cartilage repair between OWHTO and CWHTO. In addition, it is unclear whether cartilage repair is related to clinical outcomes after these two HTO procedures.
The aim of the present study was to assess differences in clinical outcomes and postoperative cartilage repair between OWHTO and CWHTO. It was hypothesized that the difference in osteotomy techniques between OWHTO and CWHTO affects clinical outcomes and rates of postoperative cartilage repair.
Methods
This retrospective case series study was approved by the institutional review board of Yokohama City University (#B180200061). A total of 90 knees of 76 patients who underwent HTO between 2011 and 2015 were investigated. The inclusion criterion was painful osteoarthritis (OA) localized to the medial compartment of the knee. Exclusion criteria were OA of the lateral compartment, flexion contracture greater than 15°, or a history of inflammatory arthritis, joint infection, or immunosuppressive therapy. The selection of technique was made preoperatively according to the correction angle. OWHTO was performed in 45 knees of 40 patients with a correction angle of 15° or less, and CWHTO was performed in 45 knees of 36 patients with a correction angle of greater than 15°. Demographic data are shown in Table 1.
Demographic data
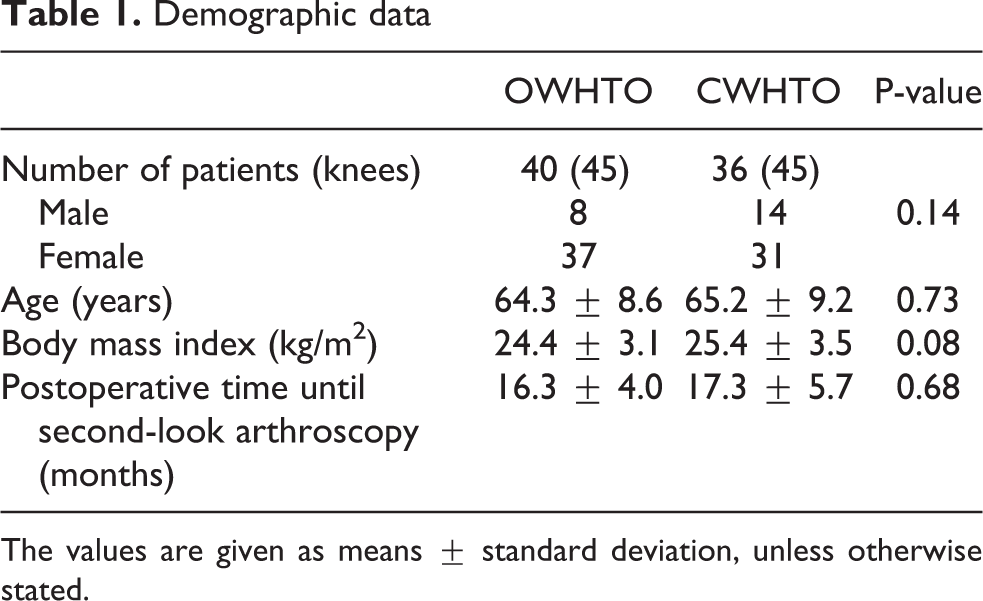
The values are given as means ± standard deviation, unless otherwise stated.
Surgical procedure and postoperative management
The amount of angular correction was planned preoperatively aiming to achieve tibiofemoral anatomical valgus of 10° in a one-leg standing radiograph postoperatively, since good long-term clinical outcomes were expected in this target angle. 2,13,14 The correction angle is limited to 15° or less in OWHTO, 14 whereas a larger correction is possible in CWHTO. The decision for either technique was made preoperatively according to the correction angle based on our institutional protocol. 14 –16 That is, OWHTO (Figure 1(A)) was performed in knees with a correction angle of 15° or less, and CWHTO (Figure 1(B)) was performed in knees with a correction angle of greater than 15°.
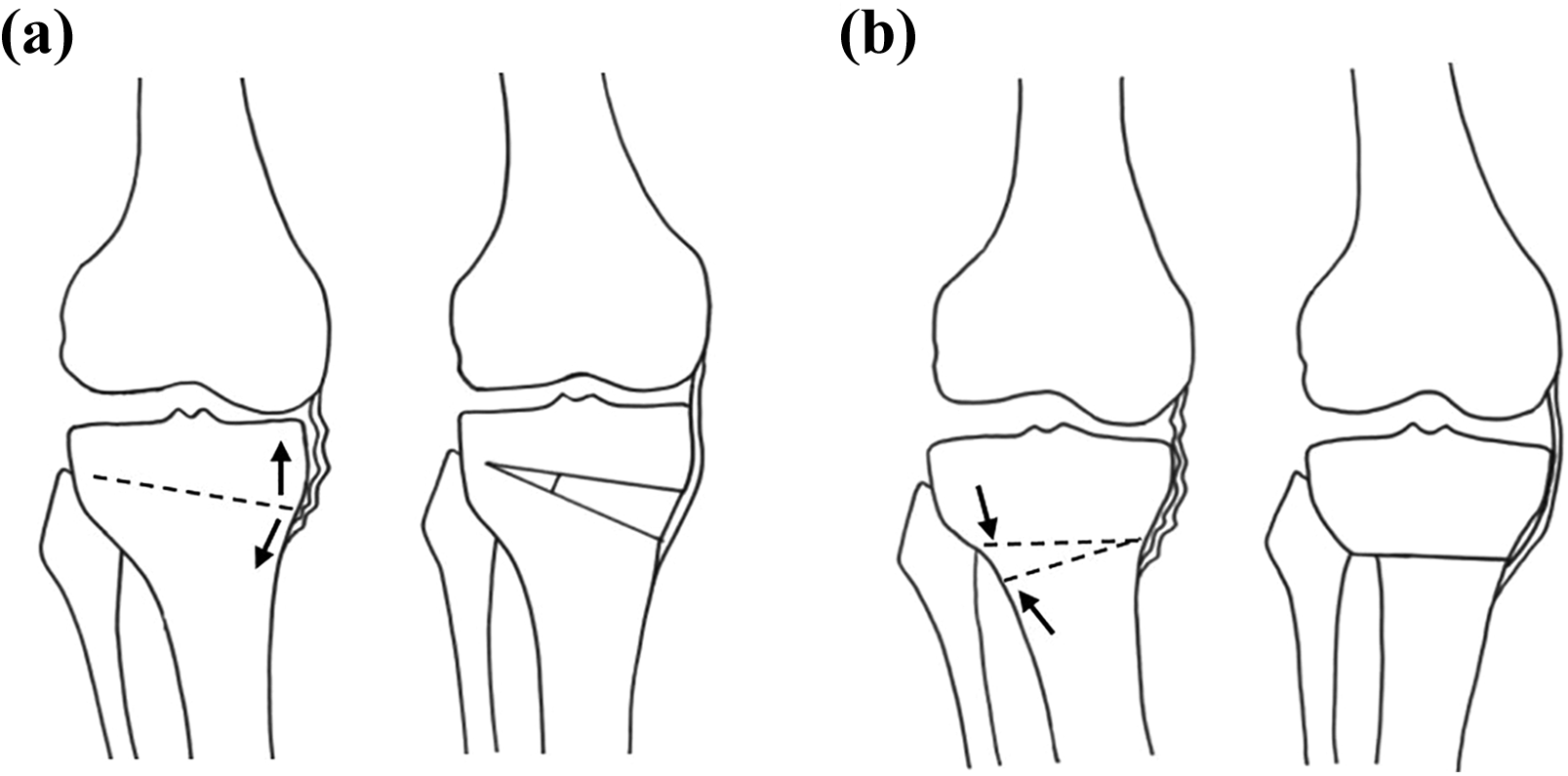
Illustrations of opening wedge (a) and closed wedge (b) high tibial osteotomies.
OWHTO was performed using an anteromedial approach under fluoroscopic guidance. The osteotomy was started 35 mm below the medial articular surface of the tibia. An oblique osteotomy was performed from the medial cortex to the upper third of the proximal tibiofibular joint using biplanar technique, leaving the tibial tuberosity intact. The osteotomized gap was gradually opened and filled with two wedged blocks of β-TCP with 60% porosity (Osferion®, Olympus Terumo Biomaterials. Corp., Tokyo, Japan) and fixed with TomoFix (DePuy Synthes, Zuchwil, Switzerland).
CWHTO was performed using an anterolateral approach under fluoroscopic guidance after fibular osteotomy. The osteotomy was started 30 mm below the lateral articular surface of the tibia. The proximal osteotomy was performed parallel to the tibial plateau, and the distal osteotomy was performed obliquely toward the hinge point of the medial cortex, with a flange to leave the insertion of the patellar tendon with a distal fragment. The osteotomy gap was closed and fixed with an OWL plate (Mizuho Ikakogyo Co., Ltd., Tokyo, Japan).
Patients started a postoperative rehabilitation program including isometric quadriceps and range-of-motion exercises the day after surgery. After CWHTO, a non-weight-bearing regimen was prescribed for 2 weeks, followed by partial weight-bearing exercise, and full weight-bearing exercise was permitted 3 weeks postoperatively. After OWHTO, a non-weight-bearing regimen was prescribed for 1 week, followed by full weight-bearing exercise. Casts or supportive devices were never applied in both procedures.
Assessments of clinical and radiographic outcomes
All subjects were followed-up postoperatively at 2 years to assess clinical and radiographic outcomes. Clinical evaluation was carried out using the Knee Society Score (KSS) 17 before HTO surgery and 2 years after surgery. For radiographic assessment, an anteroposterior weight-bearing radiograph of the knee was taken before HTO surgery and 2 years after surgery, and limb alignment was expressed as the anatomical femorotibial angle (aFTA), measuring the lateral angle between the femoral axis and the tibial axis. 2,18 Assessment of radiographic degeneration was based on Ahlbäck’s classification.
Assessment of articular cartilage
The preoperative status of articular cartilage was examined by arthroscopy at the time of osteotomy. The grade of cartilage injury associated with degeneration was recorded in each compartment according to the International Cartilage Repair Society (ICRS) classification. Articular cartilage was re-examined postoperatively by arthroscopy at the time of plate removal (postoperative 16.3 ± 4.0 months in OWHTO, postoperative 17.3 ± 5.7 months in CWHTO). Cartilage repair in the medial compartment was evaluated using the staging system with modification of previous reports 6,9 : Stage 1 = no reparative change; Stage 2 = partial coverage with white cartilaginous tissue; and Stage 3 = full coverage with white cartilaginous tissue (Table 2).
Classification of articular cartilage repair.

Statistical analysis
Statistical analysis was carried out using BellCurve for Excel version 2.21 (Social Survey Research Information, Tokyo, Japan). The Mann-Whitney U test was used to compare measurements between the two different HTO procedures. Pearson’s chi-squared tests were used to test for significant differences with respect to frequency of grade classification. An adjusted p-value < 0.05 was considered significant. A power calculation indicated that a sample size of 45 in each osteotomy procedure could detect differences with an effect size of 0.2, with 5% probability of a type I error and power of 80%. The intra- and inter-rater reliabilities of radiographic measurements were assessed by calculating intraclass correlation coefficients (ICCs).
Results
Clinical and radiographic outcomes
Clinical and radiographic outcomes are summarized in Table 3. Representative radiographs are shown in Figure 2. Regarding preoperative OA grade, varus alignment, and function score, patients undergoing CWHTO showed more advanced OA than those undergoing OWHTO. The knee score and function score were significantly improved after surgery in both HTO procedures (P < 0.05), but no significant differences were found between the two procedures in the improvements of these scores. Standing aFTA was significantly decreased after surgery in both HTO procedures (P < 0.05), but there was no significant difference between the two procedures.
Clinical and radiographic outcomes.

aFTA: anatomical femorotibial angle.
The values are given as means ± standard deviation, unless otherwise stated.
* OA grade modified from Ahlbäck classification.

Pre- and postoperative radiographs of opening wedge (a) and closed wedge (b) high tibial osteotomies.
Arthroscopic assessment of articular cartilage
Representative arthroscopic images are shown in Figure 3. Evaluation of cartilage repair by the presence of newly formed cartilaginous tissue at second-look arthroscopy is summarized in Table 4. The results suggest that regenerative change was found in more than 80% of the subjects in the medial femoral condyle (MFC) and more than 60% in the medial tibial condyle (MTC). However, there were no significant differences between the two HTO procedures. The inter-rater reliability for assessment of cartilage status was substantial, with a kappa value of 0.66 (0.47–0.85). The intra-rater reliability at more than 2-month intervals was also substantial, with a kappa value of 0.79 (0.63–0.94).

Arthroscopic images of the medial compartment at first-look (a–c) and second-look arthroscopies (d–f). Case 1: Articular surface of a 72-year-old woman with preoperative Grade 4 (a) and postoperative Stage 1 (no reparative change) (d). Case 2: Articular surface of an 80-year-old man with preoperative Grade 4 (b) and postoperative Stage 2 (partial coverage with white cartilaginous tissue) (e). Case 3: Articular surface of a 70-year-old woman with preoperative Grade 4 (c) and postoperative Stage 3 (full coverage with white cartilaginous tissue) (f).
Frequency of cartilage repair stage by procedure.

The values are given as the number of knees with the percentage in parentheses.
MFC: medial femoral condyle, MTC: medial tibial condyle.
Relationship between cartilage repair status and clinical outcomes
Clinical outcomes assessed with the postoperative knee score were compared among different cartilage repair stages (Table 5). The results showed no relationship between clinical outcomes and postoperative cartilage status for both HTO procedures.
Comparison of postoperative knee scores among different cartilage repair stages.
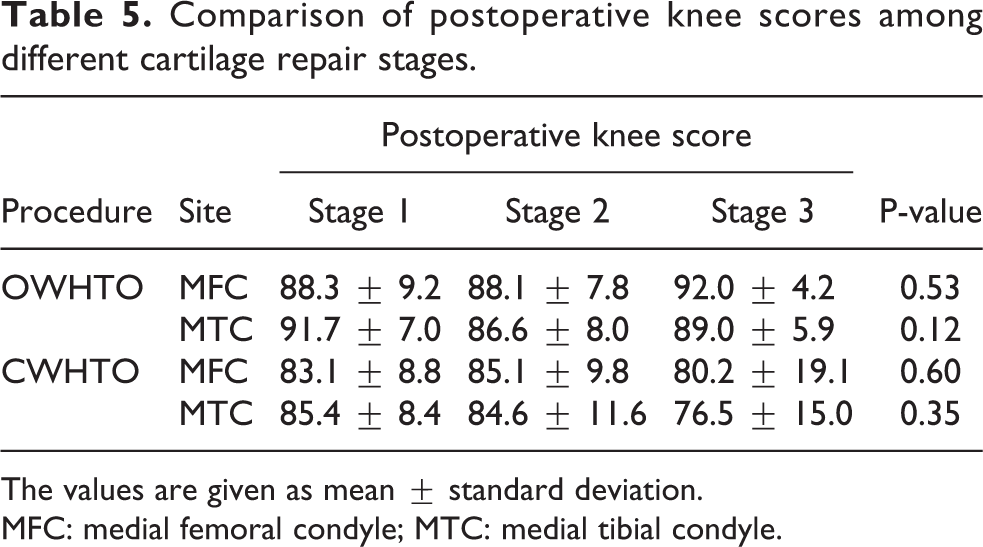
The values are given as mean ± standard deviation.
MFC: medial femoral condyle; MTC: medial tibial condyle.
Factors affecting cartilage repair after HTO
The frequency of each cartilage repair stage for each preoperative ICRS grade is summarized in Table 6. The incidence of cartilage repair was significantly higher in preoperatively advanced ICRS grade after OWHTO (P < 0.05). However, there was no significant difference in cartilage stage among preoperative ICRS grades after CWHTO. Multivariate logistic regression analysis for factors affecting cartilage repair is summarized in Table 7. The results suggest that preoperative ICRS grade was the only factor affecting cartilage repair. Age, sex, body mass index, HTO procedure, knee alignment, and clinical outcomes did not affect postoperative cartilage repair.
Frequency of cartilage repair stage in each preoperative ICRS grade

The values are given as the number of knees with the percentage in parentheses.
MFC: medial femoral condyle; MTC: medial tibial condyle.
Multivariate logistic regression analysis of factors affecting cartilage repair after HTO.

aFTA: anatomical femorotibial angle; CI: confidence interval; MFC: medial femoral condyle; MTC: medial tibial condyle; OR: odds ratio.
Discussion
The most important findings of the present study were that clinical improvement and the frequency of cartilage repair were not significantly different between OWHTO and CWHTO. The factor affecting cartilage repair was preoperative cartilage degeneration grade, regardless of HTO procedure. Cartilage repair did not affect clinical outcomes after both HTO procedures. The major advance in the present study is the comparison between two different HTO procedures of both clinical outcomes and cartilage repair.
Previous studies reported that regeneration of degenerated articular cartilage was observed in several cases after HTO without additional procedures. The incidence of complete cartilage repair after CWHTO (20–43%) 6,9,12 was relatively higher than that after OWHTO (1.6–37.5%), 5,7,8,10 although it was not directly compared between the two procedures. The variety of regeneration rates among previous reports may be due to differences in patient characteristics, surgical methods, or observation timing. This study performed a direct comparison of postoperative cartilage repair between two HTO procedures, with no significant difference in the incidence of regenerative change. Although the detailed mechanism of cartilage repair and its role are still unknown, biological remodeling was induced as a result of improvement in the mechanical environment within the knee joint. That is, an intraarticular biological response occurred in patients undergoing both HTO procedures at the same level.
The preoperative status of cartilage degeneration is a factor affecting cartilage repair. On the eburnated surface, cartilage repair was promoted by adequate lateral deviation of the mechanical axis without abrasion arthroplasty, 6,9,10 while the healing potential of fibrillated cartilage was inferior to that of eburnated bone. 12 The present study also showed that the rate of regenerative change with newly formed cartilaginous tissue was significantly higher in the advanced grade of cartilage loss with exposure of the subchondral bone. This is most likely supported by the previous studies suggesting that partial-thickness cartilage defects are harder to repair than full-thickness cartilage defects, since they are walled off from the marrow and thus have no access to macrophages, endothelial cells, and mesenchymal cells. 10,19 With regard to cartilage repair, a biological response to biomechanical change could be expected even in severe OA knees.
Although the surgical indications for OWHTO and CWHTO are still controversial, it is generally recommended that OWHTO be limited to patients with a small correction angle and no flexion contracture. 14,20 In contrast, CWHTO can also be used for medial compartmental knee OA with a large correction. For these reasons, our surgical indications differed between OWHTO and CWHTO. As a result, the preoperative OA grade and the extent of varus deformation progressed more in cases with CWHTO than with OWHTO, and a significant difference in the correction angle was found between the two HTO procedures. However, no significant differences were found in the improvement of clinical outcomes and cartilage repair between the HTO procedures. Thus, the effects of HTO on cases with advanced OA grade are comparable to those with less advanced grade, as long as surgery is performed within the inclusion criteria.
A meta-analysis of randomized, controlled trials indicated that OWHTO and CWHTO were similar with respect to coronal correction and clinical outcomes, but different in changes of the posterior slope and patellar height. 21,22 Ferner et al. introduced a unique algorithm for choosing between the HTO procedures, OWHTO or CWHTO, based on torsional deformity, patellar height, and length discrepancy. 23 In addition, a previous study investigating gait kinematics reported that OWHTO reduced knee varus moment and lateral thrust, whereas CWHTO had little effect on reducing lateral thrust. 24 Which HTO procedure should be selected based on the specific situation and clinical characteristics of each patient needs to be further elucidated.
The present study has several limitations. First, the follow-up time of 2 years, imposed by the follow-up time of arthroscopy, was not very long. The current series demonstrated only the relationship between second-look arthroscopy and short-term clinical outcomes, and it remains to be determined whether the extent of cartilage regeneration contributes to long-term clinical outcomes. Second, due to differences in OA grade of target patients, the effect of each HTO procedure on cartilage repair could not be assessed for equal severity of OA.
HTO is usually recommended for younger or early OA patients, since poor prognostic factors include severe joint destruction and advanced age. 25,26 However, the present study demonstrated that good results could be expected even in cases with severe knee OA. The extent of medial OA is not a limiting factor or contraindication for HTO. 27 The selection of HTO procedures according to the correction angle seems reasonable so far, although detailed criteria are needed to ensure the correct choice.
Conclusion
CWHTO improved clinical outcomes and cartilage status as much as OWHTO. Although the effects of cartilage repair on clinical outcomes are unknown, HTO is an effective treatment option even in patients with severe medial OA of the knee.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.